



Marine mammals are susceptible to all of the major groups of parasites, including various nematodes, trematodes, cestodes, mites, lice, and acanthocephalans. Clinical experience with many of these is limited, whereas others are commonly seen in recently captured specimens.
Acanthocephalans of Marine Mammals
Cetaceans are the primary host of Bolbosoma spp but can be infested with parasites of the genus Corynosoma, which have pinnipeds and sea otters as primary hosts. Bolbosoma spp have been reported in pinnipeds. Corynosoma enhydra has only been reported from sea otters.
Diagnosis is by detection of eggs in feces, but clinical disease and treatment are not well documented. Three species of Profilicollis (also found in birds) are reported to cause peritonitis associated with intestinal perforation in sea otters. Death usually occurs before the parasite produces ova. Premortem diagnosis is problematic; peritoneal fluid may show evidence of inflammation.
Successful treatment is very rare and highly intensive, involving very slow rehydration and refeeding of affected otters in addition to antimicrobial and gastroprotectant medications.
Acariasis of Marine Mammals
Nasal and lung mites: Nasal and lung mites are found in phocid and otariid seals. The life cycles of these mites are not completely known.
Lung mites cause rattling coughs. Nasal mites may cause nasal discharge but apparently little discomfort. Mite infestations have been associated with large, roughened lesions of the laryngeal area of cetaceans, but their overall importance or treatment is unknown.
Diagnosis is made by identifying the mite in nasal secretions or sputum.
Infections have been cleared rapidly with ivermectin (200 mcg/kg, SC, repeated after 2 weeks). Treatment of infected animals eliminates the problem in captive enclosures without environmental treatment.
Demodectic mange: Demodectic mange has been diagnosed in California sea lions and polar bears. Predisposing factors in pinnipeds are unknown. The mites are not readily transmitted among contact animals.
Nonpruritic, alopecic lesions with hyperkeratosis, scaling, and excoriation develop on the flippers and other body surfaces that contact the substrate. Secondary bacterial infection that results in pyoderma is seen in chronic cases.
Diagnosis is made by deep skin scrapings and identification of the mite.
Treatment is the same as in dogs.
They are highly sensitive to ivermectin as well as to chlorinated hydrocarbon insecticides. Rotenone powder is also effective. The affected animal must be removed from the water, allowed to dry before being dusted, and kept out of the water for ≥12 hours. Treatments must be repeated in 10–12 days. Animals in captivity can be freed of parasites if no new sources of infestation are introduced.
Pediculosis of Marine Mammals
Sucking lice are common in wild pinnipeds. The lice can be seen grossly and are readily transmitted.
Heavy infestations can cause severe anemia.
They are highly sensitive to ivermectin as well as to chlorinated hydrocarbon insecticides. Rotenone powder is also effective. The affected animal must be removed from the water, allowed to dry before being dusted, and kept out of the water for ≥12 hours. Treatments must be repeated in 10–12 days. Animals in captivity can be freed of parasites if no new sources of infestation are introduced.
Lungworms of Marine Mammals
Lungworms are common in pinnipeds and cetaceans. Sea lions have Parafilaroides decorus, whereas true seals are usually parasitized by Otostrongylus circumlitus. The latter parasite is also found in the hearts of some phocids; however, it does not produce a microfilaremia. Both of these parasites use fish as intermediate hosts. There are at least four species of lungworms in various cetacean hosts, including Halocercus lagenorhynchi, which has caused prenatal infections in Atlantic bottlenose dolphins.


Courtesy of Dr. James McBain.
Lungworm infection can be diagnosed by examination of feces or bronchial mucus. Diagnosis of O circumlitus in elephant seals is complicated by death occurring after generalized clinical signs of lethargy, dehydration, and neutrophilia before the parasites become patent and first-stage larvae can be detected in sputum or feces.
Anorexia, coughing, and sometimes blood-flecked mucus are the first signs of pulmonary parasitism. Lungworm infections often remain subclinical for long periods, with clinical signs appearing only when an animal becomes debilitated for other reasons.
Treatment of P decorus infection consists of mucolytic agents administered intratracheally, antimicrobials to treat any concomitant bacterial pneumonia, ivermectin or moxidectin (either at 0.2 mg/kg), and concurrent prednisone or dexamethasone as parasite die-off can cause severe inflammation.
Some treatment success has been reported using intratracheal administration of levamisole phosphate (5 mg/kg, intratracheally, every 24 hours for 5 days); however, combined therapy with ivermectin and fenbendazole given 3 days after initiation of therapy with dexamethasone, antimicrobials, and mucolytic agents may be more effective. Cetacean lungworms probably are also susceptible to levamisole and ivermectin; however, the sudden deaths of two beluga whales injected IM with levamisole phosphate suggest this drug administered by that route may be contraindicated. A percentage of pinnipeds also show neurologic reactions to IM injection of levamisole; PO or SC administration has been recommended.
In captivity, lungworm infections are usually self-limiting if larvae are not introduced in fresh fish intermediate hosts. Feeding frozen fish prevents reinfection.
Heartworm of Marine Mammals
Courtesy of Dr. James McBain.
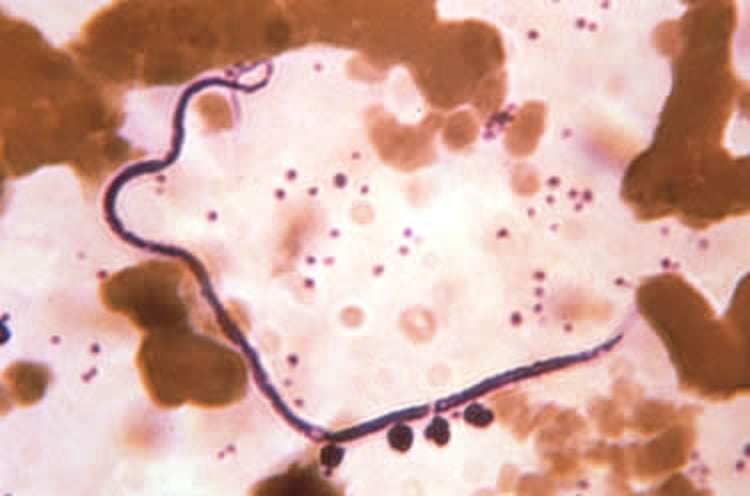
Heartworms of the genus Acanthocheilonema are a common necropsy finding in pinnipeds. Phocid seals are affected by A spirocauda, and otarids are infected subcutaneously by A odenhali. Transmission of A spirocauda is thought to be by the seal louse (Echinophthirius horridus). Both groups of pinnipeds can be infected with the canine heartworm, Dirofilaria immitis, in endemic areas; however, phocid seals are abnormal hosts.
Dirofilariasis is diagnosed by identifying microfilariae in the blood, although careful evaluation is needed as benign A odenhali microfilariae are common in otariids and can be mistaken for Dirofilaria. Transmission is thought to be by the same mosquitoes that bite dogs.
A graded regimen of levamisole phosphate progressing to a high dosage (40 mg/kg, PO, every 24 hours for 1 week) has successfully cleared infection in captive pinnipeds, with the advantage of oral administration. Prevention in endemic areas has been successful with oral administration of ivermectin (canine dosages) monthly or diethylcarbamazine (3.3 mg/kg) weekly in food during the mosquito season.
Other Nematodes of Marine Mammals
Courtesy of Dr. James McBain.
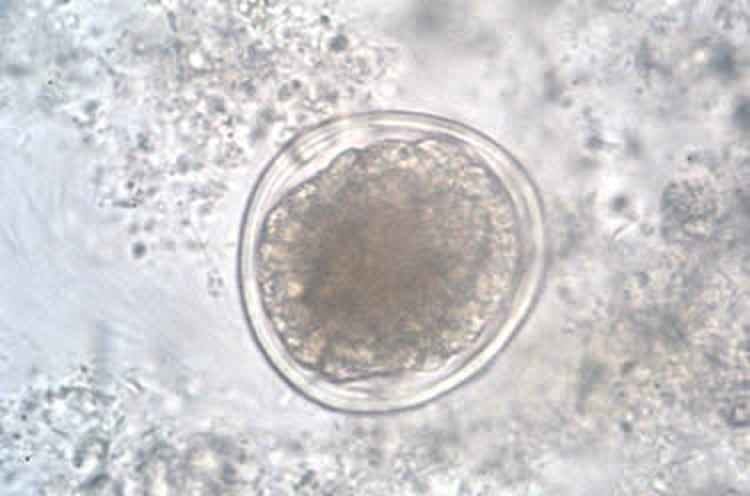
Anasakidae: The Anasakidae are pathogenic nematodes found in the stomach of marine mammals. Granulomas form at their attachment sites and can lead to blood loss, ulceration, and ultimately perforation and peritonitis. Raw fish is most often incriminated as the source of infection. Infections with Contracaecum spp are common in wild cetaceans and pinnipeds. Polar bears in captivity are prone to heavy ascarid infection.
Diagnosis is usually with fecal evaluation.
Gastric nematodes can be successfully treated with dichlorvos (30 mg/kg, PO, given twice, 10 days apart), fenbendazole (11 mg/kg, PO, given twice, 10 days apart), or mebendazole (9 mg/kg, PO, given twice, 10 days apart). Ivermectin or pyrantel may be considered.

Courtesy of Dr. James McBain.
Hookworms: Hookworms (Uncinaria spp) are found in pinnipeds. Severe infections are known in fur seals. Newborn fur seal pups are infected via colostrum, and infection usually resolves on its own without intervention. Disophenol (12.5 mg/kg, SC) or ivermectin (100 mcg/kg, SC) have been effective against these parasites.
Crassicauda: Many species of a large spirurida nematode (Crassicauda spp) infect the cranial sinuses, major vessels, kidneys, and mammary gland ducts of cetaceans.
Successful treatments are not documented but are potentially possible with systemic parasiticides. The dual intermediate host requirement of these species in captivity usually means these infections are self-limiting.
Cestodiasis of Marine Mammals
Diphyllobothrium pacificum is commonly found in sea lions, and heavy infection is thought to cause intestinal obstruction. Other cestodes commonly seen include D lanceolatum in phocid seals, Diplogonoporus tetrapterous in all pinnipeds, and Tetrabothrium forsteri and Strobilocephalus triangularis in cetaceans. Cetaceans are also commonly infected with subcutaneous tapeworm cysts throughout the blubber. These usually are the larval forms of tapeworms of sharks and are not usually clinically relevant. Several species of cestodes are reported in sea otters and polar bears but are not known to have clinical significance.
Diagnosis is with fecal floatation or visualization of the parasite in feces.
Administration of praziquantel (10 mg/kg, PO, once) is an effective treatment.
Trematodiasis of Marine Mammals

Courtesy of Dr. James McBain.
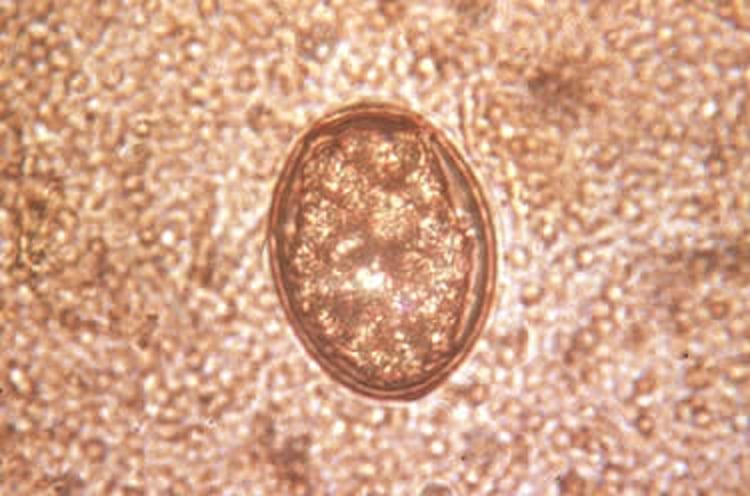
Fluke infections are common in pinnipeds and cetaceans; Nasitrema spp are found in the nasal passages and sinuses of cetaceans.
Ova of these trematodes have been associated with necrotic foci in the brains of animals showing behavioral aberrations and have been incriminated as a cause of localized pneumonia in cetaceans. Infections are often accompanied by halitosis and brown mucus around the blowhole and occasionally by coughing. Diagnosis is based on demonstration of typical operculated trematode ova in blowhole swabs or feces.
Praziquantel (10 mg/kg, PO, two treatments 1 week apart) is usually effective. Reinfection can be prevented by not feeding fresh or live fish.
Courtesy of Dr. James McBain.
Zalophotrema hepaticum is an important hepatic trematode of California sea lions; it causes biliary hypertrophy and fibrosis of the liver.
Signs are usually seen in adults and include icterus, lethargy, and anorexia. Bilirubinemia and increased serum hepatic enzymes are common. Diagnosis is based on identification of trematode ova in the feces.
Treatment with praziquantel (10 mg/kg) or with bithional (20 mg/kg) has been successful.
Various other trematodes infect the stomach, intestines, liver, pancreas, and other abdominal organs of marine mammals. Pancreatic fibrosis due to trematodiasis is a common necropsy finding.
Coccidiosis of Marine Mammals
Coccidia (Eimeria phocae) have been found in harbor seals with a fatal, bloody diarrhea. Clinical disease with this parasite is thought to be rare unless the host is stressed through capture, handling, or husbandry changes. At least two new species of intestinal coccidia have been identified in California sea lions. A coccidian, Cystoisospora delphini, has been reported as the cause of enteritis in bottlenose dolphins; however, some consider the parasite to have been a fish coccidia not associated with the disease. E trichechi reported from the Amazonian manatee (Trichechus inunguis), and E nodulosa reported from the Florida manatee, are also not associated with disease.
These coccidia are probably susceptible to anticoccidial drugs (eg, amprolium) used against other species. (Also see Coccidiosis.)
Sarcocystis of Marine Mammals
Sarcocystis neurona is found in high prevalence in the California population of sea otters and is also commonly found in phocids and California sea lions. A few cases in captive walrus and cetaceans have also been documented. Infection can be subclinical or cause severe encephalitis characterized by generalized neurologic signs. Successful treatment of a captive harbor seal and a few sea otters with neurologic disease has been reported following prolonged treatment with ponazuril (5–10 mg/kg, PO, every 24 hours for 60 days).
Sarcocystis spp have been found in the muscles of many cetacean, otariid, and phocid species and are often not associated with any recognized clinical signs. However, unlike phocids and sea otters, California sea lions may develop debilitating polymyositis resulting in severe muscle wasting. The diaphragm, intercostal muscles and esophagus are often strongly affected and animals may be suspected to have pulmonary disease. Successful treatment has been reported in an adult California sea lion with myositis using ponazuril (10 mg/kg, PO, every 24 hours for 28 days) and prednisolone in the first 5 days of therapy. Following treatment of multiple additional sea lions, a longer treatment regimen is likely warranted, and the finding of megaesophagus is a poor prognostic indicator. Sarcocystis spp have also been associated with fatal necrotizing hepatitis in phocids, otariids, odotocetes, and polar bears.
Toxoplasmosis of Marine Mammals
Toxoplasma gondii infection has been documented in many marine mammal species but is particularly known to infect the California population of sea otters, causing disease that ranges from subclinical infection to severe encephalitis. Fatal meningoencephalitis due to T gondii has also been reported in a Florida manatee and disseminated disease in Antillean manatees. Toxoplasma spp encephalitis is also reported in harbor seals, monk seals, and Northern fur seals. Disseminated toxoplasmosis is reported in California sea lions. Transplacental transmission has been reported in a Risso's dolphin. Toxoplasma gondii is reported from Atlantic bottlenose, Risso’s (Grampus griseus), striped (Stenella coeruleoalba), and spinner dolphins, and serologic evidence of toxoplasmosis is being discovered in an ever-widening array of marine mammal hosts, including polar bears.
Toxoplasmosis should be considered as a differential diagnosis for any marine mammal with CNS disease, and diagnosis in live animals is usually based on serologic testing in addition to clinical signs. Diagnostic testing by PCR assay of blood or CSF may be attempted but may yield false-negative results. Coinfection with other protozoal parasites is not uncommon.
Successful treatment has not been reported, particularly because T gondii often forms drug-resistant tissue cysts in the CNS, but a state of remission may be achieved following oral therapy with ponazuril and trimethoprim-sulfa for 3–4 weeks.






