

Fungal diseases are common in companion birds. Often, they are a secondary infection in an already ill or immunocompromised bird. The most common fungal diseases are respiratory tract infections caused by Aspergillus spp and GI tract infections caused by Candida spp. Macrorhabdus is an unusual fungus that affects the GI tract and occurs most commonly in small pet birds (budgerigars, lovebirds, finches, parrotlets, and cockatiels).
Candidiasis
Candidiasis is a common fungal disease, seen mostly in young or immunocompromised birds. It most commonly affects unweaned chicks. Birds on broad-spectrum antimicrobials are most at risk. Often, candidiasis is secondary to poor husbandry and an unclean environment. Clinical signs include anorexia, crop stasis, white plaques in the oral cavity, regurgitation, and weight loss. Thickening of the crop may develop ("Turkish-towel" appearance). Treatment options include nystatin or fluconazole.
The etiologic agent is the opportunistic yeast Candida albicans, which commonly affects the GI tract. Although C albicans is the most common isolate, others including C tropicalis, C parapsilosis, C glabrata, and Hansenula spp may also be found and may be refractory to treatment.
C albicans is not generally considered a primary pathogen. Small numbers of Candida are commonly found in the GI tract of birds and may become pathologic when normal digestive flora are disrupted by immunosuppression. (Also see Candidiasis in Poultry.)
Neonatal cockatiels are considered most susceptible. Infection may be endogenous, because of yeast overgrowth, or caused by oral inoculation of large numbers of Candida, either by parental feeding or by hand feeding with utensils that are inadequately cleaned.
Clinical Findings of Candidiasis in Pet Birds
Clinical signs in adult birds are typically mild and may include mild weight loss, lethargy, and dull plumage. Young birds may have more severe disease, especially if they are immunocompromised. Clinical signs in juvenile birds include anorexia, crop stasis, white plaques in the oral cavity, regurgitation, and weight loss. Localized infections in the oral cavity can lead to difficulty swallowing or halitosis. With severe infections, there may be complete crop and GI stasis. Thickening of the crop may develop ("Turkish-towel" appearance). The proventriculus and ventriculus can also become infected and lead to more severe clinical signs such as weight loss, regurgitation, diarrhea, and depression. See table Differential Diagnoses for Regurgitation in Pet Birds for differential diagnoses for regurgitation in birds.
Differential Diagnoses for Regurgitation in Pet Birds
Problem | Species Commonly Affected | Common Agents (if known) | Typical Signs |
|---|---|---|---|
Toxicosis | Various | Lead, zinc, pesticides, medications | Vomiting, abnormal droppings, lethargy, possible CNS signs |
Oral upper GI irritation | Cockatiels, various | Plants (Pothos, Philodendron), various medications, other caustic materials | Lethargy, ptyalism, passive regurgitation of water, erythema of tongue and pharynx |
Proventricular dilatation syndrome | Macaws, miniature macaws, African grey parrots, cockatoos, others | Avian bornavirus | Weight loss, vomiting, seeds in feces, possible CNS signs |
Bacterial GI infections | Various | Gram-negative bacteria | Vomiting, watery droppings, lethargy |
Candidiasis | Cockatiels, lovebirds, others | Candida spp | Regurgitation, crop distention, oropharyngeal and crop lesions |
Trichomoniasis | Budgerigars, cockatiels, doves, others | Trichomonas spp | Regurgitation, mouth and crop lesions (white matter), mucus in crop |
Ventricular, proventricular, or crop obstruction | Cockatoos, macaws, Eclectus parrots, cockatiels, others | Wood shavings, corncob bedding, other bedding, fibers, foreign bodies, ascarids | Vomiting, depression, weight loss |
Proventricular adenocarcinoma | Various | Neoplasm | Vomiting, weight loss, lethargy, severe pain, sudden death |
Internal papillomatosis | Amazons, macaws | Psittacine herpesvirus 1 | Vomiting, straining to defecate, secondary cloacal and choanal infections |
Abdominal mass | Budgerigars | Renal or gonadal mass—usually neoplasia | Weight loss, lameness, vomiting |
Behavioral | Various | Courtship behavior | Regurgitation on mirror, owner, toy, or cagemate |
Diagnosis of Candidiasis in Pet Birds
Diagnosis of candidiasis is by identifying Candida spp on a Gram, Romanowsky-type, or new methylene blue stain of the feces, crop contents, or regurgitated material. Scrapings or impression smears may also be performed to diagnose suspected yeast infections of the skin. In severe cases, when tissue invasion has occurred, the budding yeast will produce hyphae that can be seen in scrapings obtained from the crop or pharynx, or from the feces.
Treatment of Candidiasis in Pet Birds
Often, candidiasis is secondary to poor husbandry and an unclean environment. If a reservoir of exogenous Candida is present (eg, poor nest box or feeding tube hygiene), then eliminating the source of the Candida is critical. In neonates with crop stasis, the crop must be emptied and smaller amounts fed until the crop stasis has resolved. Metoclopramide may help crop motility and prevent regurgitation.
After identifying and resolving any predisposing factors, treatment with nystatin or fluconazole should be initiated. Nystatin (300,000 IU/kg, PO, 2 times a day) is commonly used for treatment because of its low cost and low toxicity. Disadvantages are poor taste and large volume required. Because it is fungistatic and not absorbed from the GI tract, it is only effective when in direct contact with infected tissue, so it should be administered 3 times a day before feeding. If the yeast is resistant to nystatin or the bird is difficult to medicate, then fluconazole (20 mg/kg, PO, every 48 hours) is available for systemic treatment.
Flock treatment has historically been accomplished with use of chlorhexidine at 10 mL/gal. of drinking water for 1–3 weeks. Because chlorhexidine is a disinfectant, its use will also deplete the normal digestive flora. Acidification of the upper GI tract by use of apple cider vinegar has also been reported to resolve Candida overgrowth.
See table Antifungals Used in Pet Birds for some antifungal drugs used in pet birds.
Antifungals Used in Pet Birds
Antifungala | Dosage | Route, Frequency |
|---|---|---|
Amphotericin B | 1 mg/kg intratracheal (dilute to 1 mL with sterile water; 0.25–1 mg/mL sterile water for nebulization | Given intratracheally every 8–12 h; nebulized 10–20 minutes, 2 times a day |
Amphotericin B | 1.5 mg/kg | IV, 3 times a day |
Amphotericin B suspension | 100 mg/kg | PO, 2 times a day × 30 days |
Clotrimazole | 2 mg/kg | Given intratracheally, once daily × 5 days |
Clotrimazole | 10 mg/mL (1%) | Nasal flush; nebulized for 30 minutes 2 times a day |
Enilconazole | 1 mg (0.05 mL/kg of a 1:10 dilution) | Given intratracheally, once daily × 7–14 days |
Enilconazole | 0.1 mL/kg in 5 mL sterile water | Nebulize for 30 minutes, 5 days on, 2 days off |
Fluconazole | 5–15 mg/kg | PO, 2 times a day |
Fluconazole | 20 mg/kg | PO, every 48 hours × 3 treatments |
Griseofulvin | 10 mg/kg | PO, 2 times a day |
5-Flucytosine | 20–75 mg/kg | PO, 2 times a day |
F-10b (quaternary ammonium disinfectant) | 1.5/400 mL distilled water | Nebulization for cutaneous and possibly respiratory fungus |
Itraconazole | 5–10 mg/kg | PO, once to twice daily (lower dosage, and use cautiously in African grey parrots) |
Ketoconazole | 10–30 mg/kg | PO, 2 times a day |
Terbinafine | 10–15 mg/kg 1 mg/mL solution | PO, 2 times a day Nebulization for 30 minutes |
Nystatin oral suspension (100,000 U/mL) | 300,000–600,000 U/kg | PO, 2 times a day |
Voriconazole | 12–18 mg/kg | PO, 2 times a day |
a Most are unapproved for use in birds, and caution is indicated. | ||
b Quaternary ammonium and biguanidine compound; nontoxic, ampholytic surfactant | ||
Aspergillosis
Aspergillosis is an opportunistic infection that typically occurs in immunocompromised birds. Signs include depression, anorexia, voice change, increased respirations, and/or dyspnea. Diagnosis is based on species, clinical signs, blood tests, and diagnostic imaging. A CBC may reveal leukocytosis and monocytosis. Airsacculitis in often present on radiographs. Treatment is with itraconazole, voriconazole, or amphotericin B. Fungal granulomas may require surgical resection.
Aspergillosis is an opportunistic infection that typically occurs in immunocompromised hosts (malnutrition, especially vitamin A deficiency) or when birds are exposed to large numbers of aerosolized spores. It is not transmitted bird-to-bird. Aspergillus fumigatus is the most common species isolated; A flavus and A niger are also found. Rhizopus, Penicillium, Mucor, and Scedosporium apiospermum can cause similar signs and are more difficult to diagnose and treat.
Predisposing factors for developing infection include species predilection (African grey parrots, Amazon parrots, cockatiels, and macaws), aspiration of food or medications, immunosuppression (underlying disease), moldy bedding or feed, and use of corticosteroids. Poor hygiene and inadequate ventilation, especially in warm, humid climates, can also increase the incidence of disease.
Clinical Findings of Aspergillosis in Pet Birds

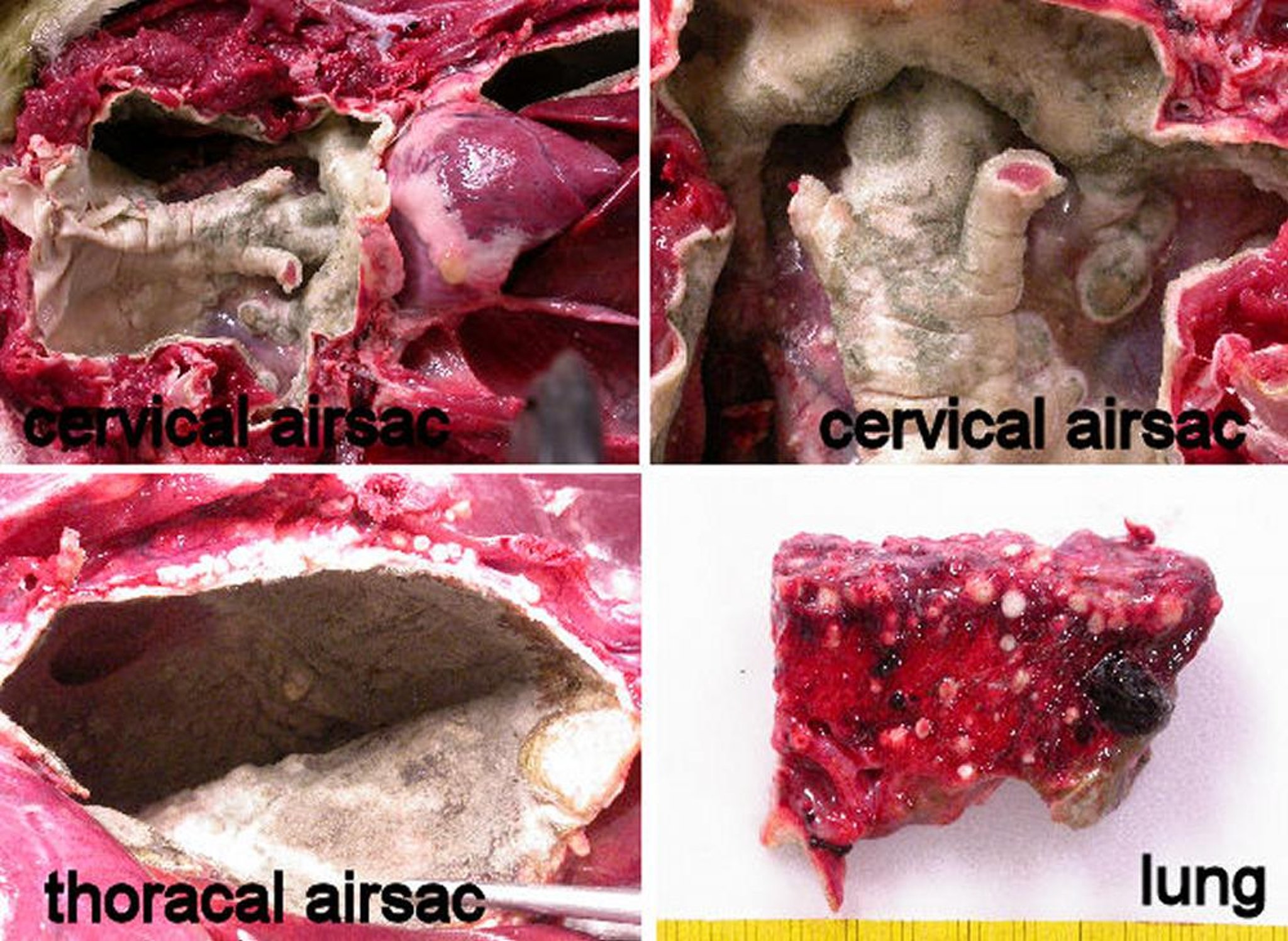
Aspergillosis granulomas in the air sacs of a hawk.
Courtesy of Dr. Gerry Dorrestein.
Clinical signs of aspergillosis depend on the site of infection. Most infections occur in the upper respiratory tract, air sacs, lungs, trachea, and syrinx. Systemic infections occur when the infection spreads to internal organs, including bone, liver, kidneys, or brain. Eye and skin infections can also occur. Anorexia and weight loss are often present. Respiratory signs may include dyspnea, tail bobbing, exercise intolerance, and voice change. Rhinitis caused by Aspergillus appears similar to bacterial rhinitis or sinusitis. A Gram stain or modified Wright’s stain of lesions or debris often demonstrates fungal hyphae. Infraorbital sinusitis caused by aspergillosis often must be surgically debrided before therapy is effective. Extensive or chronic fungal sinusitis may lead to osseous changes and permanent malformation of the upper respiratory architecture. Extension of infection to the brain can cause CNS signs.

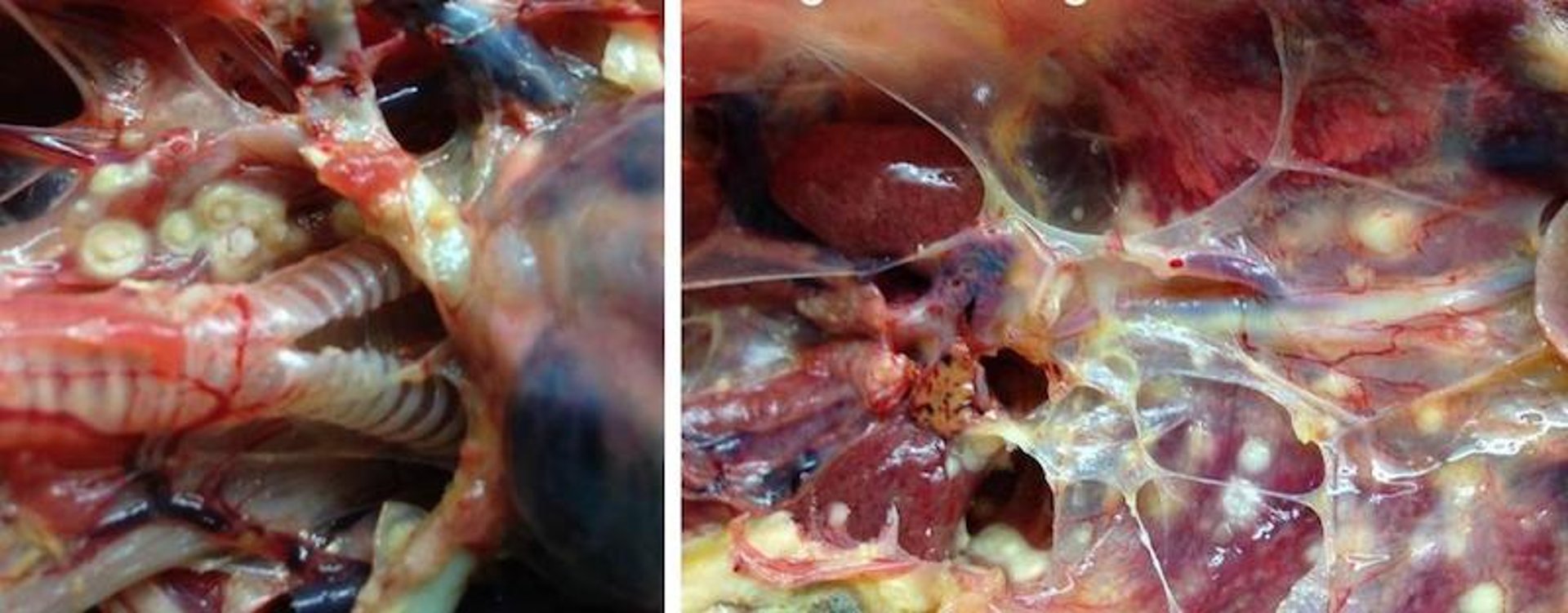
Aspergillosis granulomas throughout the air sacs and lung of a penguin.
Courtesy of Dr. Gerry Dorrestein.
Tracheitis due to aspergillosis can occur in immunocompromised birds. Aspergillus granulomas often form in the syrinx of psittacine birds and raptors and are particularly challenging to treat. Changes in vocalization may occur before dyspnea is observed, and often these birds will stretch out their necks while breathing. Lower respiratory disease, including airsacculitis, often involves invasion by Aspergillus spp. Granulomas of the air sacs or the coelomic cavity are also common, usually in the caudal thoracic or abdominal air sacs. These lesions may require surgical resection.
Diagnosis of Aspergillosis in Pet Birds
History, clinical presentation
CBC, biochemistry profile, serology, PCR assay
Imaging (radiographs, CT, endoscopy)
Cytology, histopathology, culture
Diagnosis can be challenging but should be pursued because treatment is longterm and costly. Aspergillosis should be considered in any pet bird presenting with signs of upper or lower respiratory disease, wasting disease, or marked leukocytosis/monocytosis. A leukocytosis/monocytosis combined with clinical signs and radiographic findings can provide a strong presumptive diagnosis in suspect cases. Often, birds with chronic disease will be anemic.
A radiograph may reveal airsacculitis, granulomas, or severe pulmonary disease. A CT scan or MRI is more likely to reveal more subtle or diffuse disease. Serologic testing is of limited use; antibody and antigen titers, including galactomannan antigen testing, often result in false-negative or false-positive results. A false-negative often occurs because of immunosuppression, so consultation with the laboratory regarding interpretation is important. PCR testing to detect specific Aspergillus DNA is a much more sensitive method to confirm infection and is more suitable for immunocompromised birds because detection of antibodies is not involved.
Plasma protein electrophoresis showing increased beta-globulin levels is consistent with aspergillosis. Definitive diagnosis may require direct visualization of lesions either by surgery or endoscopy and confirmation by biopsy, cytology, and/or fungal culture of lesions. Low fungal viability may yield a negative culture despite confirmation by cytologic results.
Treatment of Aspergillosis in Pet Birds
Antifungals (oral, intravenous, intranasal, nebulization)
Supportive care (oxygen, nutrition, fluids), possible air sac tube placement
Endoscopic examination and/or surgical debridement
Treatment of aspergillosis varies depending on the site of infection. An acute tracheal infection with obstruction by an aspergilloma is an emergency that may require placing an air sac tube. After tube placement, syringeal or tracheal plaques are removed with a rigid endoscope. Amphotericin B can then be instilled intratracheally at 1 mg/kg through the glottis, and treatment with systemic antifungals and nebulization should be started. Amphotericin B is the only fungicidal agent available and can be used in nebulization, as a nasal flush, intratracheally, and in IV administration. For nebulization, a concentration of 0.25–1 mg/mL of sterile water can be used. Nasal and sinus flushes are generally more dilute at 0.05 mg/mL of sterile water. Amphotericin should not be diluted with saline, because this decreases its potency.
Flushing the nares and sinus with unmedicated sterile water or saline before medicating may allow samples to be obtained for cytologic examination and culture. Several flushes of unmedicated warm isotonic saline or sterile water should be done before a final infusion of the medicated mixture. Care must be exercised to maintain the bird’s head in a downward position to avoid the potential for aspiration of the infected debris into the lower respiratory tract.
Itraconazole (5–10 mg/kg, PO, once to twice daily) is the most commonly used azole for systemic infection. African grey parrots are more sensitive to adverse effects of itraconazole, especially regurgitation and anorexia, and should be dosed at 5 mg/kg/day, PO. Terbinafine (10–15 mg/kg, PO, 2 times a day) can be used in lieu of or in conjunction with itraconazole. Clotrimazole can be used for nebulization in conjunction with systemic therapy (10 mg/mL, nebulized 15–30 minutes 2–4 times/day). Voriconazole (12–18 mg/kg, PO, 2 times a day) is used for resistant strains of Aspergillus.
If fungal granulomas are identified and the lesions are accessible, debulking endosurgically or treating the lesions topically with amphotericin B may improve the outcome. Birds undergoing treatment should be monitored closely for adverse effects of many antifungal drugs, which can include depression, anorexia, and liver dysfunction. Hepatic enzymes, bile acids, and uric acid concentrations should be monitored every 4 weeks during treatment. Treatment success may be difficult to determine, but serial CBCs and radiographs may be helpful. Treatment with oral drugs should be continued for 2–4 weeks after clinical signs have resolved. Birds with aspergillosis often have underlying disease problems and may be immunocompromised, which may affect treatment and recovery. Thickened and scarred air sacs that develop during and persist after infection can provide an ideal environment for disease recurrence.
Macrorhabdus ornithogaster Infection
(Macrorhabdosis, Megabacteria, Avian Gastric Yeast)
Macrorhabdus ornithogaster is a yeast that most often affects the proventriculus and ventriculus of smaller companion birds (eg, budgerigars, parrotlets, lovebirds, cockatiels, and finches). Previously described as a bacterium, this organism has a worldwide distribution and varies widely in pathogenicity.
Clinical Findings and Diagnosis of Macrorhabdus ornithogaster Infection of Pet Birds
Clinical evaluation
Fecal examination
Clinical signs of Macrorhabdus ornithogaster infection are weight loss, regurgitation, lethargy, passage of undigested food, and diarrhea. These clinical signs may mimic proventricular dilatation disease. Mortality may be high, but birds may recover. In birds that recover, relapses and potential shedding of the organism in the feces are likely. This disease is often seen in conjunction with immunosuppression (eg, polyomavirus and circovirus infection, or associated with poor husbandry). Asymptomatic infection is common.

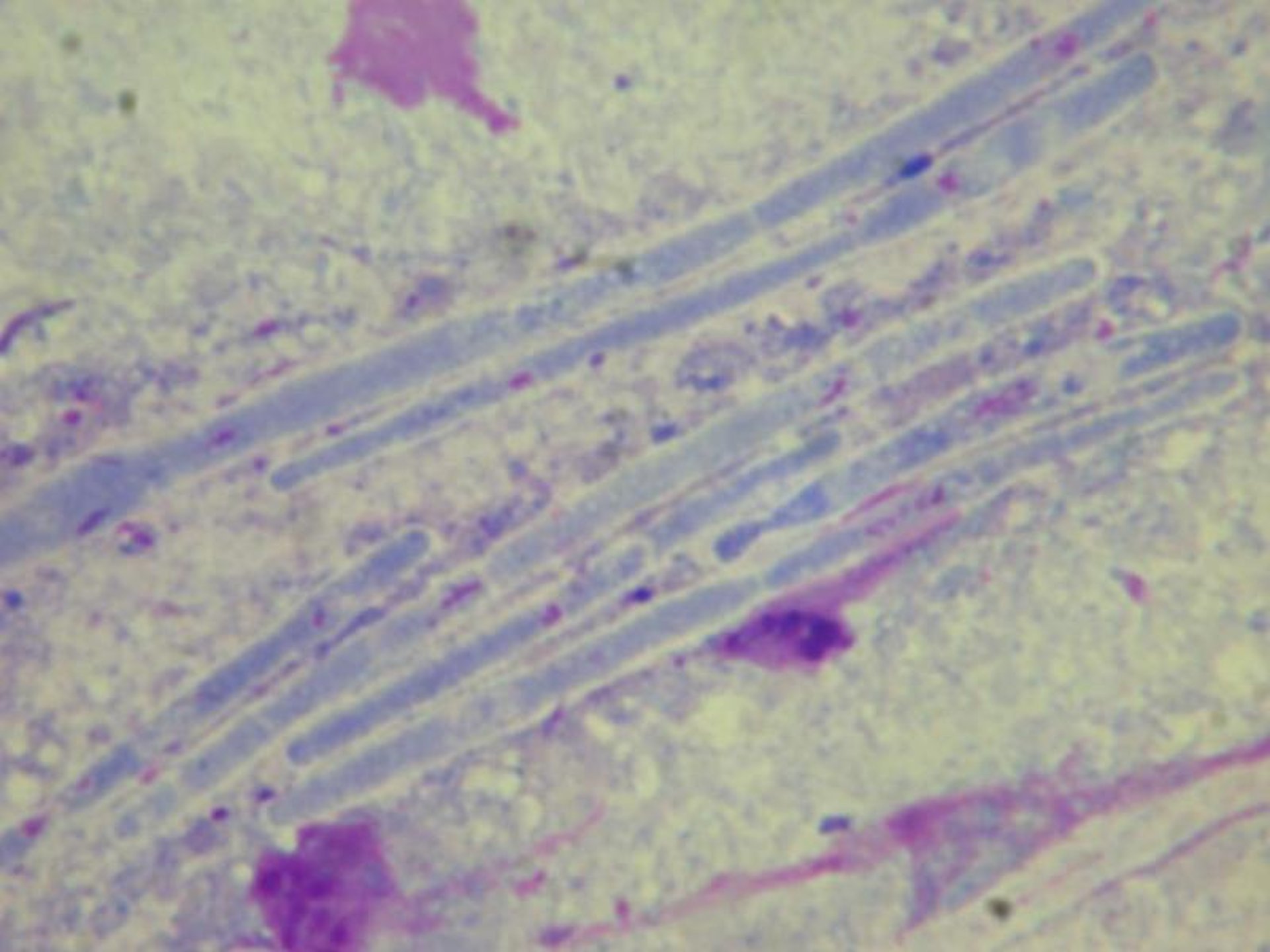
Macrorhabdus in a gouldian finch.
Courtesy of Dr. Gerry Dorrestein.
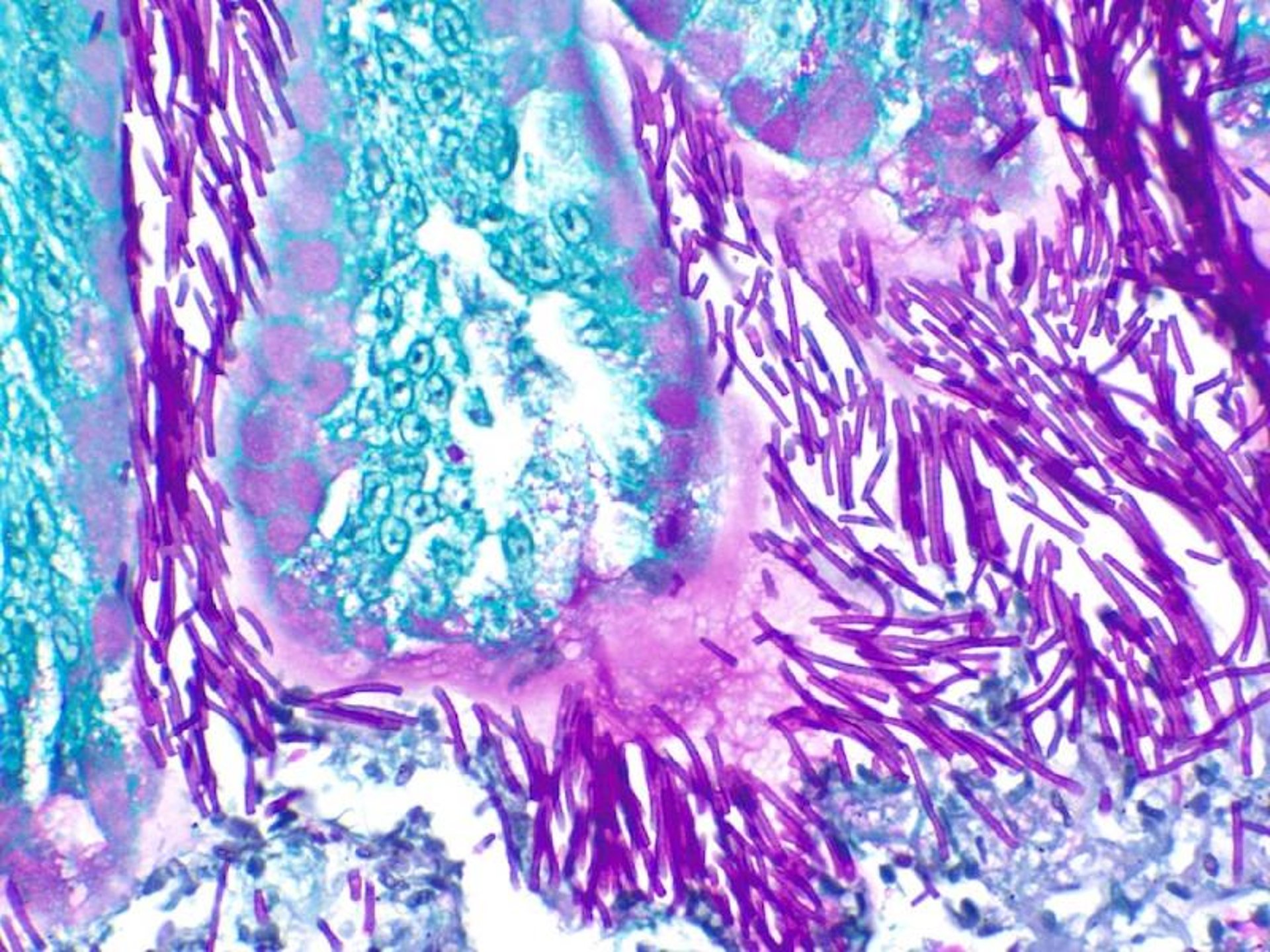
Macrorhabdus.
Courtesy of Dr. Brian Porter.
Diagnosis of Macrorhabdus ornithogaster infection is made by examining a wet mount of a fresh dropping at 10–50X magnification with the stage condenser mostly closed to increase contrast. The large, rod-shaped organisms are approximately 2–4 mcm wide and 60–90 mcm long. Many birds are asymptomatic and shed low numbers of organisms, whereas sick birds tend to shed large numbers. Birds may shed the organism intermittently, so a negative fecal examination does not exclude infection. Wet mount, modified Wright’s, or Gram stain of a fecal sample often reveal organisms.
M ornithogaster appears as a large, gram-positive rod, with mottling or stippling throughout its length. Although the size and length may vary, organisms recovered from the droppings are generally several magnitudes larger than the normal digestive bacilli found in birds. Selected veterinary laboratories offer both visual identification and PCR testing. M ornithogaster does not grow on conventional fungal media.
Radiographs may reveal a dilated proventriculus. Necropsy lesions may include thinning of the isthmus, proventricular dilation and ulceration, thickening of the proventricular wall, mucus production, and softening of the koilin layer of the ventriculus.
Treatment and Control of Macrorhabdus ornithogaster Infection of Pet Birds
Antifungal drugs
The goals of treatment of Macrorhabdus ornithogaster infection are to reduce the number of organisms and improve the general health and immunocompetence of the bird. Amphotericin (100 mg/kg, PO, 2 times a day for 30 days) has had the highest treatment success rate, but failures are common, especially with a shorter duration of treatment. Acidification of the proventriculus (apple cider vinegar, vitamin C) has been reported to create an environment less conducive to proliferation of Macrorhabdus. Voriconazole has been anecdotally reported to be successful at 10 mg/kg, PO, 2 times a day.
Treatment with sodium benzoate in the drinking water has been anecdotally reported to be successful but is still experimental. Sodium benzoate at 1 tsp/L water for 5 weeks cleared the infection in nonbreeding budgerigars, but in budgerigars that were rearing chicks in environmental temperatures >90°F (32.2°C), treatment with ½ tsp/L water resulted in neurologic signs and death of the adult budgerigars because of their increased water intake.
The current recommendation for treatment of Macrorhabdus ornithogaster infection with sodium benzoate is ½ tsp (2.5 g) of sodium benzoate powder/L of water (used as only water source and made fresh daily). If the birds are not drinking the medicated water, the dose should be decreased to ¼ tsp (1.25 g)/L of water, and slowly increased to ½ tsp over the next few days. Feces should be rechecked at 14 days; if Macrorhabdus organisms are still present, the dose should be increased over several days to 1 tsp (5 g)/L. Feces should be rechecked at 30 days. The lower dose of ¼ to ½ tsp powder/L of water should be used in birds housed outdoors in summer (temperatures >90°F [32.2°C]) and in birds feeding chicks. Gloves should be worn when handling medication.
Asymptomatic carriers are common. Artificial incubation of eggs and hand feeding nestlings can help establish a pathogen-free flock.
Miscellaneous Mycoses
Malassezia spp have been reported in birds with feather picking and dermatologic conditions. Rodotorula mucilaginosis is a yeast occasionally seen in skin infection in raptors (falcons). It causes yellowish-brown crusty areas of the skin in the axillary or inguinal areas. Cryptococcosis is worldwide in occurrence and caused by a saprophytic fungus, Cryptococcus neoformans. This fungus is uncommon in avian species, but it has been isolated from the fecal droppings of wild birds, particularly pigeons, and from feces of canaries and psittacine birds. C neoformans infection has been reported in Columbiformes, a Moluccan cockatoo, a Thick-billed parrot, a Green-wing macaw, and an African grey parrot. Dermatophytosis, including Trichophyton and Microsporum spp, is occasionally reported in pet birds. Treatment protocols for dogs and cats are used. Histoplasmosis and mucormycosis are also occasionally reported in pet birds.
For More Information
Also see pet health content regarding disorders and diseases of pet birds.





