



Bacterial Diseases of Amphibians


Courtesy of Research Animal Diagnostic Laboratory, University of Missouri.
Brucella inopinata-like
An emerging gram-negative coccobacilli bacteria in the family Brucellaceae (originally identified at Ochrobactrum anthropic) causes multifocal subcutaneous abscesses primarily affecting the amphibian's spine and limbs. Lesions have been reported in visceral organs and invading bony tissues. These lesions typically respond well to antimicrobials; however, occasionally surgical debridement is needed. Culture and histologic assessment can be used to differentiate this organism from other granulomatous lesions (eg, mycobacteriosis, chlamydiosis).
Chlamydiosis
Chlamydiosis, often caused by Chlamydia pneumoniae, C psittaci, C abortus, or C suis, is a serious infection of amphibians. Chlamydia spp have also been found in apparently healthy frogs, which raises the question of whether these animals are reservoirs or vectors. Clinical signs are nonspecific and, if present, include neurologic signs, hyperemia, sloughing skin, cutaneous depigmentation, petechiae, coelomic distension, and edema. Infected frogs may die peracutely or exhibit lethargy and disequilibrium. Histologically, intracytoplasmic basophilic inclusion bodies can be identified in sinusoidal lining cells of the liver and spleen. Secondary bacterial infections frequently occur in affected amphibians and must be treated appropriately. Diagnosis is usually confirmed with PCR assay. Antimicrobial treatment, including doxycycline (5–10 mg/kg, PO, every 24 hours for 10–14 days) or oxytetracycline (50 mg/kg, PO, every 24 hours for 10–14 days), may be effective against chlamydial infection.
Mycobacteriosis
Mycobacteriosis, are caused by non-tuberculous acid-fast bacilli, including Mycobacterium fortuitum, M marinum, M chelonea, M abscessus, M avium, M szulgai, M xenopi, and M liflandii. Captive amphibians that are debilitated or kept in crowded or unsanitary conditions are most susceptible. Anurans appear to be more frequently affected than caudatans, and captive species appear to be more affected than free-ranging amphibians. Although often an infection of the integument, ingestion of infectious organisms may also lead to gastrointestinal disease and systemic infection. Infections appear to be opportunistic because these bacteria are often isolated in aquatic environments and substrates. Individual animals can be affected as well as population outbreaks. Affected amphibians may have gray nodules or ulcerations in the skin, liver, kidneys, spleen, lungs, and other coelomic organs. Infected amphibians may eat well but still lose weight. Acid-fast bacilli may be detected in feces and oropharyngeal mucus. A presumptive diagnosis can be made by finding acid-fast bacilli in animals with external lesions with impression smears. Confirmation requires bacterial culture isolation from fresh tissue or the use of molecular methods (ie, PCR assay). Treatment is typically unrewarding for this potentially zoonotic disease, and euthanasia should be considered.
Red-leg syndrome (bacterial dermatosepticemia)
Red-leg syndrome, also known as bacterial dermatosepticemia, refers to hyperemia of the ventral skin that accompanies systemic infection in amphibians. Saprophytic, gram-negative bacteria such as Aeromonas spp, Pseudomonas spp,Proteus spp, Elizabethkingia meningoseptica, Klebsiella spp, and Citrobacter spp typically cause red-leg syndrome. However, gram-positive organisms such as Streptococcus spp have been isolated from patients. Cultures should be considered for directing antimicrobial treatment. Ventral hyperemia is a nonspecific sign and may also occur with toxicosis, viral (ie, ranavirus), and fungal (ie, chytridiomycosis) infection. Malnourished, newly acquired amphibians that are maintained in poor-quality water or other inappropriate environmental conditions are particularly susceptible.
Clinical signs include lethargy, emaciation, ulcerations of the skin, and characteristic cutaneous pinpoint hemorrhages of the legs and abdomen. Hemorrhages may occur in the skeletal muscles, tongue, and nictitating membrane. In acute cases, these clinical signs may be absent. Histologic evidence of systemic infection can include inflammatory or necrotic foci in the liver, spleen, and other coelomic organs. Blood or, if present, coelomic fluid should be taken for culture and cytologic evaluation to direct treatment. A thorough review of husbandry practices, including water testing, environment temperature testing, and assessment for overcrowding, must be completed.
Fungal Diseases of Amphibians
Many of the fungi that infect amphibians are difficult to distinguish grossly because they produce similar clinical effects, including lethargy and skin ulcerations. Some fungi can be identified via the examination of a wet mount prepared from a skin scraping, whereas others require culture, histologic evaluation, and special stains. Treatment includes proper hygiene and the use of topical or systemic antifungal agents.

Courtesy of Alison Burke, Johns Hopkins School of Medical Illustration and the National Aquarium.

Courtesy of Courtney McKena, Johns Hopkins School of Medical Illustration and the National Aquarium.
Chromoblastomycosis
Chromoblastomycosis is a chronic fungal infection involving the dermal and subcutaneous tissue layers. Chromoblastomycosis is caused by pigmented or black fungi from several genera (eg, Cladosporium spp, Fonsecaea spp, Phialophora spp, Ochroconis spp, Rhinocladosporium spp, and Wangiella spp). These fungi may be found in organic substrates such as topsoil and decaying plant matter and seem to cause sporadic and opportunistic infections. Disease is either cutaneous or disseminated; both have been reported in captive and wild populations of amphibians. Clinical signs include anorexia, weight loss, granulomatous skin lesions or ulcers, coelomic distention, and neurologic disease. Diagnosis is usually made postmortem by finding disseminated granulomas with pigmented fungal cells and hyphae. Culture is frequently unsuccessful.
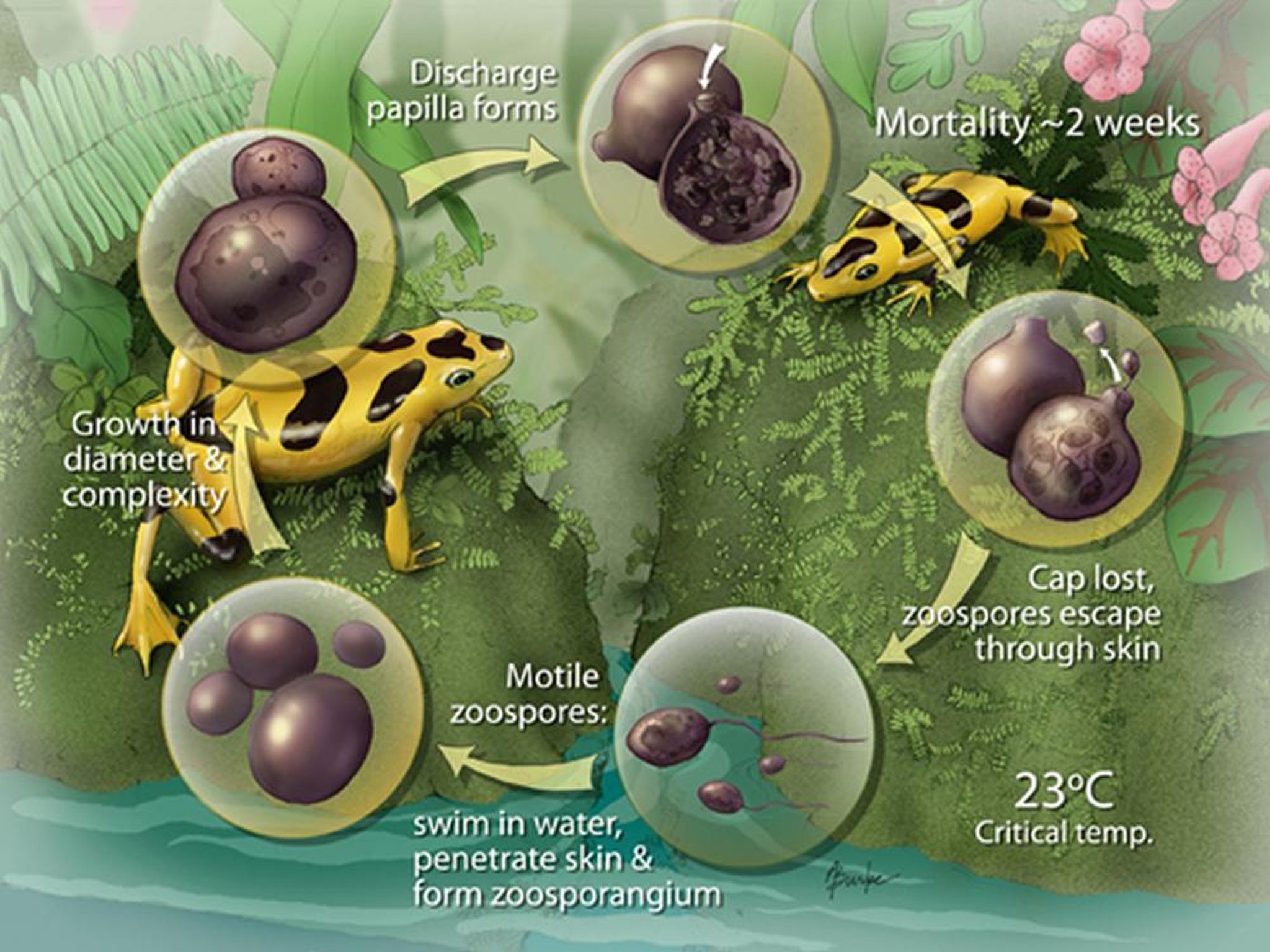
Chytridiomycosis
Chytridiomycosis is caused by the fungal organisms Batrachochytrium dendrobatidis (Bd) and Batrachochytrium salamandrivorans (Bsal). This group of fungi are reportable to the World Organisation for Animal Health (OIE) because of concerns of dissemination. This group of fungi have emerged as important causes of morbidity and mortality, causing major population declines in free-ranging and captive amphibian populations.
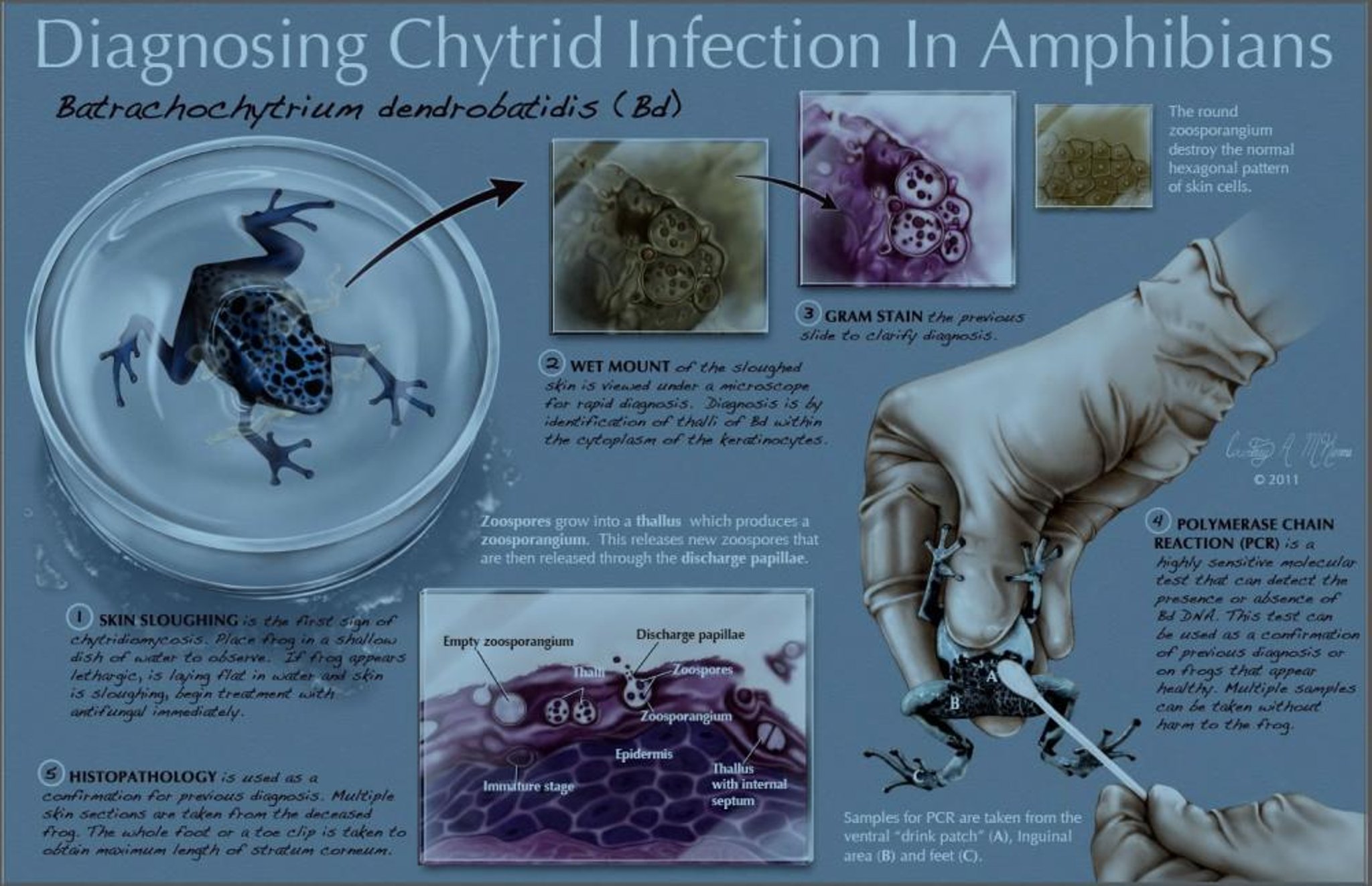
Chytrid fungi have been isolated from active disease process in anurans, caudates, and caecilians. Both Bd and Bsal infect keratinocytes in the skin of adult animals and mouth parts of tadpoles (tadpole skin is lacking in keratinocytes). The intracellular fungal bodies mature to form zoosporangia which contain numerous infective flagellated zoospores. These zoospores are free swimming and are capable of infecting cohorts. Death and clinical signs seem to be caused by damage to the epidermis, resulting in fluid and electrolyte losses leading to cardiac failure. Clinical signs include brown to red discoloration of the skin, excessive shedding and mucus production, muscle incoordination, and acute death. In tadpoles, depigmentation of toothrows or acute death may occur. Clinical signs in caudates are typically mild and may be limited to discolored cutaneous lesions. Pathogenicity of the fungi seem to be genotype specific, and infection intensity (>10,000 zoospores) seems to be associated with increased mortality.
Environmental and social factors also influence the disease process, with cooler temperatures and increased stress levels contributing to increased pathogenicity. Although the role of the adaptive immune system is unknown with this disease process, cutaneous bacteria (eg, Janthinobacterium lividum) flora metabolites have showed to confer protection. Because pathogenicity of Bd seems to decline above 25°–27°C, it is speculated that some amphibian populations living at higher elevations have disappeared because of the cooler temperatures associated with the winter months and possibly climate change. Some amphibians, including the bullfrog (Rana catesbeiana) and the African clawed frog (Xenopus laevis), are less susceptible to Bd and may serve as reservoirs for the disease.
The digits and the drink patch (specialized skin located in the ventral pelvic region that absorbs water) are good places to obtain samples for assessment. Visualizing the spherical, single-celled organisms in skin scrapings stained with Wright-Giemsa or Gram stains using a light microscope is diagnostic; however, the organisms are not always readily seen. Real-time PCR assay performed on swabs of the integument or pieces of skin is diagnostic and provides rapid assessment of presence and quantity of zoospores. This is useful in screening and management of amphibian populations at risk, such as those undergoing transport or quarantine. On histologic evaluation, zoosporangia containing zoospores are associated with hyperkeratosis and underlying dermal infection. Fungal cultures are not routinely performed because they are not useful for diagnosis.
Treatment includes the topical administration of itraconazole (a 0.01% bath for 5 min/day for 10–11 days). Maintaining animals well within their normal thermal range may be effective. The use of terbinafine (0.01% bath, buffered using bicarbonate to a pH of 7.2–7.4, for 5 min/day for 5 days) can also be considered. Spraying animals daily with voriconazole at 125 mg/L for 7 days may be effective and less time intensive. If appropriate for the species, raising environmental temperatures for captive populations to >23°C may help halt the infection, and medicated baths are used to eliminate Bd. Systemic antifungal drugs seem to be ineffective in treating this infection of the epidermis.
Saprolegniasis
Saprolegniasis refers to disease caused by several genera of opportunistic fungi or water molds that infect the gills and skin of aquatic and larval amphibians. These water molds come from the genera Saprolegnia, Aphanomyces, and Achyla. Affected animals have a whitish, cotton-like growth on their skin, typically at the site of previous trauma such as abarasions. Removal of the slime layer due to chemical irritants such as disinfectants, soaps, detergents, or ammonia spikes and malnutrition, especially hypovitaminosis A, may also contribute to formation.
As the fungal mat ages, it may become greenish due to the presence of algae. Once removed from water, the fungal mat collapses and is difficult to see. Other clinical signs include lethargy, respiratory distress, anorexia, and weight loss, depending on the extent of the lesions.
A presumptive diagnosis of saprolegniasis is made by finding hyphae and the thin-walled zoospores in skin scrapes. When practical, raising water temperature above 20°C can aid removal of the lesions. Poor water quality conditions should be corrected. Localized, smaller infections can be surgically debrided, and salt water (>30 ppt salinity) can be applied daily until the lesions resolves. Treatment with antifungals as described for chytridiomycosis can also be effective. Eggs can be treated with methylene blue.
Zygomycosis
Fungal dermatitis caused by true fungi of the class Zygomycetes (Mucor spp, Basidiobolus spp, and Rhizopus spp) and Fusarium spp, affects both wild and captive populations of anurans. Infections seem to be opportunistic after traumatic skin lesions, water quality issues, or hypovitaminosis A. Clinical signs include lethargy and multifocal hyperemic nodules with fungal growth on the ventrum. Disease progresses rapidly and results in mortality within 2 weeks. Zygomycetes are found in the environment, especially soils and decaying matter, and are a normal component of the amphibian's gastrointestinal tract. Successful treatment has not been reported, but advanced antifungal agents may be tried.
Parasitic Diseases of Amphibians

Courtesy of the National Aquarium.


Courtesy of Dr. Taylor Yaw.
Many of the protozoa and metazoa found in and on amphibians are not associated with disease unless the host amphibian is stressed or immunocompromised. Recently caught or transported amphibians are particularly susceptible to parasitism, as are those kept in poor hygienic conditions and outside their preferred optimal temperature zone (POTZ). Parasites with indirect life cycles tend to die out when wild-caught amphibians are brought into captivity if the intermediate or final host is not present. Conversely, infections by parasites with a direct life cycle may be magnified in a closed environment. Excellent hygiene is essential for parasite control and includes the routine removal of sloughed skin, fecal material, uneaten food, and carcasses from animal enclosures.
Metazoa parasites include nematodes, trematodes, acanthocephalans, and pentastomes. These infect both captive and wild animals. Amphibians may act as final or as intermediate host for the various life cycles of these metazoan parasites. Intermediate stages of many metazoan parasites can be found encysted within amphibian soft tissues, causing no clinical disease (eg, Eustrongylides spp, Angiostrongylus cantonensis).
Nematodes
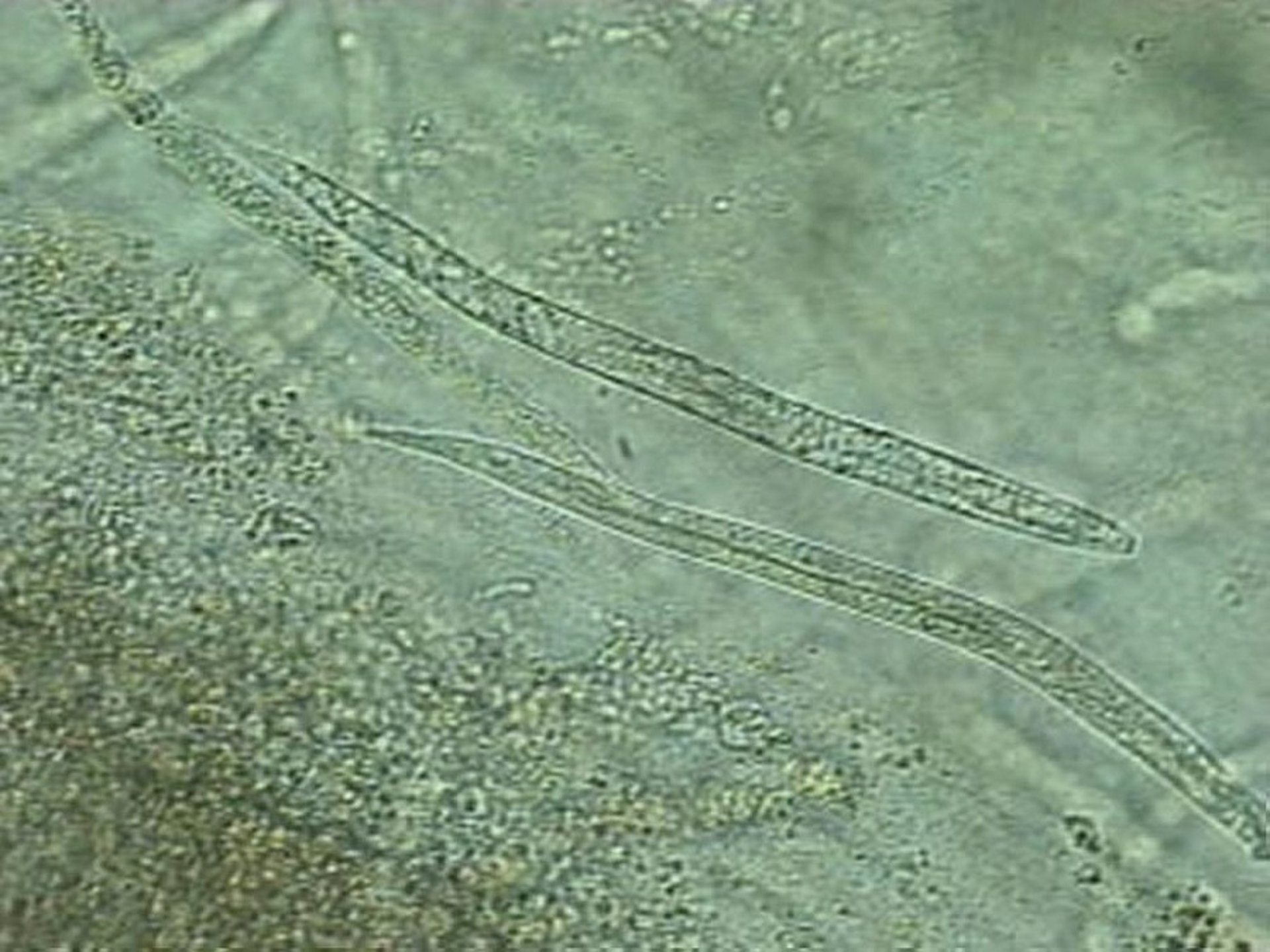
Rhabdiasis, caused by the lungworm Rhabdias spp, is a common cause of pulmonary damage and secondary infections in captive amphibians. This nematode has a direct life cycle with free-living phases that can occur in enclosure substrate. Adult worms live in the lungs, where they deposit larvated eggs that are coughed up, swallowed, and then excreted into the environment. Infective L3 larvae then burrow through the skin of a new host, where they mature and migrate to the lungs. Affected animals may appear anorectic, thin, and generally debilitated. Acute death is not uncommon.

Courtesy of the National Aquarium.
A premortem diagnosis may be made by finding ova or worms in oral and nasal secretions. Infection should be suspected when nematode larva and larvated eggs are found in fresh feces from an animal with clinical signs. When rhabdiasis is suspected, treatment using fenbendazole (100 mg/kg, PO, every 24 hours for 2 days, repeated 12–14 days later) or ivermectin (200–400 mcg/kg, PO, once, repeated 12–14 days later) is recommended. After each treatment, the animals should be moved into a newly established environment to prevent reinfection from free-living life stages. Some reactions to fenbendazole have been reported, so animals should be monitored closely and treatment discontinued if necessary.
Strongyloidiasis, caused by Strongyloides spp, results in proliferative enteritis. It has a similar life cycle to the lungworm Rhabdias spp. Due to their direct life cycle, these nematodes can increase in number rapidly, especially when a host is living in a suboptimal environment. Severe strongyloidiasis may cause debilitation and cause weight loss via protein-losing enteropathy and generalized malnutrition. Eggs or adult worms can found on fecal examination, but differentiation from other intestinal nematodes can be difficult. Treatment with anthelmintics, as with rhabdiasis, may need to be prolonged, and special attention needs to be paid to cage sanitation.
Filariasis is occasionally observed free within the coelomic cavity or encysted within coelomic organs. These are typically seen during coelomic surgery or endoscopy or can occasionally be visualized with transillumination of the coelomic cavity. Microfilaria may be observed in the blood, and, in debilitated animals, treatment may be indicated.
Pseudocapillaroides is caused by the capillarid nematode Pseudocapillaroides xenopi and is the agent of infection in the epidermis of free-ranging and captive African clawed frogs (Xenopus laevis). Lesions have excessive skin shedding with discoloration of the skin surface. Heavy infections can result in skin ulcerations and loss of body condition. Diagnosis is made by demonstrating bioperculate eggs or adults from skin scraps or biopsy and histologic evaluation. A PCR assay is available for detection of P xenopi in enclosure substrate. Treatment with administration of thiabendazole (50–100 mg/kg, PO) and levamisole (5 mg/kg, SC) followed with levamisole (10 mg/kg, SC) at 10 and 20 days was reported to be efficacious. Ivermectin baths (10 mg/L) or levamisole baths (100–300 mg/L) for 1 hour weekly also seem to be efficacious for parasitic removal.
Trematodes and Cestodes
Amphibians are host to a variety of trematodes and cestodes as the primary, secondary, tertiary, or even paratenic host. Larval forms are often found within the amphibian’s body without clinical signs. However, occasionally notable pathological changes are observed with migrating larvae. Adult trematodes can commonly live in a variety of organ systems and occasionally reach high enough numbers to cause wasting or anorexia if present in the gastrointestinal system. Ribeiroia ondatrae, a trematode, has been linked with the development of supernumerary limbs and other developmental abnormalities. Amphibians serve as a secondary host for Spirometra sp, a cestode responsible for sparganosis in mammals. The spargana encyst in subcutaneous tissue, muscle, and organs within the coelomic cavity. Some affected animals have cutaneous nodules present on the coelomic wall and legs that contain encysted worms.
Arthropods and Crustaceans
Arthropods, such as the common fish parasites Argulus sp, and Lernaea sp, may infect amphibian aquatic life cycle stages, whereas ticks and mites affect postmetamorphic terrestrial animals. Larval dipterid flies may consume amphibian eggs and embryos and feed on the tissues of adults.
Protozoa
Most protozoans found in the gastrointestinal tract, including ciliates, opalinids, and flagellates, are commensals and do not need treatment. However, there are a few protozoans that warrant further discussion.
Entamoeba ranarum has been implicated in causing amoebiasis in amphibians. Transmission is caused by ingestion of cysts. This organism has a direct life cycle that can lead to rapid accumulation and spread within a collection. Trophozoites are found in the large colon, where they can damage the mucosa. However, the organism can also be found in the liver and kidneys. Poor husbandry, inappropriate food items, or concomitant infections may predispose amphibians to amoebiasis. Clinical signs are limited and consist of anorexia, wasting, and, in later stages, blood-tinged stool. With renal or hepatic involvement, hydrocoelom and edema may be present. Diagnosis is reliant on visualizing trophozoites on wet mounts from fecal samples or colon washes. Lugol’s iodine may aid with detection of the cyst life-cycle stage. It is difficult to differentiate pathogenic amoebae from commensal amoebae, but in the presence of clinical signs, treatment is warranted. Metronidazole (50 mg/kg, PO, every 24 hours for 3–5 days) can be administered for treatment. Supportive treatment with fluids and nutritional supplementation may be necessary.
Cryptosporidiosis is occasionally seen in amphibian species and is typically caused by Cryptosporidium fragile, an apicomplexan protozoa. Oocysts are common and widespread in water sources and can persist for months within the environment. Sporozoites are typically found in the superficial gastric epithelium. Infections can be subclinical or with the clinical sign of mild weight loss. A presumptive diagnosis can be made with acid-fast stains on fresh feces, regurgitated items, or via endoscopic sampling of the gastric mucosa. Treatment options have not been reported in amphibians, and euthanasia may be warranted for clinically affected animals.
Ciliated protozoa are commonly observed in amphibians. These are routinely observed on fecal examinations and rarely cause gastrointestinal disease. If clinical disease is present, treatment with metronidazole or a tetracycline is warranted. Occasionally, ciliated protozoans can be involved with cloudy patches of skin and gill pathology in aquatic amphibians. Higher loads are often seen in relation to poor water quality and filtration issues. Skin scrapings and gill clips can be used for diagnosis.
Pathogenic lineage of alveolate protozoa from the phylum Perkinsea have recently been linked to large-scale mortality events in free-ranging ranid tadpoles. Severe Perkinsea infections are the third most common infectious disease of anurans after chytridiomycosis and ranavirus infections. Mortality rates as high as 95% have been reported during outbreaks. Affected tadpoles display coelomic distension, cutaneous erythema, edema, and white discoloration of the skin. Histologic examination reveals tissue invasion by myriad of intracellular and extracellular Perkinsea organisms. There is no treatment because this organism causes mass mortality events.
Mesomycetozoans
Mesomycetozoans are fungus-like microorganisms at the animal-fungal boundary that are currently in the protistan class. These organisms also infect fish, birds, and mammals. Although they are known to cause significant mortality events in fish, they are incidental findings in amphibians. Clinical signs in amphibians include muscle swelling in the thigh, rump, and tail and may appear nodular, especially in tadpoles. Debilitation may lead to death, especially in adults. Diagnosis is based on histologic evaluation or finding characteristic spores via microscopic examination of material from the lesions. There is no treatment other than supportive care.
Viral Diseases of Amphibians
Ranavirus
Iridoviruses, which are DNA-based viruses in the genus Ranavirus, family Iridoviridae, have been identified as the cause of mass mortality in wild populations of anurans and caudates across the world. These viruses are reportable to the World Organisation for Animal Health (OIE). Environmental conditions, reservoir species, persistence in the environment, direct and indirect transmission, stress, and host immunity contribute to the impact of ranaviruses on amphibian populations.
Species of ranavirus that infect amphibians include: frog virus 3 (FV3), Bohle iridovirus, midwife toad virus, and Ambystoma tigrinum virus. These viruses are highly virulent and may cause 90%–100% mortality in tadpoles and adults. Transmission occurs via exposure to contaminated water or soil, contact with infected individuals, and consumption of infected tissues. Fish and reptiles (especially turtles) are reservoirs for ranaviruses.
Clinical signs of ranavirus are nonspecific, develop rapidly in a large number of cohorts, and include abnormal swimming behavior, swelling of the limbs or body, edema, hydrocoelom, erythema, ventral skin hemorrhage (especially in the hind region), and occasionally skin ulcerations. Lesions may appear very similar to those of bacterial dermatosepticemias. The original viral lesions may be overwhelmed by secondary invaders, and many outbreaks of red-leg syndrome may have had underlying and undiagnosed viral infection. Death typically results from multiple organ failure. Amphibian larvae undergoing metamorphosis or recently metamorphosed juveniles seem to be most susceptible to infection. For this reason, mortality events often occur in the spring or summer. Survivors seem to acquire some immunity to future infections. Diagnosis is made using PCR assay, primary cell culture, or microscopy.
Ranaviruses can persist in the aquatic environment without a host for weeks, which contributes to their ability to infect naive amphibian populations and emphasizes the need for biosecurity measures when transporting amphibians or working in environments where the virus exists.
Ranid herpesvirus-1
Renal adenocarcinomas (Lucké tumors), caused by ranid herpesvirus-1, are relatively common in leopard frogs (Rana pipiens) wild-caught in the northeastern and north central US. Few frogs with tumors are evident in the summer, because viral replication is temperature dependent. Virus particles and intranuclear inclusion bodies are evident when frogs are in hibernation, at 5°–10°C. Metastasis of the tumor to liver, lungs, and other organs is common; both the primary and metastatic tumors can become very large. There is no treatment. The neoplasm is a model of herpesvirus-induced cancer.
For More Information
Divers S, Stahl S, eds. Mader's Reptile and Amphibian Medicine and Surgery. 3rd ed. Elsevier, 2017.
Also see pet health content regarding diseases and disorders of amphibians.






