



Stomach
Gastric Dilatation and Gastric Rupture Associated with Colic in Horses
The most common cause of gastric dilatation in horses is excessive gas or intestinal obstruction. Gastric dilatation may be associated with overeating fermentable feedstuffs such as grains, lush grass, and beet pulp. Presumably, the large increase in production of volatile fatty acids inhibits gastric emptying. If untreated, gastric dilatation associated with overeating can rapidly lead to gastric rupture. If intestinal obstruction is the cause of gastric dilatation, the obstruction most often involves the small intestine. The fluid from the obstructed small intestine accumulates in the lumen of the stomach, causing gastric dilatation and retrieval of gastric reflux on passage of the nasogastric tube. Gastric dilatation also may develop in some horses with certain colonic displacements, most notably right dorsal displacement of the colon around the cecum. It is presumed that the displaced colon obstructs duodenal outflow. Gastric dilatation with fluid and gastric reflux also are characteristic findings in horses with proximal enteritis-jejunitis.
Rupture of the stomach is a fatal complication of gastric dilatation. The stomach generally tears along its greater curvature. Approximately two-thirds of all gastric ruptures occur secondary to mechanical obstruction, ileus, and trauma; the remaining cases are due to overload or to idiopathic causes.
Clinical signs associated with gastric dilatation include severe abdominal pain, tachycardia, and retching. The mucous membranes may be pale. Classically, these acute signs are replaced by relief, depression, and toxemia after the stomach has ruptured. The prognosis for survival may be excellent in most cases of gastric dilatation; however, gastric rupture is fatal.
Gastric Impaction Associated with Colic in Horses
Impaction of the stomach is an uncommon cause of colic. Although impaction of the stomach may be associated with ingestion of certain feedstuffs (eg, beet pulp, pelleted feeds, persimmon seeds, straw, barley), contributing factors (eg, diseased teeth, inadequate intake of water, and rapid eating) should also be considered. Because the incidence of gastric impaction is low, it is difficult to determine which factors may be most important. The most striking clinical sign associated with gastric impaction is severe abdominal pain. Because of the lack of other characteristic findings, the diagnosis most often is made at surgery, and the decision for surgery is based on unrelenting pain. Use of a 3-meter endoscope has made diagnosis possible without surgery.
Treatment usually involves repeated intragastric administration of carbonated drinks ("soft drinks") if the condition has been identified without surgery. If the gastric impaction is identified at surgery, saline or water can be infused into the mass through a needle passed through the wall of the stomach. After the fluid has been injected into the mass, the stomach is massaged and the obstruction broken down. If a nasogastric tube is in place at the time of surgery, water may be pumped into the stomach and the mass massaged. Gavage is continued after surgery with the hopes of removing some of the impacted material; this can be followed by feeding slurries and pasture grazing once the impaction begins to resolve. The prognosis is favorable if the diagnosis has been made without surgery or if the decision to perform exploratory surgery is made early and the impaction can be broken down manually at surgery.
Small Intestine
Clinical signs of colic may arise due to obstruction, inflammation, or strangulating obstruction of the small intestine. The prognosis for conditions affecting the small intestine is often guarded; therefore, rapid diagnosis and appropriate treatment are critical.
Ileal Impaction Associated with Colic in Horses

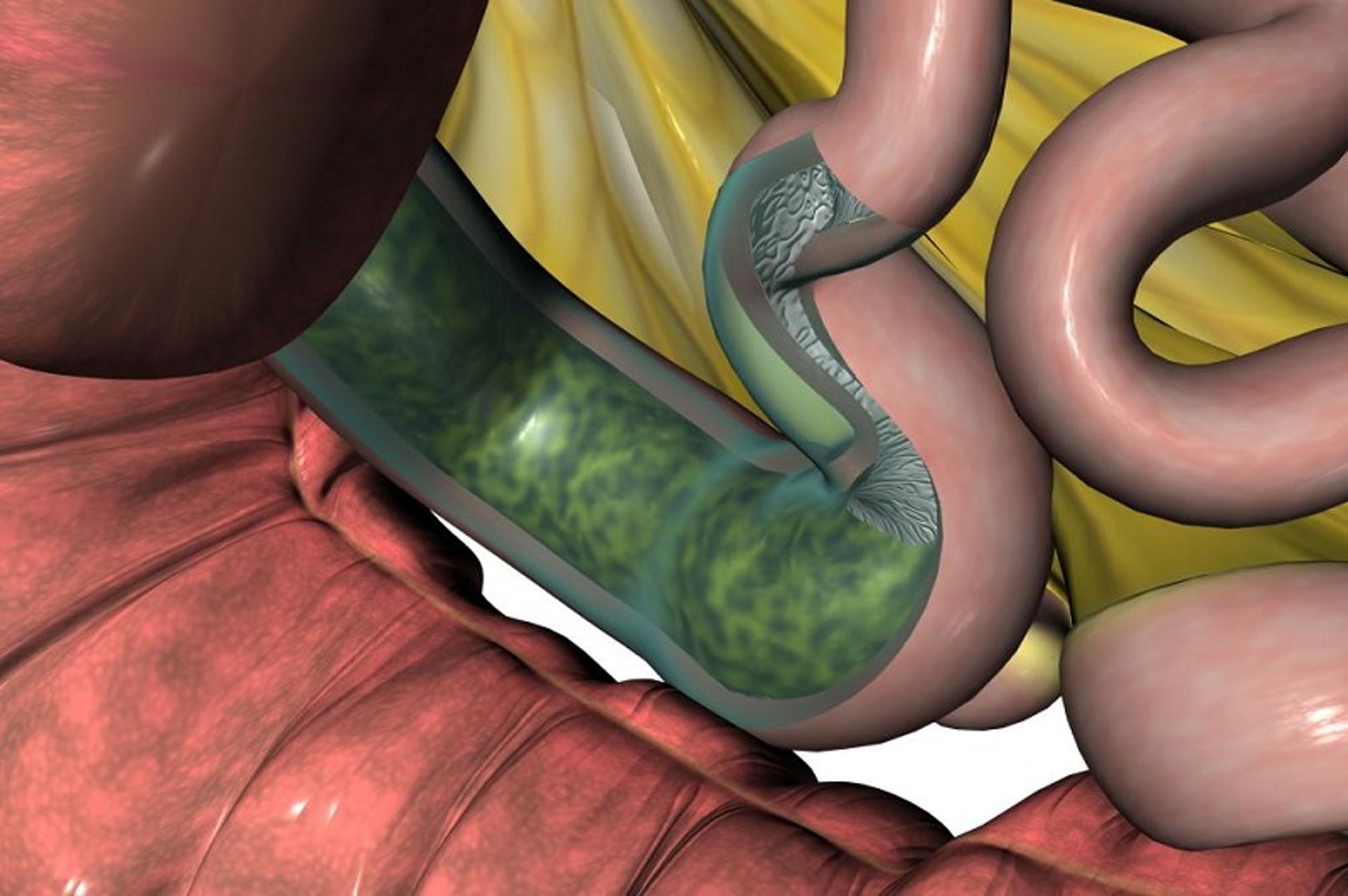
From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
The most common condition resulting in simple obstruction of the lumen of the small intestine is ileal impaction. It is most common in the southeastern US, Germany, and the Netherlands. The results of clinical studies in the UK indicate that infection with the intestinal tapeworm Anoplocephala perfoliata and ileal impaction are strongly associated. In a similar study performed in the US, two risk factors for ileal impaction were identified: 1) the feeding of Coastal Bermuda hay, and 2) the lack of administration of pyrantel pamoate, an anthelmintic with some efficacy against A perfoliata, within the 3 months preceding development of the impaction. It also has been suggested that the impaction develops secondary to spastic contractions of the ileal musculature against ingesta.
Clinical signs include the onset of mild to severe abdominal pain followed by reduced intestinal sounds, gastric reflux, and tachycardia. Although early rectal examination may permit identification of the impaction in the ileum low in the right caudal abdominal quadrant, subsequent distention of the jejunum may make this identification difficult or impossible. The most common differential diagnosis is proximal enteritis-jejunitis, and distinguishing the two conditions can often be difficult. Because the horse’s condition initially may remain stable and the abdominal pain may be mild, many horses with this condition are not referred for intensive care or surgery for >18 hours. The protein concentration of the peritoneal fluid may increase if the impaction has persisted for this long.
Patients with ileal impaction respond to treatment with fluids and mineral oil if the impaction has been identified early (ie, before gastric reflux has developed). If surgery is indicated, the impacted mass may be mixed with saline or carboxymethylcellulose and massaged into the cecum, or an enterotomy may be performed in the distal jejunum and the ingesta removed through the incision. Ileus may develop after surgery. Depending on the extent of damage to the serosal surface of the small intestine at the time of surgery, complications may develop several weeks after surgery due to intra-abdominal adhesions.
Adhesions of the Small Intestine Associated with Colic in Horses
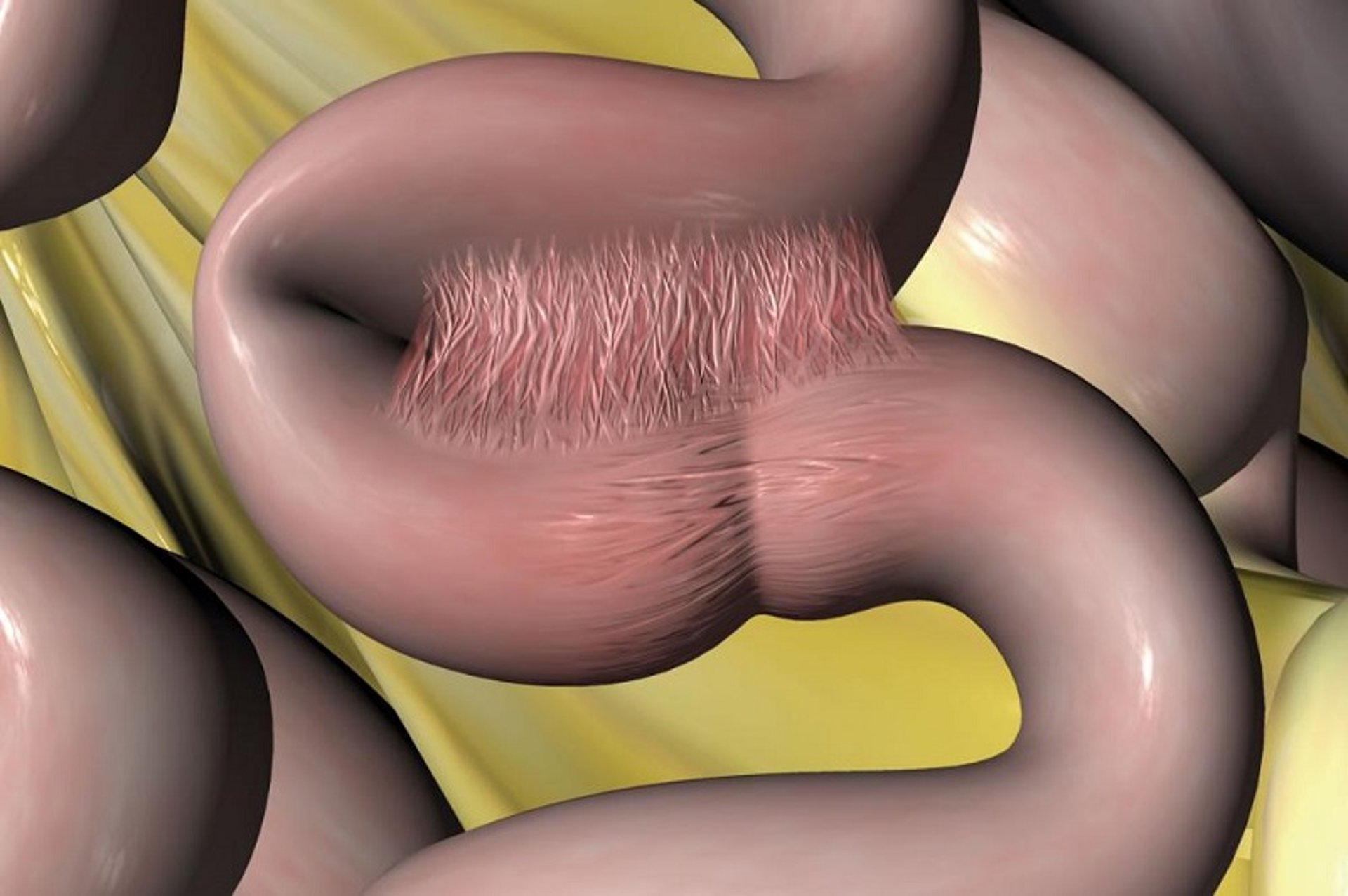
From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
Intra-abdominal adhesions generally affect the small intestine and usually cause obstruction of the intestinal lumen, although they may cause strangulating obstruction. These adhesions develop in response to peritoneal injury and, most often, are the result of previous small-intestinal surgery, chronic small-intestinal distention, peritonitis, or larval parasite migration. The tissue response to ischemia, traumatic tissue handling, foreign material, hemorrhage, or dehydration results in the formation of fibrinous (and subsequently fibrous) adhesions. Clinical signs are seen if the adhesion causes kinking, compression, or stricture of the intestine.
Adhesions should be considered if the horse has had prior abdominal surgery and a more recent history of recurrent abdominal pain. Clinical signs associated with intra-abdominal adhesions range from mild, recurrent colic to severe unrelenting pain. Most commonly, intra-abdominal adhesions cause clinical signs within 60 days of the initial surgery if they are going to be a considerable problem for the horse.
Surgical treatment involves transection of the adhesion, resection of the affected intestine, and anastomosis to achieve normal flow of ingesta. Therapeutic agents purported to reduce the subsequent formation of additional adhesions then are used. These include the systemic administration of antimicrobials and NSAIDs, and instillation of sterile carboxymethylcellulose into the abdomen at the time of closure. The owner should be informed that adhesions are likely to recur and that the longterm prognosis for patients with extensive adhesions is poor.
Ascarid Impaction of the Small Intestine Associated with Colic in Horses
Young horses, particularly those on farms with inadequate parasite control programs, may develop ascarid impactions of the small intestine. These impactions are seen after administration of an anthelmintic with high efficacy against Parascaris equorum. The anthelmintics most commonly associated with this condition are ivermectin, piperazine, and organophosphates. These drugs paralyze the ascarids, resulting in accumulation of masses of the worms in the small-intestinal lumen. It has been suggested that disruption of the surface of the ascarid releases antigenic fluids that inhibit intestinal muscular activity, thereby increasing the likelihood of intestinal obstruction.
Clinical signs range from mild to severe abdominal pain, evidence of toxemia, and gastric reflux that may contain ascarids. Ascarid impaction should be suspected if the affected horse is a weanling or yearling, in poor condition, and has a recent history of deworming. Medical treatment with fluids and intestinal lubricants may be successful in some cases. Other horses may require surgical intervention and removal of the ascarids through multiple enterotomies. The prognosis is guarded if surgery has to be performed. The owner should be advised that other young horses on the premises should be treated with anthelmintics that have lower efficacy against ascarids, such as fenbendazole. These initial treatments can then be followed with more efficacious compounds.
Proximal Enteritis–Jejunitis Associated with Colic in Horses
Proximal enteritis–jejunitis, also referred to as anterior enteritis or duodenitis–jejunitis, is a poorly understood disease that affects the proximal portion of the small intestine in horses. The disease has been recognized in the southeastern and northeastern US, England, and on the European continent. The cause is unknown, although it seems that toxins of Clostridium difficile may be involved. The affected intestine contains lesions varying from hyperemia to necrosis and infiltration of the submucosa with inflammatory cells. Often, there is edema and hemorrhage in the various layers of the intestinal wall.
Abdominal pain, ranging from mild to severe, is characteristic. When the prevalence of the disease peaked in the 1980s, it was characterized by voluminous amounts of gastric reflux, progression from pain to depression, and moderate to severe distention of the small intestine on rectal examination. In addition, the distended duodenum often was palpated as it coursed around the base of the cecum. The peritoneal fluid often contained an increased concentration of protein (>3 g/dL) with a normal number of WBCs; however, this finding did not consistently distinguish proximal enteritis–jejunitis from other causes of small-intestinal disease. Based on anecdotal reports, the prevalence and clinical severity of the disease have decreased, at least in regions of the US where it characteristically had a more severe course and was accompanied by a high incidence of laminitis.
Treatment may be either medical or surgical. Medical treatment includes continued gastric decompression until the gastric reflux abates, intravenous fluids, and analgesics, as required. Many clinicians administer penicillin and low doses of flunixin meglumine; some also administer neostigmine, lidocaine, or metoclopramide to stimulate small-intestinal motility. Some surgeons, particularly in the UK, believe exploratory laparotomy and intestinal decompression result in a more rapid recovery. The survival rate associated with proximal enteritis–jejunitis is reported to be 44%. The horse's feet should receive particular attention because acute laminitis has been reported as a common complication, with a prevalence of ~25%.
Intussusception of the Small Intestine Associated with Colic in Horses


Courtesy of Dr. Sameeh M. Abutarbush.
Most intussusceptions that develop in horses are jejuno-jejunal, ileal-ileal, or ileocecal. The length of intestine that has become invaginated (the intussusceptum) into the more distal segment of intestine (the intussuscipiens) may range from a few centimeters to as much as a meter. Although the precise cause of most intussusceptions remains speculative, alterations in peristalsis due to enteritis, surgical trauma, parasite damage, anthelmintics, and Anoplocephala perfoliata infection have been suggested. Horses < 3 years old are affected most commonly.

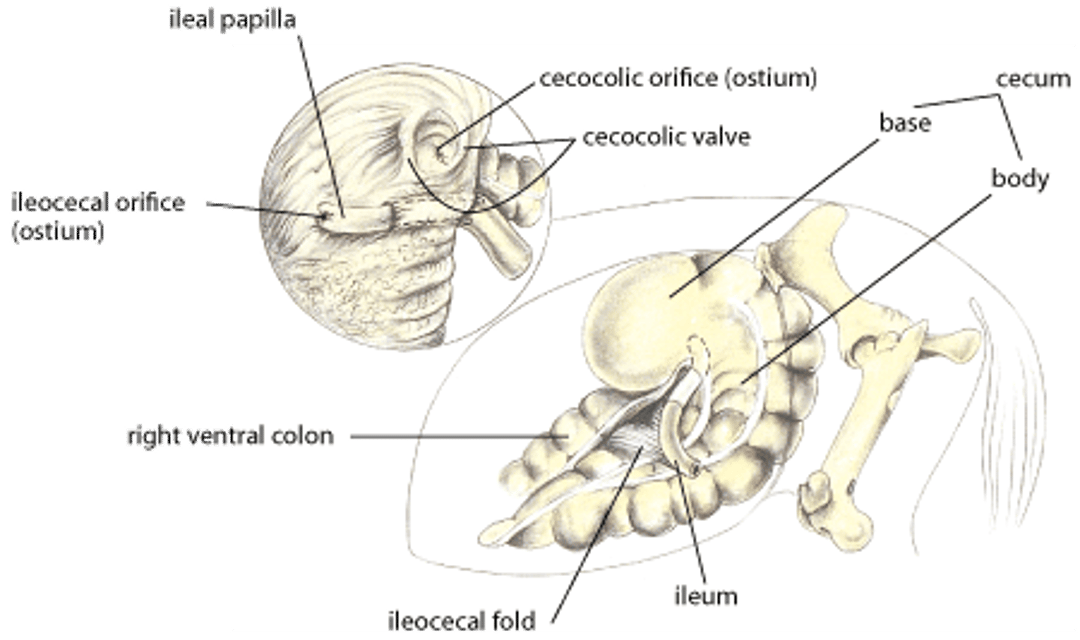
Illustration by Dr. Gheorghe Constantinescu.
Abdominal pain may be either acute due to complete obstruction of the intestinal lumen or chronic due to partial occlusion of the lumen. If the occlusion of the intestinal lumen is complete, the horse is acutely painful and has gastric reflux, and distended loops of small intestine are palpable per rectum. It may be possible to palpate the turgid intussusception, especially if the ileum is involved. Because the strangulated intussusceptum is contained within the intussuscipiens, the WBC count in the peritoneal fluid may not reflect the extent of intestinal damage.
Treatment requires surgery to reduce the intussusception, if possible, followed by resection and anastomosis. Because of the edema and hemorrhage in the wall of the affected intestine, it may be difficult to assess the viability of the bowel. Additionally, the damage to the intussusceptum may result in the development of adhesions. If the jejunum is involved, a jejuno-jejunal anastomosis must be performed. If the intussusception involves only the ileum, the affected intestine must be resected and a jejuno-cecal anastomosis performed. If the ileum has invaginated into the cecum, the terminal portion of the ileum should be transected close to the cecum and a jejuno-cecal anastomosis performed. The prognosis for survival is good if surgery is performed before the intussusception has become irreducible; if it is performed after, the prognosis is fair to poor because of the development of peritonitis, ileus, adhesions, and abscess formation.
Volvulus of the Small Intestine Associated with Colic in Horses
A small-intestinal volvulus occurs when the intestine rotates on its mesenteric axis >180°. As the degree of the rotation increases, the vascular supply to the intestine is lost. Presumably because of its attachment to the cecum, the distal aspect of the volvulus is the ileum in most cases.
Horses with small-intestinal volvulus have acute pain and an increased heart rate, a prolonged capillary refill time, and gastric reflux. Because of the loss of fluid into the intestine and stomach, these horses rapidly become dehydrated and have increased PCV and plasma protein concentrations. The horse’s status may deteriorate rapidly because of hypovolemia and endotoxemia. Rectal examination generally reveals turgid distended loops of small intestine, and the peritoneal fluid contains increased numbers of WBCs and high concentrations of lactate and protein.

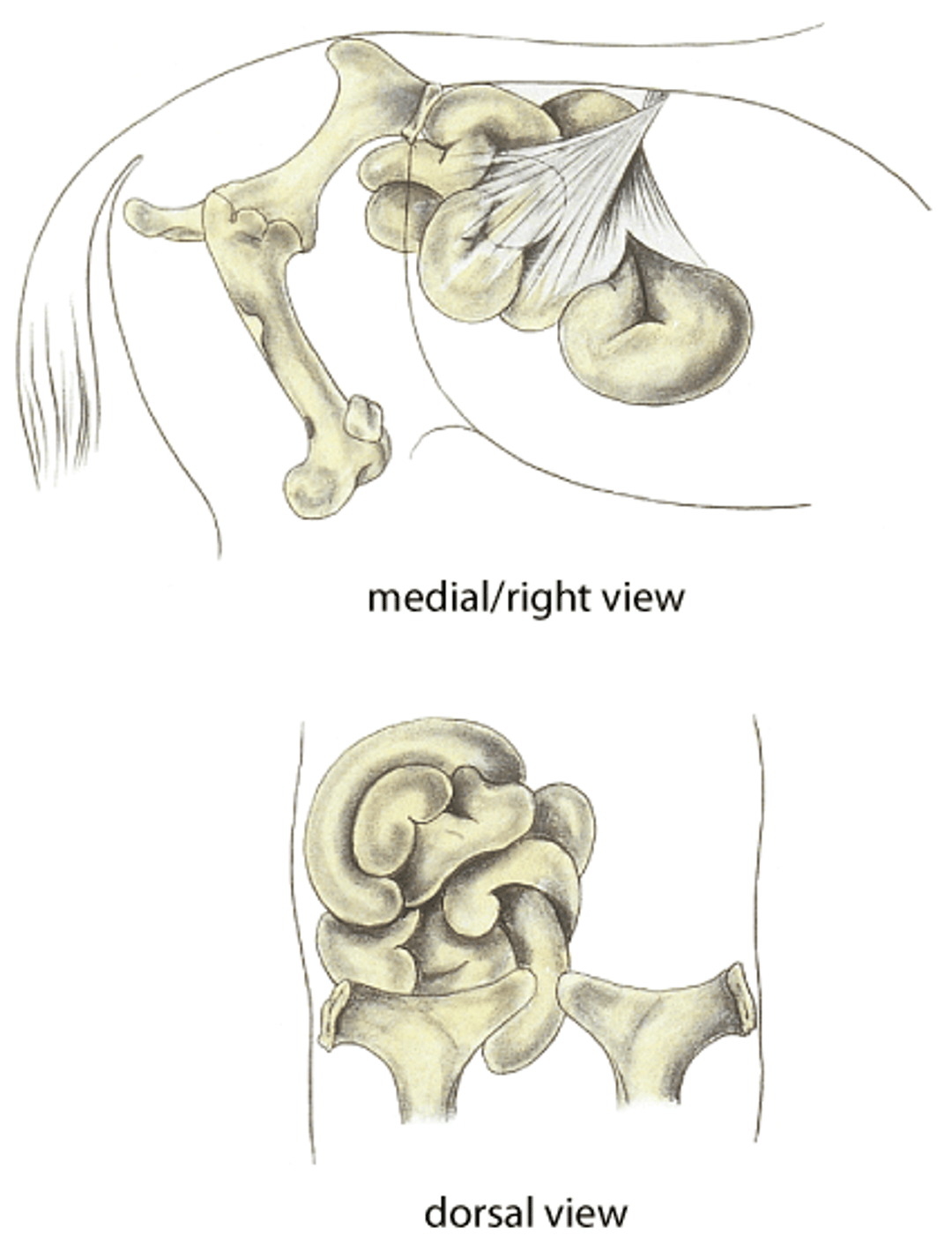
Illustration by Dr. Gheorghe Constantinescu.
Treatment involves surgical correction of the volvulus via a ventral midline celiotomy. If the intestine is nonviable, it must be resected and an anastomosis performed. The prognosis for survival depends on the duration of illness and amount of intestine that must be resected. Prognosis is good with early detection and surgery. Horses with a longer period of illness preoperatively, or those that develop postoperative ileus and peritonitis, are at increased risk of adhesion formation. It has been suggested that euthanasia is warranted if >50% of the length of the small intestine must be removed. However, results of an experimental study in ponies indicated that removal of 70% of the small intestine did not result in malabsorption provided the ponies were fed several (8) small, pelleted meals each day.
Pedunculated Lipomas Associated with Colic in Horses
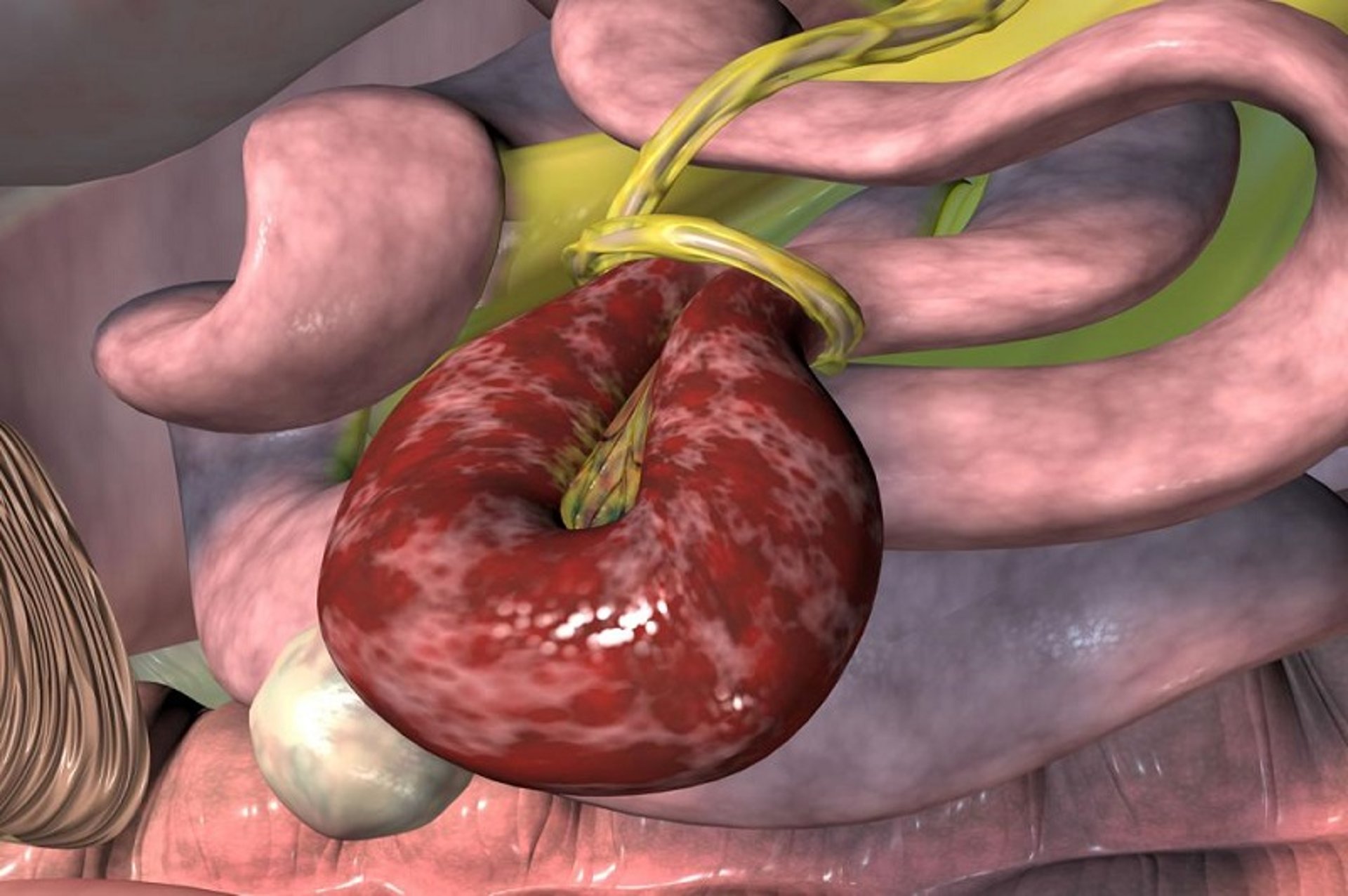
From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
Colic due to pedunculated lipomas occurs most often in horses >10 years old. Pedunculated lipomas are suspended from the mesentery by a stalk or pedicle, which wraps around a segment of intestine, occluding the lumen of the intestine and interfering with its blood supply. The lipoma frequently forms a knot with the pedicle.


Courtesy of Dr. Sameeh M. Abutarbush.
Clinical signs range from depression to severe abdominal pain, gastric reflux, and rapid deterioration in metabolic status. Distended loops of small intestine are palpable on rectal examination and can be identified with abdominal ultrasonographic evaluation; the lipoma can be felt per rectum in rare cases. The peritoneal fluid contains an increased number of WBCs and RBCs and increased concentrations of protein and lactate.
Treatment requires transection of the pedicle and, if necessary, resection of the devitalized intestine. The prognosis depends on the time between onset of clinical signs and surgery. If surgery is performed early, the prognosis is good; however, if surgery is not performed until signs of cardiovascular deterioration are present, the prognosis for survival is fair to poor.
Internal Incarceration Associated with Colic in Horses
The most common sites for internal incarcerations are mesenteric rents and the epiploic foramen. Mesenteric rents are defects in the small-intestinal mesentery. Problems develop when a segment of small intestine passes through the mesenteric defect, and the intestine becomes incarcerated. Because the intestine distends with fluid and blood, volvulus of the affected segment frequently occurs. Mesenteric rents causing intestinal incarceration occur in horses of all ages.
From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
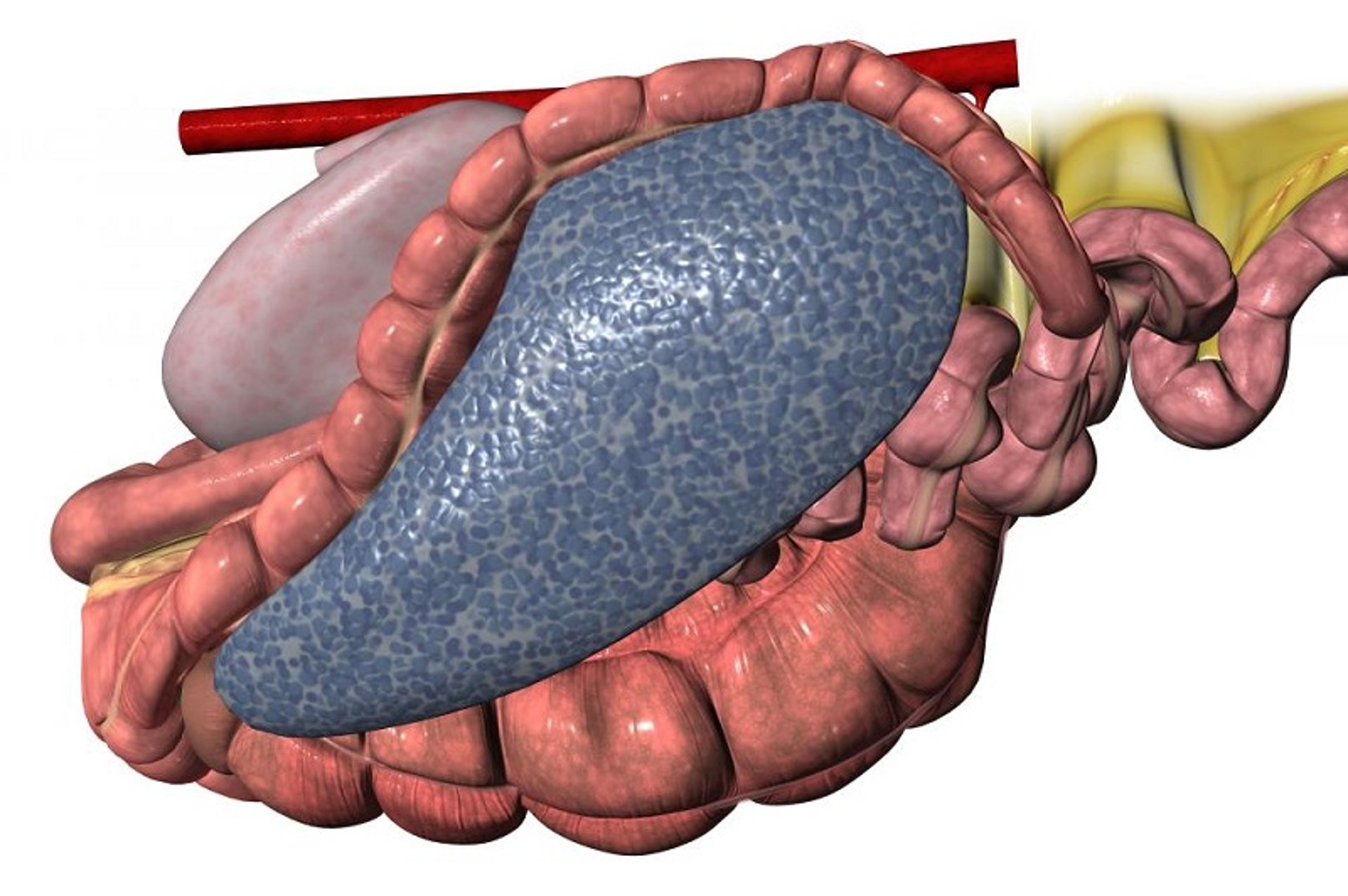
The epiploic foramen is a natural opening bounded by the caudate lobe of the liver, the portal vein, and the caudal vena cava. The distal jejunum and ileum are the most common portions of the intestine that become incarcerated through the epiploic foramen. Although, typically, the intestine passes through the epiploic foramen from left to right, tearing the omentum in the process, it also may pass in the opposite direction to enter the omental bursa. It has been reported that horses >7 years old are affected most frequently by epiploic foramen entrapment. However, the condition also has been reported in horses < 7 years old. The condition is notably associated with windsucking or cribbing.
Clinical signs may be vague and similar to those of horses with proximal enteritis or pedunculated lipomas. The diagnosis may have to be made at surgery. Furthermore, in some cases, because of the position of the affected intestine within the omental bursa, the peritoneal fluid available for analysis may be normal.
Treatment of horses with either mesenteric rents or epiploic foramen entrapments is surgical. The affected segment of intestine must be exteriorized, its viability evaluated, and, if necessary, a resection and anastomosis performed. The prognosis for survival depends on the time between onset and surgery. If surgery is performed early in the course of the disease, the prognosis is good. However, because the clinical signs may be vague, the decision to perform surgery may be delayed, worsening the prognosis. Laparoscopic techniques have been developed to evaluate and close the space with mesh.
Inguinal Hernia Associated with Colic in Horses
Inguinal hernias generally develop in stallions after breeding a mare, trauma, or a hard workout. Hernias appear to be most common in Tennessee Walking Horses, American Saddlebreds, and Standardbreds. In most cases, the hernia results in acute colic. The intestine descends through the vaginal ring in most cases and lies next to the testis and epididymis. Physical examination reveals a swollen testis that is firm and cool to the touch. If the hernia has occurred within hours, the intestine may be palpated in the inguinal canal. In this situation, an attempt may be made to reduce the hernia by pulling down on the testis to tighten the boundaries of the inguinal canal and then forcing the intestine up toward the vaginal ring. Once the incarcerated intestine, which frequently includes the ileum, has become edematous, it is not possible to reduce the hernia manually. Rectal examination will reveal distended loops of small intestine, with one of the loops tracing to the vaginal ring on the affected side. There will be gastric reflux, and the patient’s condition will deteriorate rapidly. Peritoneal fluid generally reflects the extent of ischemia.
Surgery involves a ventral midline celiotomy and inguinal approach to reduce the hernia. Often, the testicle on the affected side must be removed and the affected intestine resected. The prognosis for survival seems to be breed-dependent, with Standardbred horses having a good prognosis and Tennessee Walking Horses having a fair to poor prognosis. This is presumably because many Tennessee Walking Horse stallions with inguinal hernias show few clinical signs of pain, which delays the decision for surgery.
Cecum and Large Intestine
Impaction of the Cecum and Large Intestine Associated with Colic in Horses
The most common sites of impaction are the pelvic flexure region of the left colon, the junction of the right dorsal colon with the transverse colon, and the base and body of the cecum. The pelvic flexure and transverse colon regions are anatomically predisposed to obstruction because of the dramatic changes in size. The underlying reason for impaction of the cecum is unknown, although it has been speculated that cecal muscular activity is abnormal in affected horses. Other predisposing factors include feed that is too coarse, diseased or poorly managed teeth, and insufficient water intake.
In one clinical study, Morgan, Arabian, and Appaloosa breeds were overrepresented among horses with cecal impaction, and it has been proposed that the condition may develop secondary to infection with the tapeworm Anoplocephala perfoliata. Impactions also may develop secondary to other intestinal diseases and may be associated with prolonged hospitalization. Consequently, the fecal output of horses being treated for other abnormalities should be assessed on a routine basis. This is especially important in horses being administered NSAIDs on a daily basis.

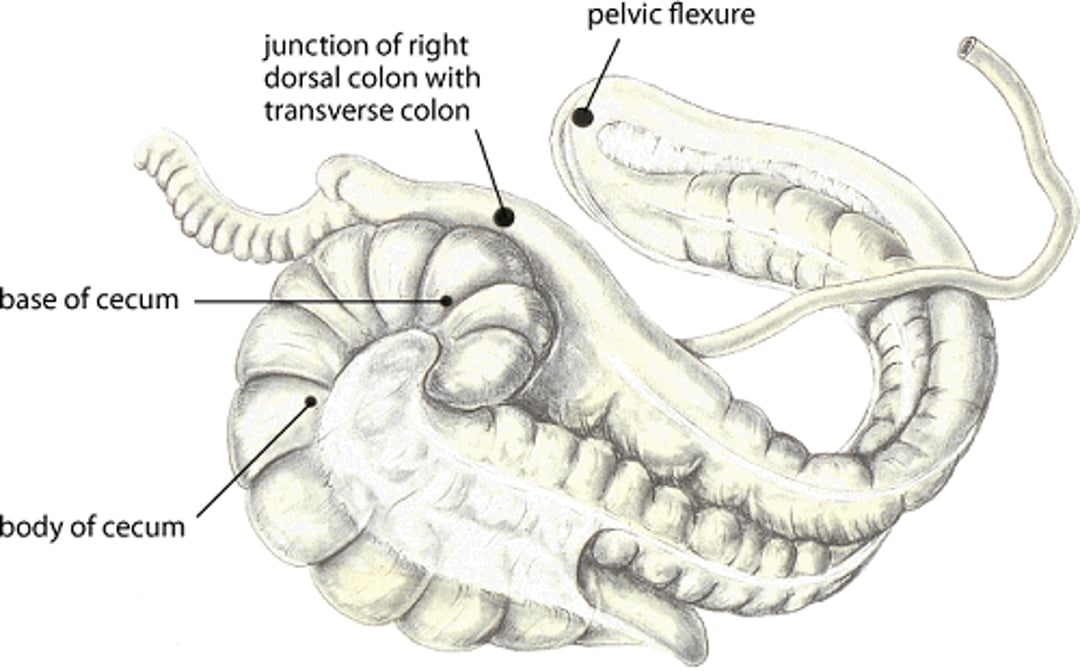
Illustration by Dr. Gheorghe Constantinescu.
Horses with simple impactions of the cecum or large colon exhibit mild intermittent signs of colic, and there is minimal evidence of systemic deterioration unless the impaction has a prolonged course. Generally, the heart rate is only slightly increased. Intestinal sounds are usually heard on auscultation of the abdomen and may be associated with the onset of pain as the affected portion of the intestine contracts against the obstruction. Diagnosis is made on rectal examination. Although the most common site of obstruction is considered to be the pelvic flexure region of the large colon, the impacted ingesta actually fills much or all of the left ventral colon. The impacted mass may be felt extending cranially in the abdomen, and the affected segment of bowel is identified by palpating the longitudinal bands on the surface of the ventral colon. Impaction of the cecum is relatively easy to identify, because the mass is situated in the right paralumbar region. The cecum can be definitively identified by palpating the taut ventral cecal band and the fat and blood vessels overlying the medial cecal band. Peritoneal fluid analysis may be normal, or the total protein concentration may be increased as the course becomes more prolonged.
Cecal impactions tend to cause colic in horses >8 years old. Alternatively, impactions may be seen in horses hospitalized for other reasons and are often associated with abrupt rupture of the cecum in these cases. Consequently, there is some controversy regarding the best method of treatment. Because medical treatment in some clinical studies has been unsuccessful in 50% of cases, surgical removal of the impacting mass followed by an ileocolostomy has been strongly recommended. Other veterinarians report good results with aggressive medical treatment, particularly if abdominal pain associated with the cecal impaction was the primary reason the patient required veterinary attention.
Medical treatment of horses with cecal or large-colon impaction involves the administration of analgesics as necessary, large volumes of balanced intravenous fluids, and intragastric administration of either mineral oil or dioctyl sodium sulfosuccinate and water. Feed should be restricted until the impaction is relieved. Many veterinarians consider aggressive fluid therapy (eg, >50 L of fluid/day to a horse weighing 450 kg) to be the mainstay of treatment. Balanced electrolyte solutions are administered to induce movement of fluid from the plasma into the lumen of the intestine and continued until the impaction is resolved.
Interest has increased in using enteral fluid therapy to treat horses with impactions, primarily because enteral fluid therapy is substantially less expensive than intravenous fluid therapy. The clinical results with enteral fluid therapy have been rewarding, and the results of experimental work in healthy horses have shown that enteral fluid therapy is more effective than intravenous fluid therapy in promoting hydration of colonic contents.
If the large-colon impaction does not resolve with medical management, surgery can be performed. Typically, the impaction is approached via a ventral midline celiotomy, with the affected portion of the colon gently exteriorized and positioned on a sterile colon tray. An enterotomy then is made in the pelvic flexure and the contents of the colon removed.
Surgery for treatment of cecal impactions requires general anesthesia, a ventral midline celiotomy, isolation of the cecum from the celiotomy site, and removal of the contents of the cecum via an enterotomy. Because impactions have recurred after simple evacuation, some surgeons prefer to bypass the cecum with an ileocolostomy.
The prognosis associated with impactions involving the large colon is excellent, with a survival rate of >95%. The survival rate associated with cecal impactions is ~80% for those horses that can be treated medically and 60%–70% for those horses requiring surgical intervention.
In some geographic areas, the offending material may be sand, especially if the amount of pasture grass is insufficient and the horses are fed on the ground. The sand accumulates in the right dorsal colon and transverse colon. Intermittent signs of abdominal pain may occur because of the weight of the sand in the intestine. More severe signs of pain occur when the impaction occludes the lumen of the transverse colon. Under such circumstances, the colon proximal to the obstruction distends with gas, resulting in extreme pain. It may not be possible to distinguish this condition from an intestinal displacement or volvulus. Sand also may be identified in the feces by mixing fecal material with water in a transparent rectal examination sleeve.
Treatment of sand impaction may be either medical or surgical. Medical treatment generally involves intragastric administration of psyllium (400 g/500 kg body wt, daily for 7 days) to purge the sand from the lumen. The psyllium flakes are added to 7.5 L of warm water and rapidly pumped into the stomach. These treatments are accompanied by analgesics as needed and intravenous fluids to promote movement of fluid into the intestinal lumen.
Surgery via a ventral midline celiotomy is necessary if the sand completely obstructs the lumen of the transverse colon. The left colon is exteriorized on a sterile colon tray, and the sand is removed via an enterotomy. The prognosis is usually good. Problems sometimes develop during surgery if the colon was damaged due to the extensive weight of the sand or while the sand is being removed from the intestine (Also see Sand Enteropathy in Horses).
Enterolithiasis Associated with Colic in Horses
Enteroliths are concretions of magnesium ammonium phosphate crystals that form around a nidus (eg, wire, stone, nail). Enteroliths may occur singly or in groups and are commonly causes of colic in horses in certain parts of the US, including California, the southwest, Indiana, and Florida. Enterolithiasis commonly affects Arabian horses, but the popularity of these horses in the aforementioned areas confounds the question regarding breed association. Most horses with enteroliths are ~10 years old; enterolithiasis rarely occurs in horses < 4 years old. Although not all factors that contribute to the formation of enteroliths have been identified, results of clinical studies indicate that large-colon contents from horses with enteroliths have higher mineral (magnesium, calcium, and phosphorus) concentrations and pH than contents from horses with colic not due to enteroliths. A common factor associated with enterolithiasis is the consumption of alfalfa hay, which results in a higher pH and increased concentrations of calcium, magnesium, and sulfur in the large colon.
From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
Many horses with enterolithiasis have a history of recurring colic, presumably indicating that the enterolith(s) previously had caused partial or temporary obstruction of the colonic lumen. If the enterolith becomes lodged at the origin of the transverse colon, the colon proximal to the obstruction distends with gas and the pain is severe. Distention of the abdomen may be marked. Heart and respiratory rates are increased, and the mucous membranes may be pale or pink. Generally, colonic and cecal distention is evident on rectal examination; however, the mass rarely is palpable because the transverse colon is cranial to the cranial mesenteric artery. Analysis of the peritoneal fluid is usually within normal limits unless ischemia of the colonic wall has developed over the enterolith. In areas where the problem is endemic, radiography may be used to identify the enteroliths.
Treatment involves surgery via a ventral midline celiotomy to decompress the colon and cecum and then to remove the stone(s). The left portion of the large colon is exteriorized and positioned on a sterile colon tray, the ingesta removed via an enterotomy, and then the enterolith(s) removed. If the stone has a flat side or a polyhedral shape, this is indicative of the presence of one or more additional enteroliths. Consequently, the rest of the large and small colons must be thoroughly checked for other stones. The prognosis is excellent, with practices in endemic areas reporting survival rates of 95%.
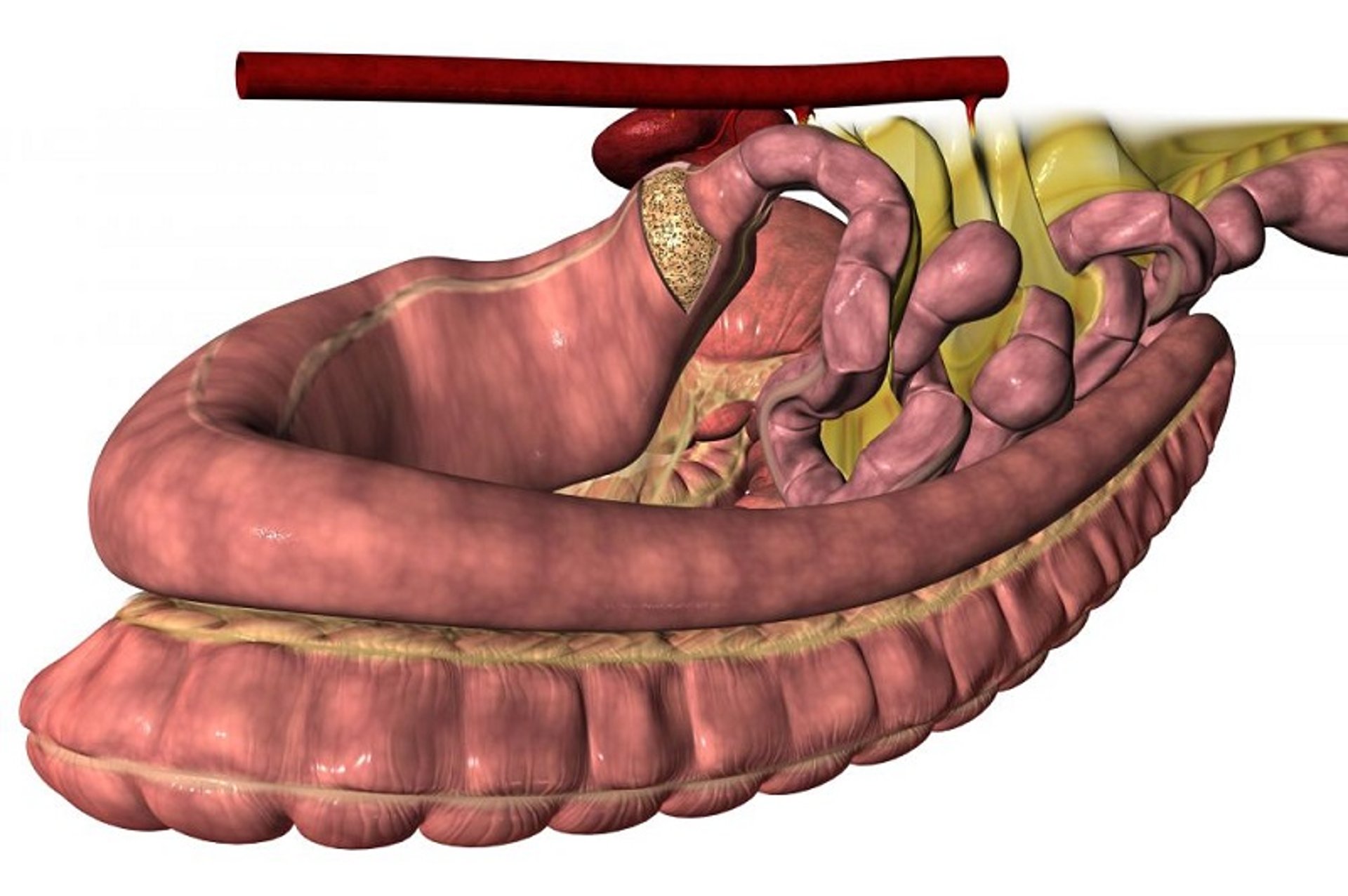
Left Dorsal Displacement of the Colon Associated with Colic in Horses
From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
Left dorsal displacement of the colon occurs when either the pelvic flexure or the entire left colon becomes displaced over the renosplenic ligament. Because the renosplenic ligament is not attached to the most dorsal aspect of the spleen, a natural cleft exists between the spleen and left kidney. Although all ages and sexes of horses are affected equally, results of a clinical study indicate that the displacement is common in young horses.

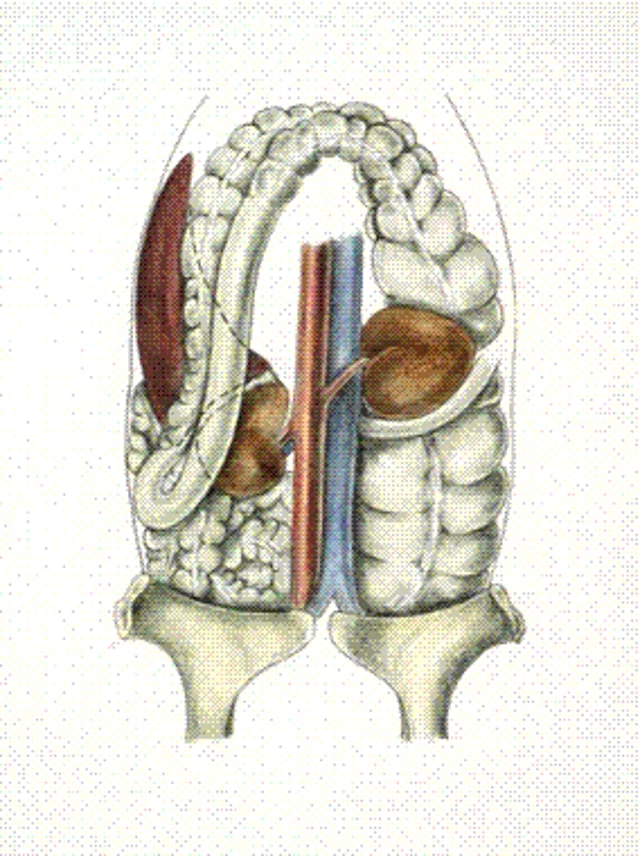
Illustration by Dr. Gheorghe Constantinescu.
Because left dorsal displacement results in simple obstruction of the colon at the point where it hangs across the ligament, the condition usually is associated with moderate abdominal pain or a prolonged course of intermittent painful episodes. The mucous membranes remain normal, and the heart rate is increased only slightly. The diagnosis usually is made on rectal examination (palpating the pelvic flexure over the ligament, palpating the bands of the left ventral colon running dorsocranially to the left kidney, and detecting that the spleen is displaced toward the middle of the abdomen). The condition also may be identified via ultrasonographic examination. A paracentesis may yield blood if the spleen is engorged and displaced toward the midline.
Four forms of treatment have been used:
withholding feed to determine whether evacuation of the intestinal contents will allow the colon to return to its normal position
rolling the patient to dislodge the colon from the ligament
administering phenylephrine and/or jogging the patient to cause splenic contraction and correction of the displacement
performing surgery to return the colon to its correct position; the rolling procedure involves short-term anesthesia (generally xylazine or detomidine and ketamine), elevation of the horse’s hindlimbs, and rolling the horse 360°
Surgery is performed via a ventral midline celiotomy. The advantage of surgery is that the viability of the colon can be assessed. Phenylephrine should not be administered to horses >15 years old because of the increased risk of fatal hemorrhage in aged horses treated with this drug. If left dorsal displacement of the colon recurs, the renosplenic space may be sutured closed laparoscopically. Overall, the prognosis is good, with survival rates >80% reported in most studies.
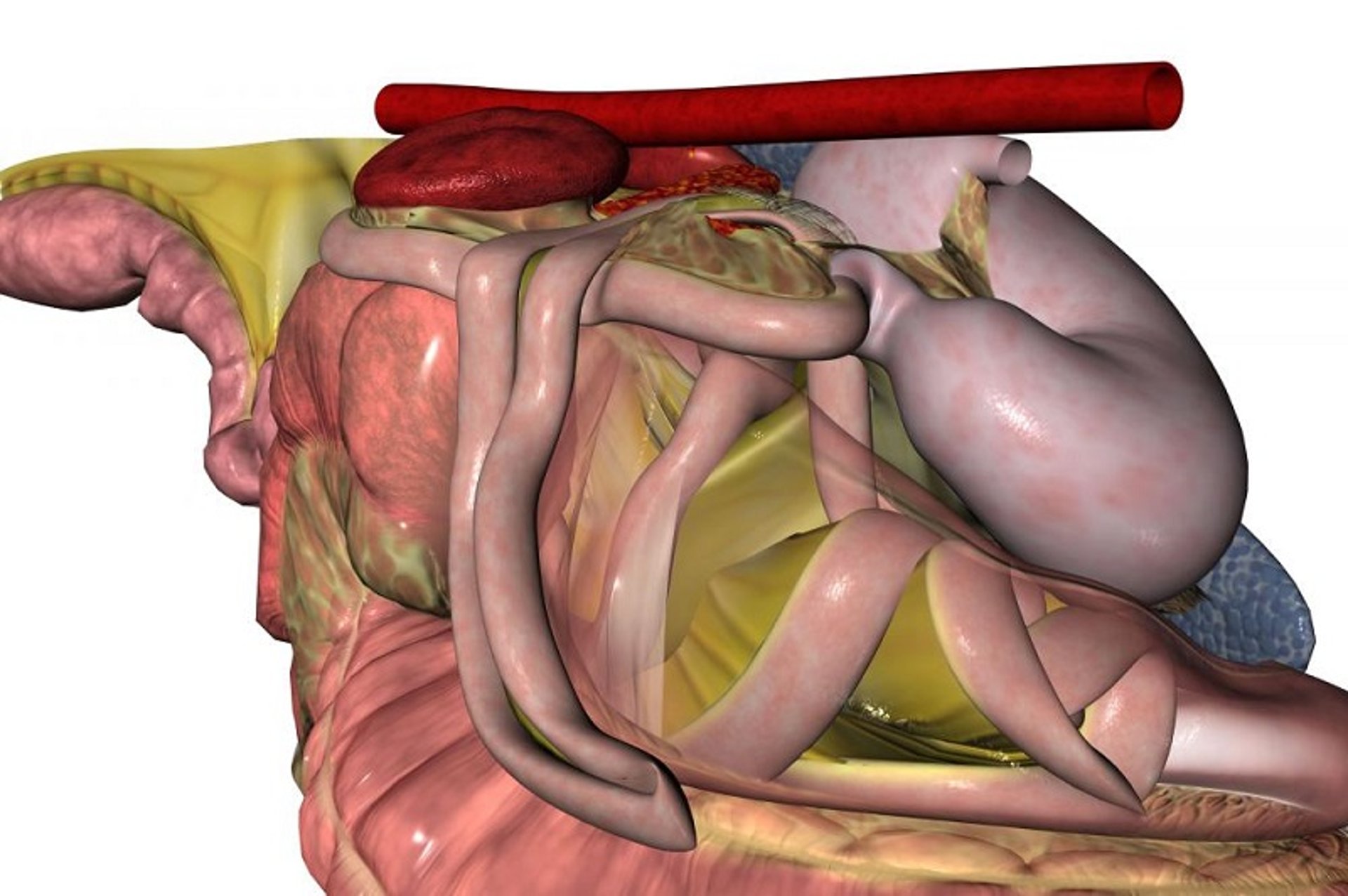
Right Dorsal Displacement of the Colon Associated with Colic in Horses

From The Glass Horse: Equine Colic CD, courtesy of www.sciencein3D.com.
In horses with right displacement of the ascending colon, the left colons move laterally around the base of the cecum to lie between the cecum and the right body wall. With the most common form of this displacement, the pelvic flexure ends up positioned near the diaphragm. In many instances, the displacement may be complicated by twisting of the colon near the base of the cecum. Although there may be some interference with venous drainage from the affected colon, usually the arterial supply remains intact.

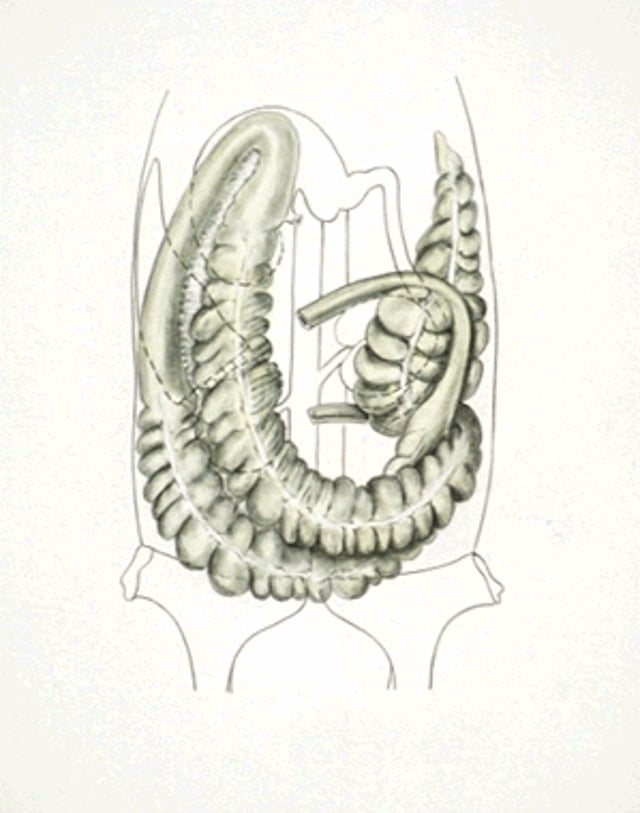
Illustration by Dr. Gheorghe Constantinescu.
Most horses with right dorsal displacements exhibit moderate degrees of pain, and there is slow development of systemic deterioration. In some cases, however, the pain may be severe. Rectal examination may reveal the taenia of the colon running transversely across the pelvic inlet. It may not be possible to palpate the ventral cecal band on rectal examination. Some horses with this condition have gastric reflux, presumably due to occlusion of the lumen of the duodenum.

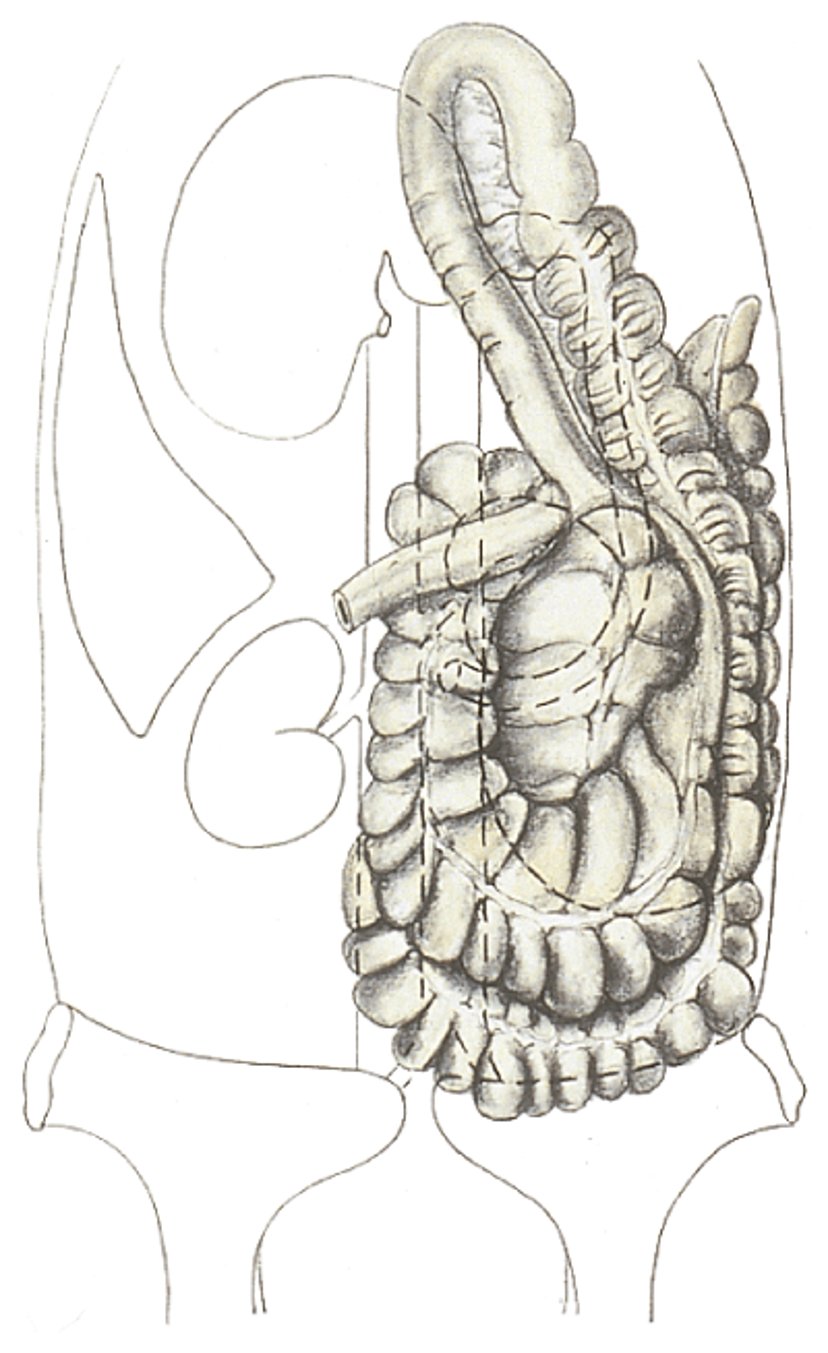
Illustration by Dr. Gheorghe Constantinescu.

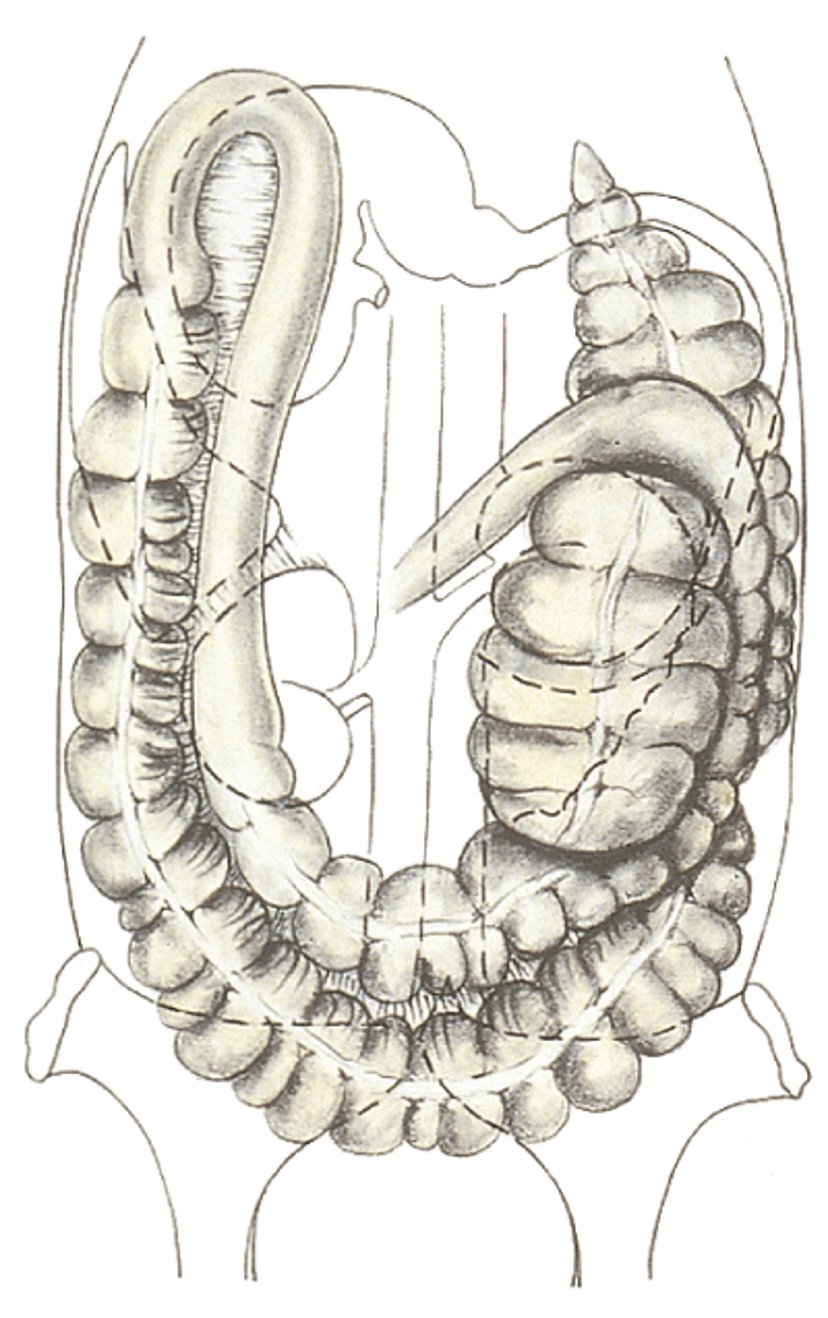
Illustration by Dr. Gheorghe Constantinescu.
Some horses with this condition appear to be stable and may show intermittent signs consistent with mild abdominal pain. Treatment may be conservative, involving attention to fluid needs and administration of mild analgesics. For painful horses, however, surgery must be performed to locate the pelvic flexure, to exteriorize and decompress the left portion of the colon, if possible, and then to relocate the colon to its normal position by rotating it around the cecal base. The twisting of the colon must be identified and corrected. The prognosis for survival is good, provided that the colonic wall is not damaged during surgery.
Right Dorsal Colitis Associated with Colic in Horses
Right dorsal colitis has been recognized with increasing regularity in recent years, particularly, but not only, in horses administered excessive amounts of NSAIDs. Because the condition has been diagnosed in horses receiving recommended doses of these drugs, it seems that some horses are particularly sensitive to their toxic effects. The drug most commonly associated with right dorsal colitis is phenylbutazone, but this may reflect the common and often chronic use of this drug. The most common lesions reported in horses with right dorsal colitis are ulceration and thickening and/or fibrosis of the wall of the right dorsal colon.
Horses commonly present with abdominal pain, anorexia, and lethargy. In many cases, the signs are consistent with severe abdominal pain, fever, endotoxemia, and diarrhea. Horses with the more chronic form of the disease present with intermittent abdominal pain, weight loss, lethargy, and anorexia. In most cases, hypoproteinemia is a common finding on hematologic evaluation and may account for ventral edema in some horses with the chronic form of the disease. The diagnosis is usually based on the history, clinical signs, and hematologic findings. In some cases, ultrasonographic evaluation of the colon via the twelfth to fifteenth intercostal spaces may provide evidence of marked thickening of the wall of the right dorsal colon.
Treatment of affected horses includes discontinuation of NSAIDs, rest, and a change in diet to a complete pelleted feed that contains ≥30% dietary fiber. Some veterinarians recommend feeding many small meals daily, many recommend the inclusion of psyllium to promote mucosal healing, and some administer sucralfate or metronidazole. Horses with uncontrollable pain may require surgery to resect or bypass the affected portion of the right dorsal colon. The prognosis for horses with right dorsal colitis is guarded.
Volvulus of the Large Colon Associated with Colic in Horses
Although the term “torsion” has been used for years to indicate that the colon has twisted on itself, the involvement of the mesentery between the ventral and dorsal colons indicates that the condition is a volvulus. When viewed from the most common site of the volvulus (the junction between the right ventral colon and the cecum), the volvulus most often occurs in a clockwise direction; the cecum may or may not be involved. If the volvulus is < 270°, there may be obstruction of the bowel lumen without ischemia. If the volvulus is >360°, there is strangulating obstruction of the entire left colon.
The onset of colic is sudden, and the pain may be mild to moderate if the volvulus results only in obstruction of the intestinal lumen. When the twist is more extensive, the pain is severe and the horse may not respond to analgesics. The colon is extremely enlarged, and the mesentery between the dorsal and ventral colons is edematous on rectal examination. The heart rate is rapid, peripheral perfusion is poor, and the horse’s condition deteriorates rapidly. Distention of the abdomen usually is marked. Generally, results of peritoneal fluid analysis and the extent of colonic involvement are poorly correlated.

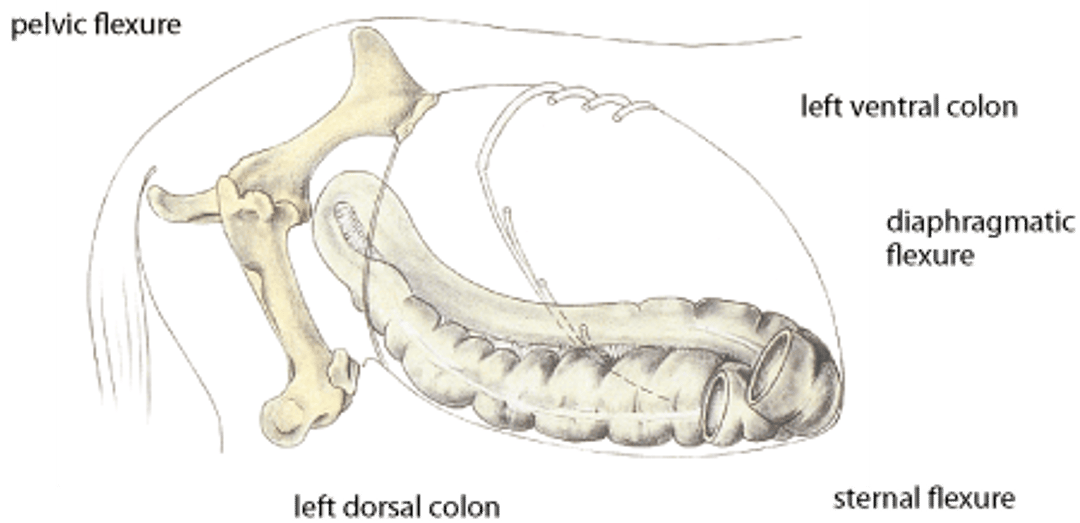
Illustration by Dr. Gheorghe Constantinescu.

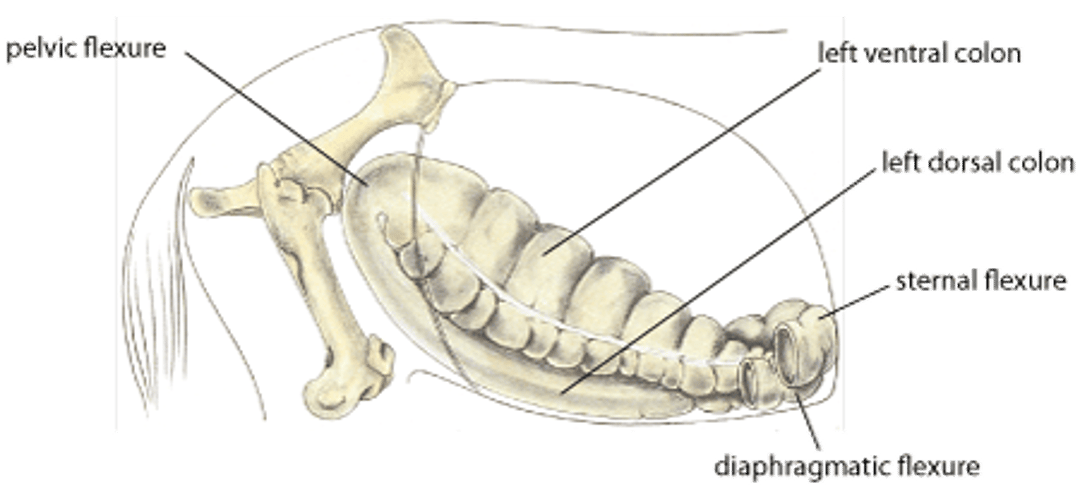
Illustration by Dr. Gheorghe Constantinescu.
Although the cause of colonic volvulus remains unknown, it is presumed to be associated with a disproportionate amount of gas in the colon. On broodmare farms, the condition frequently is associated with recent (within 90 days) or impending parturition, a grass diet, or highly fermentable feeds. The presence of a foal at the mare’s side (history of recent parturition) is an additional risk factor.
Treatment of colonic volvulus requires surgery to correct the volvulus and remove affected bowel, if necessary. Although the technique for removal of 90% of the colon has been perfected in healthy horses, extreme difficulty can be encountered if the colon is edematous. Because the recurrence rate has been estimated to be as high as 20% in some clinical studies, colopexy procedures have been devised to reduce the recurrence of the condition in broodmares. Although a survival rate of 27% was reported in a study involving several university hospitals, survival rates >85% are common for practices situated near broodmare farms.
Impaction and Foreign Body Obstruction of the Descending Colon Associated with Colic in Horses
Abnormalities involving the descending (small) colon are infrequent, accounting for < 5% of conditions characterized by colic in one study. The more common causes include meconium retention, impaction, and foreign body obstruction. Meconium retention occurs in newborn male foals within the first 24 hours of life. Affected foals swish their tails from side to side, strain to defecate, and roll. The diagnosis is made by careful digital examination. Treatment involves gentle administration of a warm, soapy water enema. The prognosis is excellent.
Impaction of the descending colon occurs in ponies, miniature horses, and adult horses with limited access to drinking water or with other causes of intestinal stasis. Most recently, the condition has been associated with salmonellosis, although a cause and effect relationship has not been proved. Pain may be severe if the obstruction is complete. In such cases, tympany of the colon occurs secondarily, and ileus results.
The diagnosis is made in adult horses by palpating the obstructing mass in the ventral portion of the abdomen on rectal examination. Foreign body obstruction of the descending colon must be considered if the horse is < 3 years old; the offending material may be rubber fencing, nylon fibers from halters or lead shanks, hay net, or feed sacks. Horses with impactions may be treated medically with analgesics, intravenous fluids, and gentle enemas. Often, however, surgery is required to evacuate the colon because of severity of pain and gas distention. The prognosis associated with impaction of the descending colon is fair, unless it is complicated by severe colitis after the obstruction has been removed. The prognosis associated with foreign body obstruction is good.
For More Information
Also see pet health content regarding colic in horses.






