

Proper growth and development of the oral cavity depends on a series of events that must occur normally and in the proper sequence. Genetic abnormalities or trauma that affects either the developing tissues or the timing of their development can cause abnormalities.
Defects that decrease comfort, health, or function require treatment; those that result in only an aesthetic problem do not. Common developmental problems include persistent deciduous teeth, unerupted teeth, malformed teeth, skeletal malocclusions, and malformed jaws.
Persistent Deciduous Teeth in Small Animals
Deciduous teeth of kittens and puppies are designed to function in a small mouth (fewer in number and smaller in size) and for a temporary period of time. Dental trauma during this time of energetic oral exploration is often compensated for by the exfoliation of the damaged teeth as the permanent teeth erupt. The permanent teeth are larger and more numerous, erupting as the jaws lengthen to accommodate them (see ).

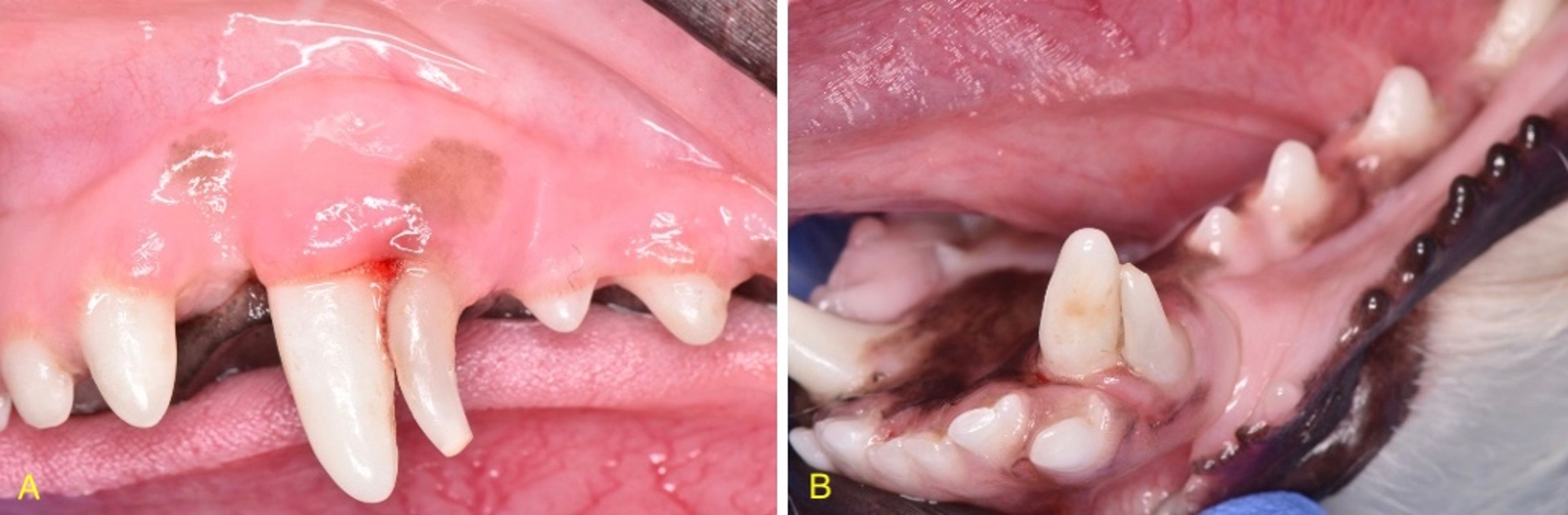
Image A depicts the normal eruption pattern of the left maxillary canine tooth, and image B depicts the eruption of the left mandibular canine tooth. A normal eruption of teeth would include the deciduous tooth exfoliating before the permanent successor begins its eruption. No two teeth trying to occupy the same space should be in the oral cavity at the same time.
Courtesy of Dr. Brenda Mulherin.
Exfoliation of deciduous teeth is a complex process, part of which involves pressure exerted by the crown of the subjacent permanent tooth against the root of the deciduous tooth. If the permanent tooth does not erupt in the correct position, the deciduous tooth may remain firmly in position.
A deciduous tooth may also remain within the oral cavity if there is no succedaneous permanent tooth (hypodontia). In addition, a genetically malpositioned permanent tooth bud or traumatic displacement of the tooth bud may lead to the presence of a persistent deciduous tooth.
Persistence of a deciduous tooth in areas of wide tooth spacing may not cause a problem clinically. However, if the deciduous tooth causes crowding of the permanent tooth (often the case with canine teeth in dogs), the area is predisposed to periodontitis.
In addition, the displaced permanent tooth can result in a traumatic occlusion that requires treatment. Timing of deciduous tooth exfoliation and permanent tooth replacement is genetically determined. In rare cases, trauma during tooth development can cause displacement of a tooth bud that affects exfoliation.
Most commonly, two canine teeth (one deciduous and one permanent) are present at the same time.
The permanent maxillary canine tooth erupts mesial (rostral) to the deciduous one, giving the appearance of a wider and blunter canine tooth rostral to a narrower one with a sharper cusp. The permanent mandibular canine tooth erupts lingual (medial) to the deciduous one, giving the appearance of a wider and blunter canine tooth toward the tongue next to a narrower one with a sharper cusp positioned toward the lip.
In the premolar area, it is common to see a deciduous tooth in an area with no simultaneous permanent tooth. A smaller-than-normal premolar should be radiographed for evaluation of its anatomy and root structure to determine whether it is a deciduous tooth.
A deciduous tooth should be extracted when it remains in the oral cavity once its successor permanent tooth has begun eruption. This is to encourage the permanent tooth to erupt into a more appropriate position.
Persistent deciduous teeth that do not have a permanent tooth replacement may be left within the oral cavity if there is no clinical or radiographic evidence of disease and if they are not causing crowding to the surrounding teeth. However, if there is no evidence of eruption from a permanent tooth, radiographs should be taken to verify that there are no embedded or impacted permanent teeth at the site of the deciduous tooth, the roots are not being resorbed, and no cysts are developing.
Because most persistent deciduous teeth are genetic, pets with this problem should not be bred unless the condition is known to have been caused by trauma.
Unerupted Teeth in Small Animals
Tooth eruption is genetically programmed. Some breeds, particularly small breeds (eg, Maltese), are predisposed to delayed or incomplete eruption. Some brachycephalic breeds are predisposed to malpositioned first premolar teeth that remain unerupted because of their abnormal position.
Trauma can also move a tooth bud into a position in which it is unable to erupt because of impact against another structure.
In some breeds (particularly the terrier breeds), missing premolars are considered a variation of normal. But in all animals, an edentulous area where there should be a tooth is an indication for radiography.
An unerupted (retained) tooth should be easily identified radiographically. Any area in which there should be a tooth present clinically warrants radiographic imaging to verify whether an unerupted tooth is present, which frequently results in the need for intervention and treatment.
Several terms can be associated with a tooth that is not clinically present:
Embedded refers to an unerupted tooth covered in bone. In this case, it is thought the eruption of the tooth was compromised by a lack of eruptive force.
Impacted refers to an unerupted or partially erupted tooth, in which the eruption was prevented by contact with a physical barrier, such as another tooth, bone, or soft tissue.
While it may be difficult to ascertain the true etiology of an unerupted tooth, the most important concept to understand is that edentulous areas need radiographic imaging to identify whether intervention or treatment is needed.
Teeth that are incompletely erupted with a persistent gingival covering can be treated with operculectomy (a form of gingivectomy) to sculpt the tissue to a normal architecture around the crown of the tooth. Individual teeth that are completely unerupted after maturity may remain quiet and require only radiographic monitoring. Alternatively, they can also form dentigerous cysts that can destroy large areas of the jaws (see ).


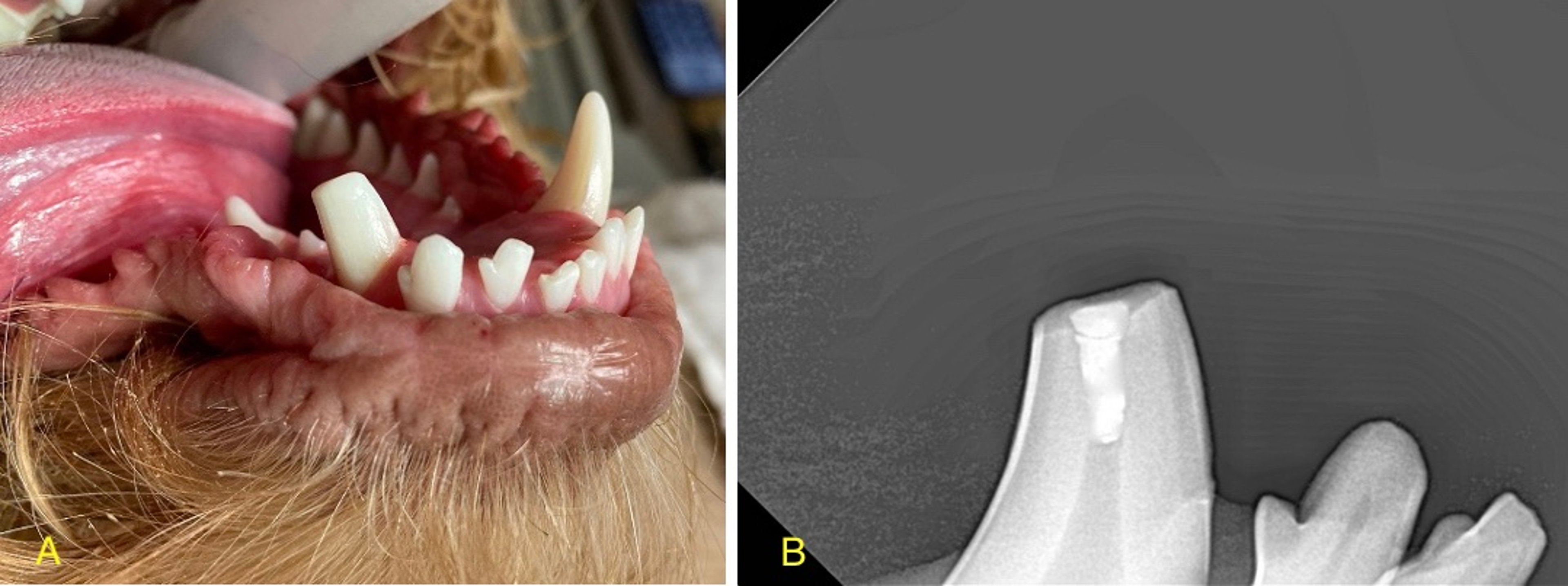
Unerupted (red arrow) left mandibular first premolar tooth of a dog. Note the radiolucent area surrounding the unerupted tooth just distal to the canine tooth. In addition, the cystic area appears to affect the left mandibular second premolar tooth. A cystic lesion that is associated with an unerupted tooth is most consistent with a dentigerous cyst.
Courtesy of Dr. Brenda Mulherin.
Mandibular first premolars are markedly predisposed to cyst formation, particularly in brachycephalic breeds. For that reason, any missing mandibular first premolar teeth should always be radiographed. Should there be any unerupted teeth identified, they should ideally be removed or at a minimum closely monitored with annual intraoral radiographs.
While any tooth within the mouth can be found to be unerupted, the mandibular first premolar teeth and canine teeth are most frequently observed to be clinically absent and radiographically present.
The accepted treatment and best practice is extraction of any teeth that are found to be unerupted. Surgical removal of deeply unerupted mandibular canine teeth can be challenging; therefore, referral to an oral surgeon may be warranted.
Conservative radiographic monitoring should only be considered if the patient is a mature or senior patient without radiographic or clinical evidence of cyst formation, the patient has comorbidities that may compromise anesthetic stability, and the owners are committed to bringing the pet back for annual radiographic monitoring.
Animals with unerupted teeth should not be bred unless it is known the condition was caused by trauma.
Malformed Teeth in Small Animals
Any interruption during tooth formation can result in a malformed tooth. The insult can be traumatic, metabolic, infectious, or rarely genetic.
Insults to epitheliogenesis (eg, parvovirus, distemper virus, high fever) that occur during amelogenesis can cause enamel hypoplasia or hypomineralization. Histological evaluation is usually necessary to distinguish between these two diagnoses.
Enamel abnormalities can be regional, with circumferential lines of missing enamel (rough surface with staining), or generalized with complete loss of enamel. Insults to dentin formation can cause deformed or missing roots.
Enamel hypoplasia or hypomineralization is treated with early dentin sealants to prevent bacterial ingress to the pulp (see ). Composite resin veneers can also protect the softer dentin from abrasion and provide a smooth surface on which plaque is less able to form; however, they will eventually wear or chip.


Evidence of enamel hypoplasia associated with a canine tooth of a dog. The rough surface of the tooth will be more plaque-retentive.
Courtesy of Dr. Brenda Mulherin.
Radicular dysgenesis can present with relatively normal-appearing crowns that are mobile. The lack of roots is readily identified on radiographs.
Root dysgenesis carries a poor longterm prognosis. The teeth can be maintained for years with strict oral care and avoidance of any dental trauma or overuse. Individual anomalous teeth should be evaluated for associated disease; many cause no problem and do not require treatment.
An individual tooth abnormality that appears to be genetic is convergent roots of the mandibular first molar tooth. This anomaly less commonly affects other teeth.
Clinically the crown may appear normal or have a small developmental groove on the buccal surface extending from the gingival margin.
Radiographically, the roots converge apically instead of having their normal divergent position. The crown can appear too large in relation to the size of the roots. The convergence causes the floor of the pulp chamber to arch dorsally into the main pulp chamber, giving it the radiographic appearance of dens in dente, or dens invaginatus.
These teeth frequently have a communication from the periodontal ligament to the pulp chamber in the furcation area, resulting in an extremely high rate of endodontic disease.
Other individual tooth anomalies, such as supernumerary teeth, twinning and fusion of teeth, supernumerary roots, and “peg” teeth (short cylindrical teeth) can be observed.
Supernumerary teeth are an excess number of teeth present in the oral cavity. Treatment may not be necessary if there is enough space within the oral cavity and all teeth are periodontally and endodontically healthy.
Supernumerary roots are excess roots present above the expected number of roots associated with a specific tooth (see ). Again, treatment may not be necessary if the tooth and all associated roots are periodontally and endodontically healthy.


The radiographic image depicts a supernumerary root of the left mandibular second molar tooth of a dog. This dog is also missing the left mandibular third molar tooth. In a normal dentition, there should be no three-rooted teeth observed in the mandible. While a supernumerary root can be present, diagnostic imaging of the tooth is frequently the only way to identify whether additional or fused roots are present. Frequently, supernumerary roots are found associated with the furcation area of a tooth.
Courtesy of Dr. Brenda Mulherin.
It may be difficult to identify whether a tooth has additional roots by clinical observation. Diagnostic imaging is frequently necessary to confirm. Occasionally, there will be an additional cusp associated with the crown of a tooth to indicate that there may be additional roots associated with a specific tooth.
Malocclusion and Malformed Jaws in Small Animals
Malocclusions are nearly always genetic; however, trauma during development can interfere with normal growth.
Maxillary length is easier to manipulate through selective breeding than mandibular length. As a result, a preference for longer faces and noses inadvertently selects for mandibular distoclusion or class 2 malocclusion (ie, overbite, or lower jaw appears shorter than upper jaw). By contrast, selecting for a “blockier” head or shorter nose results in mandibular mesioclusion or class 3 malocclusion (ie, underbite, or lower jaw appears longer than upper jaw).
The upper and lower jaws develop at different rates, making the timing of tooth eruption critical. If the jaws have an abnormal relationship to each other at the time the permanent teeth gain enough height to create an occlusion, the dentition is locked into the abnormal position. If this occurs unilaterally, it can allow continued jaw lengthening on one side while arresting the growth of the other side, resulting in a mismatch of the central incisor midlines (ie, asymmetric skeletal malocclusion, such as wry bite or class 4 malocclusion).
The most common maxillary-mandibular discrepancy is a horizontal symmetric skeletal malocclusion, resulting in mandibular mesioclusion (class 3 malocclusion) or mandibular distoclusion (class 2 malocclusion). The latter problem often causes traumatic occlusion when the mandibular canine teeth impact against the most rostral hard palate. Linguoversion of the mandibular canines often accompanies this problem because the mandibular canine teeth are directed palatally as they erupt along the palatal surface of the maxillary canine teeth.
Individual tooth malposition (dental malocclusion or class 1 malocclusion) can also be genetic, such as mesioversion of the canine teeth (ie, “lance projection”) in Dachshunds and Shetland Sheepdogs.
When deciduous dentition is present, interceptive orthodontics can be performed by selectively extracting deciduous teeth that are malpositioned. If there is a dental interlock in which the maxillary and mandibular teeth have difficulty separating from each other, extracting the locked teeth can allow the jaws to grow to their genetic potential independent of each other.
A class 2 malocclusion or mandibular distoclusion of the deciduous teeth can be treated by extraction of the deciduous mandibular canine and potentially incisor teeth. This not only relieves the dental interlock but also encourages the permanent mandibular canine teeth to erupt in a more labial angle (they normally erupt on the lingual aspect of the deciduous canine teeth) to help correct the malocclusion.
Likewise, a class 3 malocclusion or rostral crossbite of the deciduous teeth can be treated by extraction of the deciduous maxillary incisors. This both relieves the interlock and also encourages the permanent incisors to erupt in a more labial angle (they normally erupt on the palatal side of the deciduous incisors) to help correct the malocclusion.
Whenever deciduous teeth are extracted, contact with or trauma to the developing tooth bud of the permanent successive teeth must be avoided so as not to damage the enamel organs or developing enamel. Damage to the developing, unerupted tooth can result in brown spots on the crowns of permanent teeth due to focal areas of enamel loss or enamel defects.
To help avoid trauma to the developing teeth, surgical instruments used for elevating the tooth from the socket should not be inserted on the lingual aspects of deciduous incisor or canine teeth. Even with proper technique, enamel damage can occur because the enamel epithelium can be disrupted as the deciduous tooth is extracted from the alveolus.
A class 3 malocclusion or mandibular mesioclusion in the permanent dentition is considered normal for many brachycephalic breeds and does not require treatment unless it results in a traumatic occlusion. If the mandibular canine teeth contact the palatal aspect of the maxillary incisors, extraction of the maxillary incisors associated with the malocclusion may create a wider diastema for the canine teeth to occlude atraumatically, thus resolving the problem.
The rostral crossbite (ie, maxillary incisors positioned lingual to the mandibular incisors) rarely causes discomfort or a traumatic occlusion. In contrast, mandibular distoclusion or a class 2 malocclusion often requires orthodontic or surgical intervention.
Affected canine teeth causing a traumatic occlusion can be orthodontically moved by a veterinary dentist into a nontraumatic (not always normal) position that is a more comfortable and functional occlusion for the patient.
Multiple anesthetic events may be necessary to move the tooth into an atraumatic position. At minimum, two anesthetic events are necessary: one to place the orthodontic appliance or device and one to remove the appliance.
Alternatively, the malpositioned tooth can be shortened with a crown reduction procedure and the pulp treated with endodontic therapy (vital pulp therapy). The goal of this technique is to allow the patient to maintain the tooth at a much shorter height but still maintain some of its form and function. In addition, this technique is much less invasive than extraction of the affected tooth (see ).

Crown reduction and vital pulp therapy are frequently performed on malpositioned mandibular canine teeth. (A) The malpositioned tooth’s height is decreased to at or just above or below the height of the associated incisor teeth. (B) A medicament is placed to protect the pulp of the tooth to keep the tooth vital.
Courtesy of Dr. Brenda Mulherin.
This technique is also performed by a veterinary dentist. The procedure requires a sterile technique to avoid introducing infection into the pulp and placement of a medicament to stimulate dentin deposition to keep the tooth alive. Continued follow-up radiographs throughout the patient's life are required to monitor the need for definitive endodontic treatment.
Extraction of a tooth that is causing a traumatic occlusion is also a viable treatment option. Extraction of a malpositioned tooth is the most invasive of the procedures; however, it is frequently the least expensive treatment and requires the least amount of follow-up.
Examination of the patient 10–14 days postoperatively to evaluate the healing of the soft tissues is frequently all that is required to assess the success of treatment. Depending on skill level and comfort, this procedure can be performed by general practitioners.
Because of the suspicion that most malocclusions have a genetic component, only animals with a normal, atraumatic occlusion should be used for breeding. Unless the patient has a history of a traumatic event that may have caused the abnormal eruption of a tooth or malformation of the jaw, genetic counseling should be considered and breeding of the patient should be discouraged.
For More Information
Also see pet health content regarding dental disorders of dogs and dental disorders of cats.





