



Coccidioidomycosis (valley fever) is a dustborne, noncontagious infection due to Coccidioides spp fungi. These fungi form mycelial mats in shallow arid soil; the mycelium fragments form arthrospores.
Coccidioidomycosis infections are most common in arid and semiarid regions of the southwestern US and similar areas of Mexico and Central and South America, though cases have been reported from nonendemic regions. Although many species of animals, including humans, are susceptible, dogs most commonly develop clinical signs of coccidioidomycosis. Infections are caused by Coccidioides immitis and C posadasii.
Inhalation of fungal arthrospores is the most common mode of infection, and spores may be carried on dust particles. Epidemics may occur when rainy periods are followed by drought, resulting in dust storms. Infection via cutaneous inoculation has been reported but is rare.
Clinical Findings and Lesions in Coccidioidomycosis in Animals


Courtesy of Dr. John Prescott.

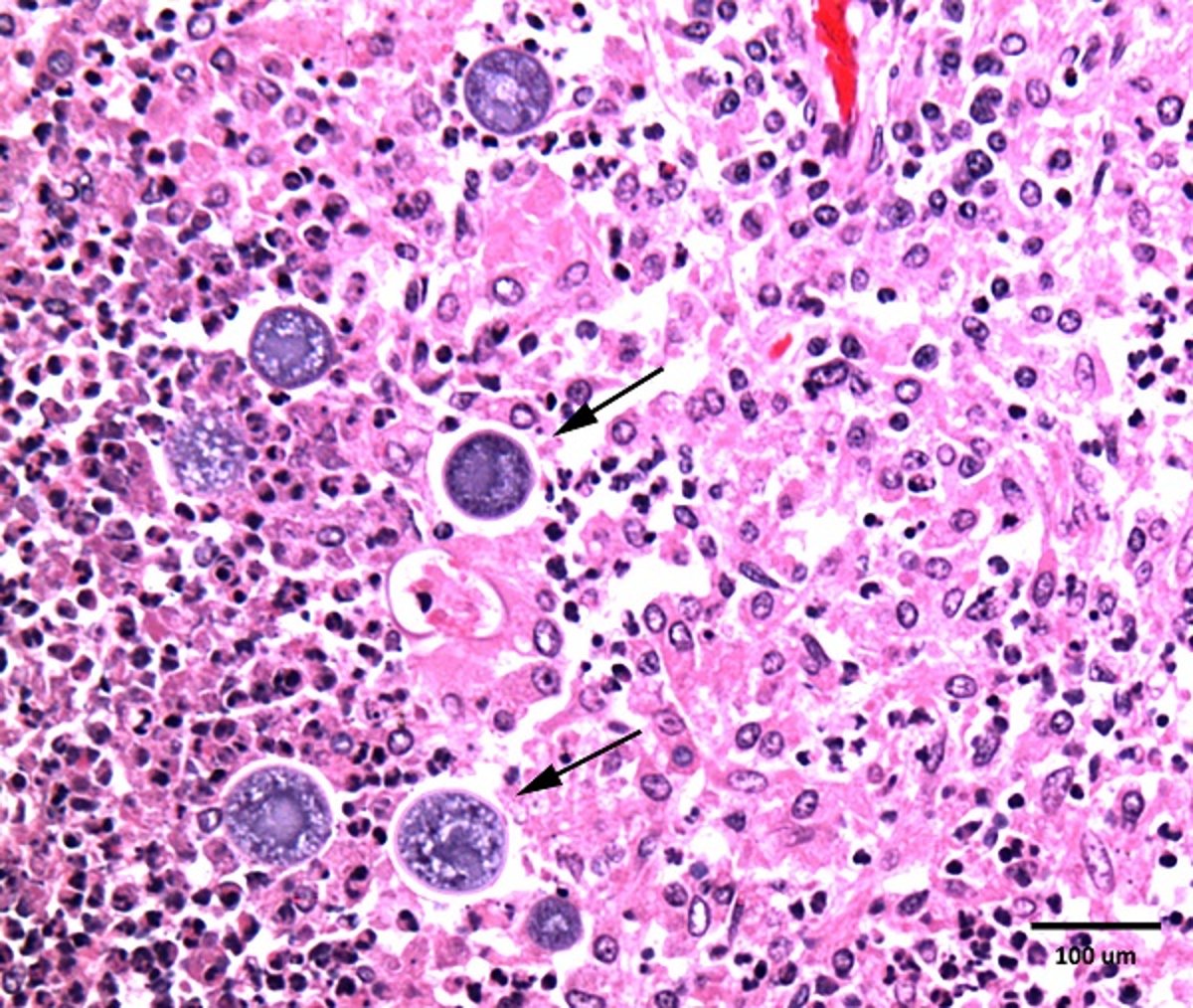
Courtesy of Dr. Dae Young Kim.
Coccidioidomycosis varies from inapparent to progressive, disseminated, and fatal. Coccidioidomycosis is primarily a respiratory disease that ranges from self-limiting to chronic. Dissemination occurs in ~20% of canine infections, with many tissues affected, especially brain, eyes, skin, bone, and joints. Most, but not all, dogs with disseminated disease will display signs referable to more than one organ system.
Clinical signs can vary greatly depending on organ involvement and severity of infection. Patients with pulmonary-only disease often show cough, lethargy, inappetence, fever, and tachypnea. Dogs with CNS involvement most often demonstrate seizures; vestibular signs, asymmetric cranial nerve signs, behavior changes and compulsive circling are also observed in these patients.
In addition, dogs with disseminated disease may have anorexia, cachexia, lameness, skin lesions, subcutaneous masses, enlarged joints, heart failure, ascites and/or ocular abnormalities. Cats infected with C immitis most often present with dermatologic signs (draining skin lesions, subcutaneous granulomatous masses, abscesses), fever, inappetence, and weight loss. Less common clinical signs in cats include respiratory (dypsnea), lameness, neurologic, and ophthalmologic abnormalities.
Clinical coccidioidomycosis is uncommon in large animal species. Placental infection leading to abortion and osteomyelitis has been described in horses. Ruminants and pigs may have subclinical infections with lesions restricted to foci in the lungs and thoracic lymph nodes. Presumed transplacental infection has been reported in a llama cria.
Gross lesions may be limited to the lungs, mediastinum, and thoracic lymph nodes or may be disseminated to various organs. Lesions are discrete nodules of variable size, have a firm gray-white cut surface, and resemble those of tuberculosis. The nodules are pyogranulomas composed of epithelioid and giant cells, and the center of some foci may contain purulent exudate and fungal organisms. Some lesions may have mineralized foci.
Fungal organisms are found in tissue as spherules ranging from 20–200 mcm in size but may be sparse in tissue. Spherules can contain hundreds of endospores.
Diagnosis of Coccidioidomycosis in Animals
Histopathologic discovery of spherules in tissue
Serologic testing: antibody agar gel immunodiffusion (AGID), enzyme immunoassay (EIA), or lateral flow assay (LFA)
MRI
CSF cytology and EIA testing
In endemic areas, coccidioidomycosis should be considered in dogs with chronic bronchopulmonary disease, when pulmonary nodules and enlarged lymph nodes are found on thoracic radiographs, or when CNS signs develop. Definitive diagnosis of this organism can be challenging; in some cases response to antifungal treatment may be the only evidence for the diagnosis.
On histopathology, the spherules vary in size and appear as relatively large (20–80 mcm, up to 200 mcm) spherules with a double-contoured wall. The mature spherules contain endospores 2–5 mcm in diameter. Diagnosis is established by demonstrating the spherules in tissues, but this can be challenging or impossible to achieve by antemortem sampling, particularly when the CNS is affected.
Fungal organisms are seldom found in aspirates and impression smears. Serum can also be laboratory tested by agar gel immunodiffusion (AGID) or enzyme immunoassay (EIA) for IgG and IgM antibodies that are sensitive and specific. A sensitive point-of-care lateral flow immunoassay is also available that can provide results in 15 minutes.
A presumptive diagnosis can be made when serologic testing is positive in a patient with consistent clinical signs; however, many clinically normal animals may also have positive serology, due to prior exposure or subclinical infection.
Antigen testing for coccidioidomycosis has proven largely insensitive, but recent work indicates that EIA antigen testing of CSF is positive in some cases. EIA antibody testing of CSF may also be useful, but some patients with brain disease other than coccidioidomycosis will also be positive for CSF antibodies.
MRI can be useful for diagnosis of CNS coccidioidomycosis. Two general MRI presentations are described: the majority of patients show a discrete, single, contrast-enhancing granuloma with perilesional edema, usually in the cerebrum. Differentiating these coccidioidomycosis granulomas from masses of other origin may still prove challenging. A second small group of patients will instead demonstrate bilaterally symmetric encephalitis of the frontal lobes and caudate nuclei, best seen on T2 sequences.
Attempts to culture the fungus should be restricted to those biosafety level-3 laboratories equipped to handle such dangerously infective cultures.
Treatment of Coccidioidomycosis in Animals
Fluconazole or itraconazole for 6-12 months
Surgery
Disease may be self-limiting; however, if chronic respiratory signs, CNS signs or multisystemic disease is present, then longterm antifungal treatment is needed. Compounded formulations of azoles may not contain adequate therapeutic doses, and should be avoided.
Fluconazole (5–10 mg/kg every 24 hours) is the most commonly used drug. Itraconazole (10 mg/kg every 24 hours) is also commonly used to treat dogs with coccidioidomycosis but may be more expensive and have a higher incidence of adverse effects.(1,2,3,4,5) It may be the better choice for patients with bone involvement. Numerous investigations in animals indicate that itraconazole compounded from the bulk drug substance is not bioavailable and should not be used for serious mycotic infections.
Amphotericin B has been recommended, but it is highly nephrotoxic. It may be indicated in patients that either do not improve or are unable to tolerate the azole antifungals. No specific treatment recommendations have been made for coccidioidomycosis in large animals; however, successful treatment of horses has been reported with fluconazole and itraconazole.
Surgical excision of granulomas may be successful when feasible.
The prognosis ranges from guarded to good; a recent report indicated a favorable response to chronic treatment in a majority of dogs with CNS involvement.
Key Points
Coccidioidomycosis is an endemic fungal disease in arid regions of the Americas; dogs are the most susceptible veterinary species.
Clinical signs relate to chronic respiratory disease, but dissemination to skin, bones, eyes, and other tissues can occur.
Diagnosis can be made by serologic testing or demonstration of the fungal spherules in tissue.
References
Mawby DI, Whittemore, JC, Fowler LE, Papich MG. Comparison of absorption characteristics of oral reference and compounded itraconazole formulations in healthy cats. JAVMA. 2018;252(2):195-200.
Renschler J, Albers A, Sinclair-Mackling H, Wheat LJ. Comparison of compounded, generic, and innovator-formulated itraconazole in dogs and cats. JAAHA. 2018;54(4):195-200.
Smith JA, Papich MG, Russell G, Mitchell MA. Effects of compounding on pharmacokinetics of itraconazole in black-footed penguins (Spheniscus demersus). J Zoo Wild Med. 2010;41(3):487-495.
Molter CM, Zuba JR, Papendick R. Cryptococcus gattii osteomyelitis and compounded itraconazole treatment failure in a Pesquet's parrot (Psittrichas fulgidus). J Zoo Wild Med. 2014;45(1):127-133.
Bunting EM, Abou Madi N, Cox S, Martin-Jimenez T, Fox H, and Kollias GV. Evaluation of oral itraconazole administration in captive Humboldt penguins (Spheniscus humboldti). J Zoo Wild Med. 2009;40(3):508-518.
For More Information
Butkiewicz CD, Alcott CJ. Renschler J, Wheat LJ, Shubitz LF. The utility of Coccidioides antigen and antibody detection in cerebrospinal fluid in the diagnosis of canine central nervous system coccidioidomycosis. Am J Vet Res. 2021;83(1):59-63. doi: 10.2460/ajvr.21.08.0121.
Kelley AJ, Stainback LB, Knowles KE, Moore TW, Plummer SB, Shoup OR. Clinical characteristics, magnetic resonance imaging features, treatment, and outcome for presumed intracranial coccidioidomycosis in 45 dogs (2009-2019). J Vet Intern Med. 2021;35(5):2222-2231. doi: 10.1111/jvim.16243. Epub 2021 Aug 19.






