



Aspergillosis is a sporadic fungal infection due to several environmentally ubiquitous Aspergillus spp. A fumigatus is believed to be the most common; however, multiple other species of Aspergillus are being recognized more commonly with increasing use of molecular techniques for identification.
Aspergillosis is found worldwide and in almost all domestic animals and birds as well as in many wildlife species. It is primarily a respiratory infection that may become generalized; however, tissue predilection varies among species.
The most common forms of aspergillosis are pulmonary infections in poultry and other birds; mycotic abortion in cattle; guttural pouch mycosis and mycotic keratitis in horses; infections of the nasal and paranasal tissues, intervertebral sites, and kidneys of dogs; and sinonasal, sino-orbital, and pulmonary infection in domestic cats.
Because Aspergillus is a ubiquitous fungal organism, infection must be diagnosed by demonstrating tissue invasion; isolation of the organism alone is insufficient.Penicillium is a similar organism to Aspergillus; infections are rare compared to Aspergillus, but clinical presentation, diagnosis, and treatment are identical.
Clinical Findings and Lesions in Aspergillosis in Animals
In birds, aspergillosis is primarily bronchopulmonary, causing clinical signs of dyspnea, gasping, and polypnea accompanied by somnolence, anorexia, and emaciation. Mycotic tracheitis has also been described.
Torticollis and disturbances of equilibrium occur when infection disseminates to the brain. Yellow nodules of varying size and consistency or plaque lesions are found in the respiratory passages, lungs, air sacs, or membranes of body cavities. Furlike mycelial growth of fungus may be found on the thickened walls of air sacs.

Courtesy of Dr. Maria Dashek.
Other species with bronchopulmonary aspergillosis may have nodular lesions in the lungs or an acute pneumonia accompanied by serosanguineous fluid in the pleural cavity and a fibrinous pleuritis. Among nonpoultry avian species, penguins appear to be overrepresented.
In ruminants, infection may be subclinical, appear in a bronchopulmonary form, cause mastitis, or cause placentitis and abortion. Mycotic pneumonia may be rapidly fatal. Clinical signs include pyrexia; rapid, shallow, stertorous respiration; nasal discharge; and a moist cough. The lungs are firm, heavy, and mottled and do not collapse.
In subacute to chronic mycotic pneumonia, the lungs contain multiple discrete granulomas, and the disease grossly resembles tuberculosis.
In the absence of pneumonia, infected cows generally have no clinical signs except for abortion; a dead fetus is aborted at 6–9 months gestation, and the fetal membranes are retained. Lesions are found in the uterus, fetal membranes, and often the fetal skin.
In the uterus, the intercaruncular areas are grossly thickened, leathery, and dark red to tan. They contain elevated or eroded foci covered by a yellow-gray adherent pseudomembrane. Maternal caruncles are dark red to brown, and the adherent fetal cotyledons are markedly thickened. Cutaneous lesions in aborted fetuses consist of soft, red to gray, elevated, circumscribed lesions that resemble ringworm.
Mycotic mastitis often presents as a sudden decrease in milk production from one or more quarters; the gross appearance of milk may not be abnormal. Affected quarters are often firm.

Courtesy of Dr. Sameeh M. Abutarbush.
In horses, epistaxis (sometimes fatal) and dysphagia are common complications of guttural pouch mycosis. The infected guttural pouch is characterized by necrotizing inflammation and is thickened, hemorrhagic, and covered by a friable pseudomembrane and/or fungal mats. The fungal lesions grow on and can erode through the internal carotid, external carotid, and/or maxillary arteries as they pass through the guttural pouch. Mycotic rhinitis characterized by dyspnea and nasal discharge has also been described.
Aspergillosis can be a rapidly fatal disease associated with diffuse pulmonary invasion, especially in foals. In these cases, acute enteritis or colitis is often a predisposing factor. The colitis is thought to result in a profound neutropenia that decreases the immunocompetence of the host, followed by the invasion of Aspergillus from disrupted intestinal mucosa.
Locomotor and visual disturbances, including blindness, may occur when the infection spreads to the brain and optic nerve.
Aspergillus spp are also common in equine eyes. Mycotic keratitis may present as a nonhealing or melting corneal ulcer, and mycotic keratitis is a recognized complication of using ophthalmic products containing glucocorticoids in the equine eye.


Courtesy of Dr. Louise Bauck.
In dogs, aspergillosis is typically localized to the nasal cavity or paranasal sinuses. Nasal aspergillosis is evident mainly in dolichocephalic breeds; it begins in the caudal region of the ventral maxilloturbinate with clinical signs of nasal pain, ulceration, and depigmentation of the nares; sneezing/reverse sneezing; unilateral or bilateral sanguinopurulent nasal discharge; and/or epistaxis.
Frontal sinus osteomyelitis may occur. The cribriform plate may be affected, resulting in CNS signs.
Gross lesions vary considerably with the site of infection; however, the mucosa of the nasal and paranasal sinuses may be covered by a layer of necrotic material and gray-white fungal growth. The mucosa and the underlying bone may be necrotic with loss of bone definition on radiographs or CT. Dogs may also acquire fungal ear infections associated with Aspergillus spp.
Disseminated invasive aspergillosis in dogs occurs most often in middle-aged female German Shepherd Dogs and most often involves A terreus. The clinical signs of disseminated aspergillosis may include lethargy, lameness, anorexia, weight loss, muscle wasting, pyrexia, hematuria, urinary incontinence, generalized lymphadenopathy, and neurologic deficits, including head tilt, ataxia, and proprioceptive deficits.
Lesions are frequently found in the abdominal and thoracic lymph nodes, kidneys, spleen, and vertebrae. Discospondylitis is common.
In cats, sinonasal and sino-orbital disease occur most often. Aspergillosis is rare in cats compared with dogs. Sinonasal disease, usually associated with A fumigatus, can present similarly to the disease in dogs.
However, sino-orbital disease, associated with A felis, can be aggressive, often causing severe facial swelling, exophthalmos, corneal ulceration, miosis, retrobulbar fungal granulomas, and lysis of orbital bones. In some cases, a mass in the pterygopalatine fossa or ulceration of the hard palate may be evident. The CNS may be invaded, causing neurologic signs.
Diagnosis in Aspergillosis and Penicilliosis in Animals
Demonstration of tissue invasion
Guttural pouch endoscopy in horses
Antigen assays, immunohistochemistry, and molecular diagnostics
In dogs and cats, CT or MRI may be necessary
In poultry, respiratory signs of aspergillosis such as dyspnea or wheezing should prompt an investigation in which one or more birds are sacrificed for diagnostic purposes; necropsy examination should evaluate lungs and air sacs in particular. Fungal granulomas may be identified grossly or histologically For pet or zoo birds, testing may include radiology, CT, or MRI to identify fungal granulomas or pulmonary infiltrates; biopsy may be necessary to confirm infection.
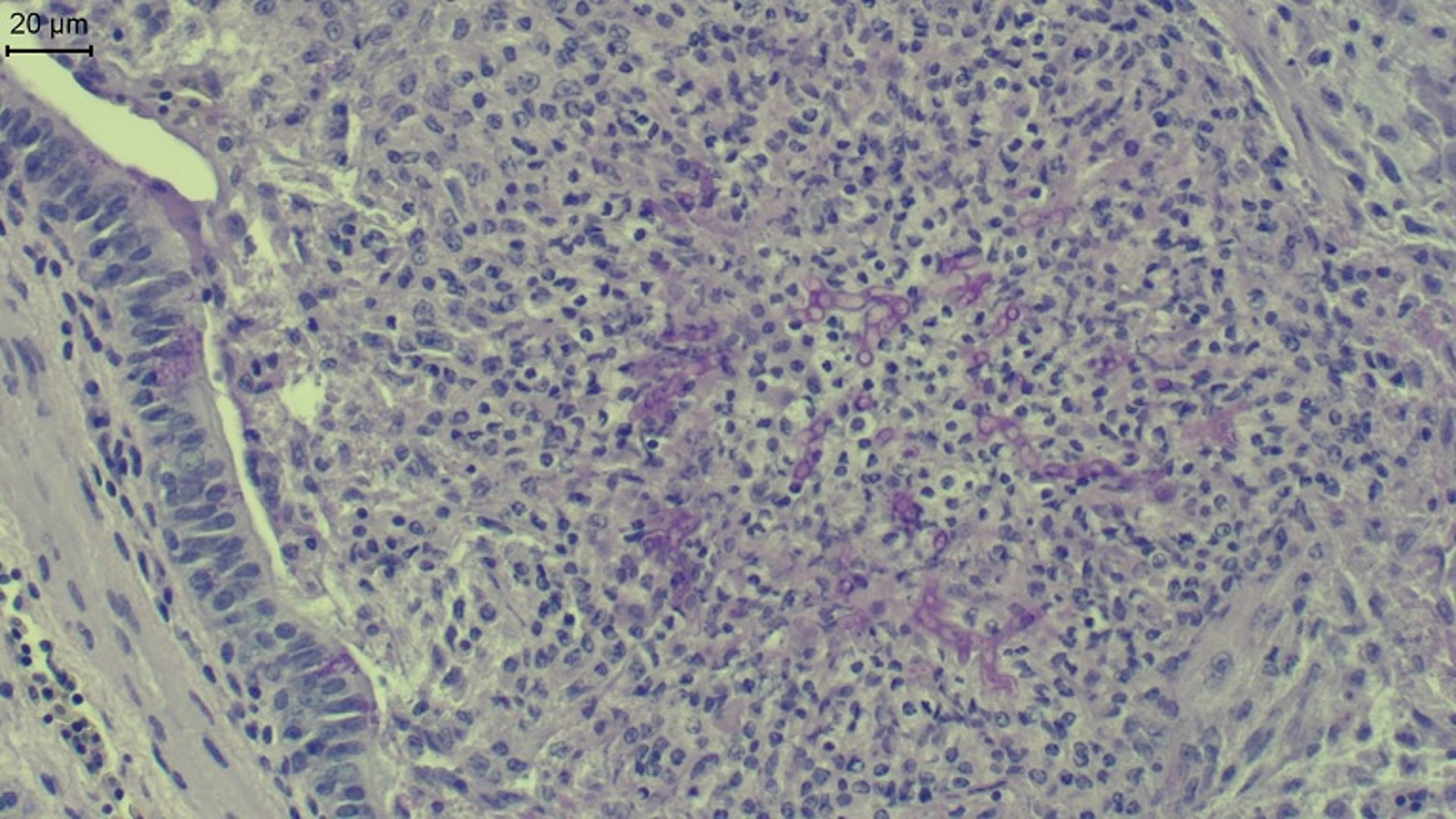
In ruminants, antemortem diagnosis of pulmonary aspergillosis is seldom made. Postmortem examination may demonstrate fungal granulomas or firm lungs that fail to collapse; hyphae will be evident on histopathologic examination.
In ruminant mycotic abortion, identification of hyphae on histopathology of placenta or fetal skin is diagnostic. Culture of the organism from fetal abomasal contents may also be useful, but culture from placenta is not diagnostic because of environmental contamination.
For mycotic mastitis, culture of milk from a sterilely obtained sample may be helpful if the organism is present in heavy pure growth. Mycotic mastitis cases are often associated with reuse of intramammary infusion devices, which become contaminated in the barn environment.

Courtesy of Dr. Rosalie Ierardi.

Courtesy of Dr. Fred Williams III.
Radiographs in dogs with nasal aspergillosis may show generalized radiolucency of the nasal cavity secondary to turbinate tissue destruction. Frontal bone or maxillary osteomyelitis is present in as many as 80% of dogs. Cross-sectional imaging via CT or MRI is more sensitive than plain radiographs in demonstrating consistent changes and extent of lesions.
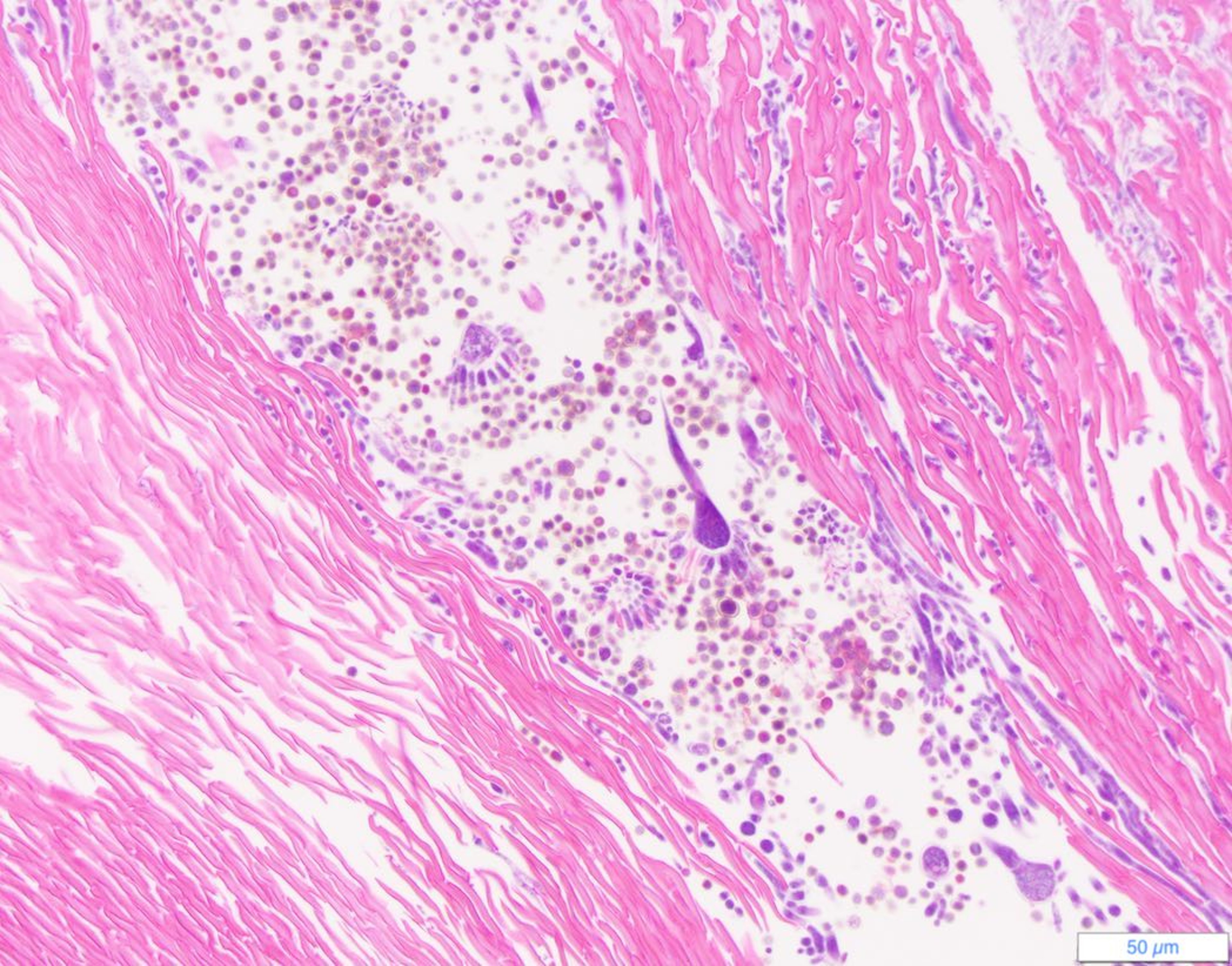
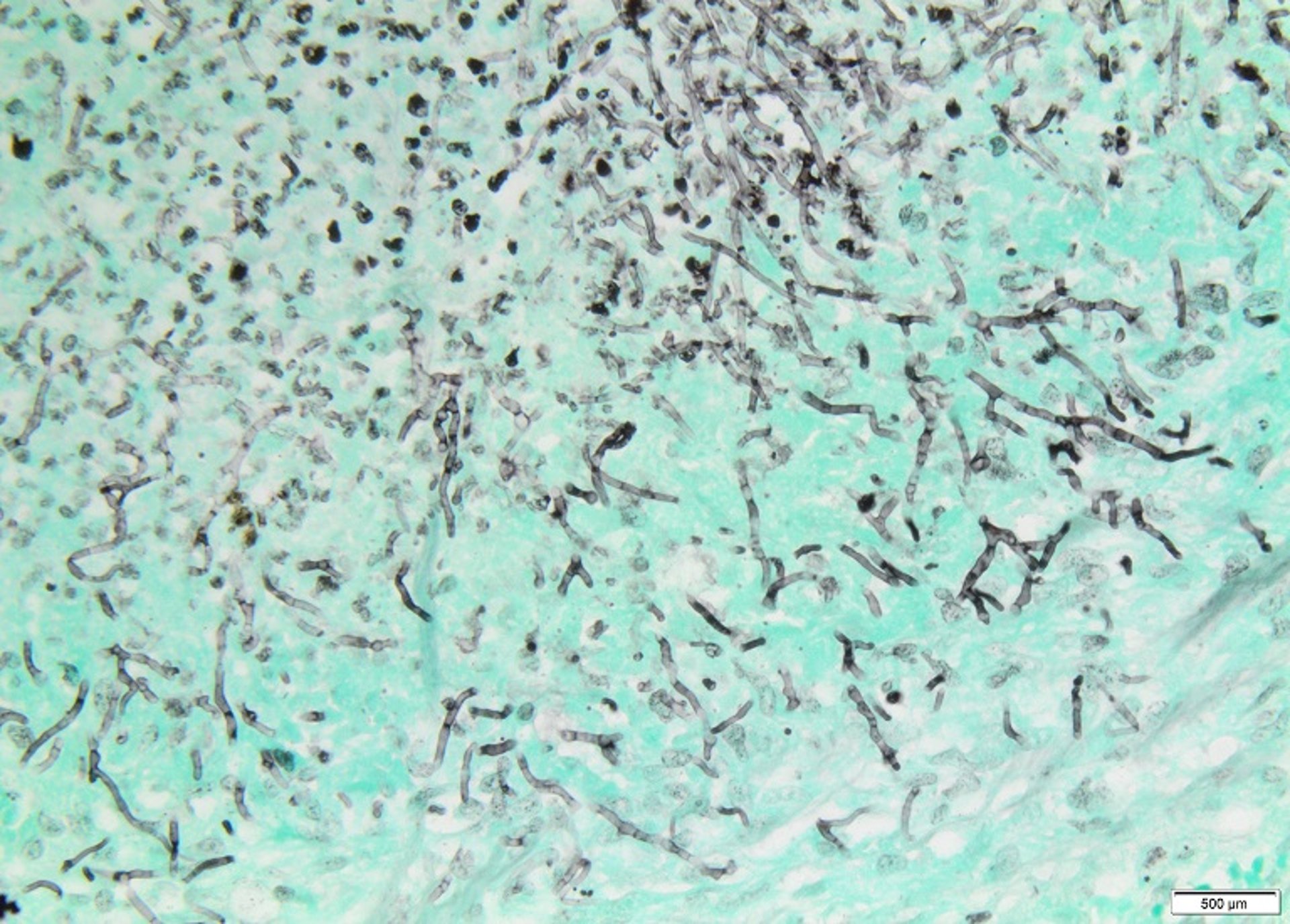
Visualization of fungal plaques by rhinoscopy together with either mycologic or radiographic evidence of disease is often how a diagnosis is made. A diagnosis based on culture results alone is not appropriate, because aspergilli are ubiquitous and can be isolated from the nasal cavities of healthy dogs. Positive culture results should be supported by demonstration of narrow, hyaline, septate, branching hyphae within lesions.
Serologic assays are generally considered unreliable because of frequent false negative results. A urine or serum galactomannan assay is sensitive for disseminated aspergillosis in dogs but cross-reacts with other fungal species.
Many cases of canine disseminated aspergillosis have an extensive history of failed antimicrobial treatment before a definitive diagnosis is achieved. Dogs with systemic disease usually have neutrophilia, often with a left shift, and a nonregenerative anemia. Azotemia, hyperglobulinemia, hypoalbuminemia, and hypercalcemia are common. Ultrasound usually reveals abdominal lymphadenopathy and renal lesions.
Systemic disease is usually diagnosed by culture of the organism, often from urine. MRI examination of dogs with CNS aspergillosis may not demonstrate CNS lesions. Histopathologic evaluation of biopsy specimens is insufficient to definitively identify Aspergillus; immunohistochemistry, culture, or molecular diagnostics are necessary. Speciation of Aspergillus often involves PCR amplification and sequencing of several genes but may be necessary for appropriate treatment and prognosis.
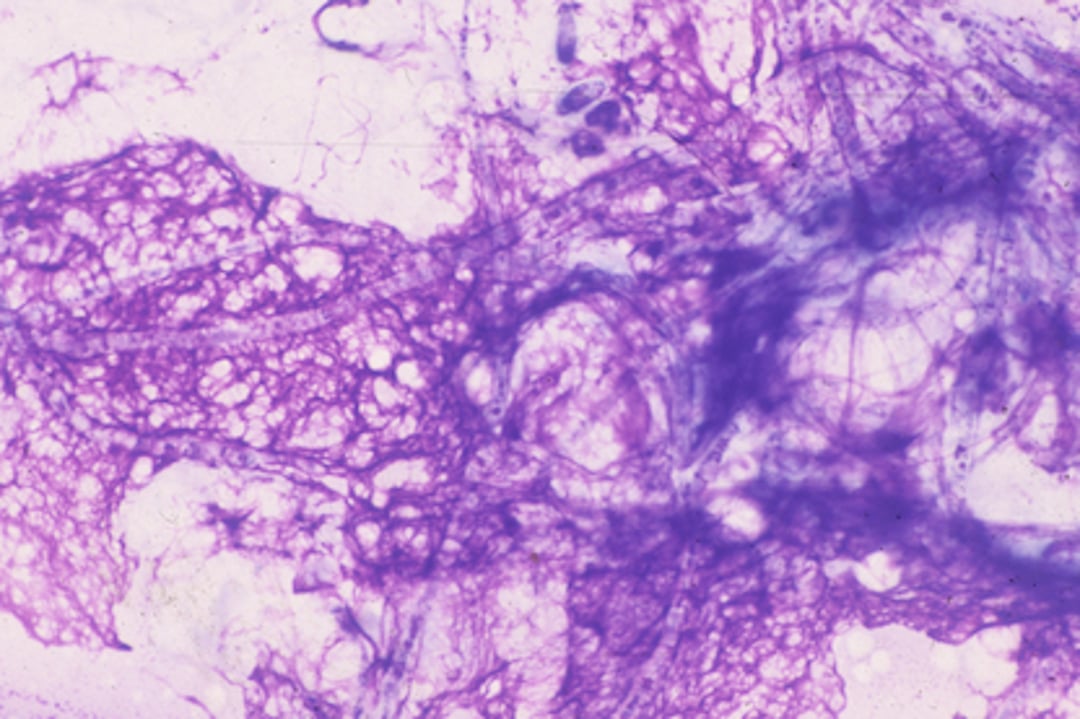
In horses, epistaxis not associated with exercise is the most common clinical sign of guttural pouch mycosis and should prompt endoscopic evaluation of the guttural pouches. Endoscopic visualization of gray-black fungal mats within the guttural pouch is considered diagnostic. Sampling the lesions is not necessary in this location and would be dangerous; the gross lesion is diagnostic for Aspergillus infection.
Equine mycotic keratitis is diagnosed via cytology of a corneal scraping; culture alone is insufficient evidence.
Treatment in Aspergillosis and Penicilliosis in Animals
Topical antifungal treatment for nasal and ophthalmic aspergillosis; systemic azoles or amphotericin B for disseminated disease
Surgery possible for equine guttural pouch mycosis
First-line treatments: itraconazole, voriconazole, posaconazole, liposomal amphotericin B, and terbinafine
In poultry, husbandry changes are often sufficient to decrease prevalence of aspergillosis, especially better ventilation and decreased contamination via feed or environment. For individual birds, oral antifungals have been recommended; however, little information exists on appropriate dose and interval.
In ruminants, treatment of pulmonary aspergillosis is seldom attempted because of rapid clinical progression. Evaluation of feed and environment should be undertaken to identify sources of contamination on premises affected by pulmonary cases or mycotic abortion. Bovine mastitis has rarely been treated successfully with combined intra-arterial and intramammary injection with miconazole, although this is extra-label use; most cases fail to respond to treatment.
In dogs, debridement of lesions followed by topical treatment is considered the treatment of choice for nasal and paranasal aspergillosis. Several surgical techniques and drug regimens have been used with varying success.
Clotrimazole formulated in a polyethylene glycol base is generally considered the first-line treatment. It can be administered via indwelling tubes trephined into the frontal sinuses or via the nares as a single infusion.
If infusion is via the nares, Foley catheters are used to instill 0.5 g in each side of the nasal cavity. The infused solution is left in place for 1 hour, during which the dog’s position is changed periodically to maximize penetration. There is an ~80% success rate using local infusions in this manner.
Enilconazole, 10 mg/kg, instilled every 12 hours for 7–14 days via tubes implanted surgically into the frontal sinuses, has also been used with a similar success rate.
Drugs administered systemically have included ketoconazole, itraconazole, fluconazole, voriconazole, and posaconazole. Fluconazole (2.5–10 mg/kg, divided every 12 hours) and itraconazole (5–10 mg/kg every 24 hours) are cost-effective options. Ketoconazole (5–10 mg/kg, every 12 hours for 6–8 weeks), although cost-effective, is not as effective clinically. Voriconazole (3–6 mg/kg every 24 hours) is probably the most effective of the azole antifungals for treating aspergillosis; however, the cost is much higher than that of the other choices.
Relapse of systemic aspergillosis is common regardless of treatment, and prognosis is guarded, especially in cases with CNS involvement.
Feline sino-orbital aspergillosis due to A felis may be less responsive to azole treatment than disease due to A fumigatus, emphasizing the need for definitive speciation.
In horses, guttural pouch mycosis is most effectively treated by ligation or embolization of the internal carotid artery. Surgical exposure and curettage have also been used; however, the location of lesions over the large vessels in the guttural pouch make this a risky endeavor.
Topical natamycin and oral potassium iodide have been reported effective in some equine cases of Aspergillus infection, but topical treatment alone is usually unrewarding. Itraconazole (3 mg/kg, every 12 hours for 84–120 days) has been effective in Aspergillus rhinitis in horses. Dysphagia may not resolve after treatment of guttural pouch mycosis.
Equine mycotic keratitis may respond to topical antifungal treatment but may require surgical intervention or enucleation. Topical voriconazole, miconazole, or natamycin is commonly used.
Key Points
Aspergillosis has many different clinical signs in veterinary species; practitioners should be familiar with the presentation(s) of disease in their species of interest.
Diagnosis often relies on demonstration of fungal tissue invasion because the fungus is ubiquitous in the environment.
Azole antifungals are generally the treatment(s) of choice.






