



Pasteurellosis
Pasteurellosis is common in domestic rabbits. The etiologic agent is Pasteurella multocida, a gram-negative, nonmotile coccobacillus. Rabbits will usually become infected with P multocida immediately after birth, and the prevalence of colonization increases with age until about 5 months. Most adult rabbits are believed to be infected with P multocida. It is highly contagious and transmitted primarily by direct contact, although aerosol transmission may also occur.
In conventional colonies, 30%–90% of apparently healthy rabbits may be asymptomatic carriers. This is important to consider when nasal cultures are collected, because not every positive result indicates a pathologic condition.
This bacteria is not specific to rabbits but affects other animals as well, including dogs, cats, poultry, and domestic livestock. In case of a sudden Pasteurella outbreak, immediate medical attention is required for containment of the disease. The investigation of the case should include factors that could have contributed to the problem and any aspects that could be causing stress and immune suppression in the affected rabbits. To get a true representative culture of the nasal bacterial fauna, the rabbit needs to be heavily sedated or anesthetized and a deep nasal culture obtained by introducing the swab relatively far into the nasal opening. Several barrier colonies of laboratory rabbits have been established as Pasteurella-free.
Clinical Findings of Pasteurellosis in Rabbits
Pasteurellosis presents with a variety of clinical symptoms, including rhinitis, pneumonia, abscesses, reproductive tract infections, torticollis, otitis media/interna and septicemia. Rabbits may develop Pasteurella septicemia and die acutely without any clinical signs. Necropsy findings of septicemia cases may reveal only congestion and petechial hemorrhages in multiple organs.
Rhinitis (snuffles or nasal catarrh) is an acute, subacute, or chronic inflammation of the mucous membranes of the air passages and lungs, induced primarily by Pasteurella, but Pseudomonas spp, Bordetella bronchiseptica, Staphylococcus spp, and Streptococcus have also been isolated. The initial sign is a thin, serous exudate from the nose and eyes that later becomes purulent. The fur on the inside of the front legs just above the paws may be matted and caked with dried exudate, or this area may be clean with thinned fur as a result of pawing at the nose. Infected rabbits usually sneeze and cough. In general, snuffles occurs when the resistance of the rabbit is low. Recovered rabbits are likely carriers. Pneumonia can ensue.
Pneumonia is common in domestic rabbits. Frequently, it is a secondary and complicating factor in the enteritis complex. The cause is typically P multocida, but other bacteria such as Klebsiella pneumoniae, Bordetella bronchiseptica, Staphylococcus aureus, and pneumococci may be involved. Upper respiratory disease (snuffles, see above) is often a precursor of pneumonia. Inadequate ventilation, sanitation, and nesting material are predisposing factors. The number of cases of pneumonia is directly proportional to the level of ammonia in the cage, hutch, or rabbitry. Ventilation is of utmost importance to provide good air quality. Affected rabbits are anorectic, listless, dyspneic, and might have a fever. Treatment should include systemic antibiotics, optimally based on a culture and sensitivity, because of possible resistance to common pathogens. The rabbits are usually dehydrated, and supportive care with hydration and syringe feeding is often necessary as well. Topically administered ophthalmologic antibiotic products instilled into the nostril can also be beneficial. Necropsy reveals bronchopneumonia, pleuritis, pyothorax, or pericardial petechiae. Because rabbits commonly harbor Bordetella bronchiseptica in their upper respiratory tract, rabbits and guinea pigs should not be housed together, because guinea pigs are very susceptible to a severe pneumonia caused by Bordetella.
Otitis media or interna (“wry neck” or head tilt) results from infections with various agents. P multocida was reported to be isolated from 97% of cases of otitis media, including clinical and subclinical cases. B bronchiseptica and staphylococci were also found in 5%–10% of cases. An accumulation of pus or fluid in the middle or inner ear causes the rabbit to twist its head, eg, “wry neck” or torticollis. However, not all rabbits with middle ear infections show torticollis. Longterm antibiotic treatment is required for drug penetration into the affected area. Antibiotic therapy may only prevent worsening of clinical signs, and the prognosis is guarded with medical therapy alone. A bulla osteotomy is often indicated when medical management of otitis media and interna fails. A total ear canal ablation in rabbits is not recommended because the pathophysiology of otitis in rabbits is very different from that in dogs, in which a total ear canal ablation is often performed. If drainage of the cerumen is required, a simple stoma surgery at the base of the ear canal will be enough to facilitate the opening of the ear canal. Proper imaging of the ear lesions is indicated before surgery. Often, a CT scan of the head will help to identify the lesion and potentially help to differentiate otitis media/interna from intracranial disease in cases of torticollis (eg, Encephalitozoon cuniculi infection).

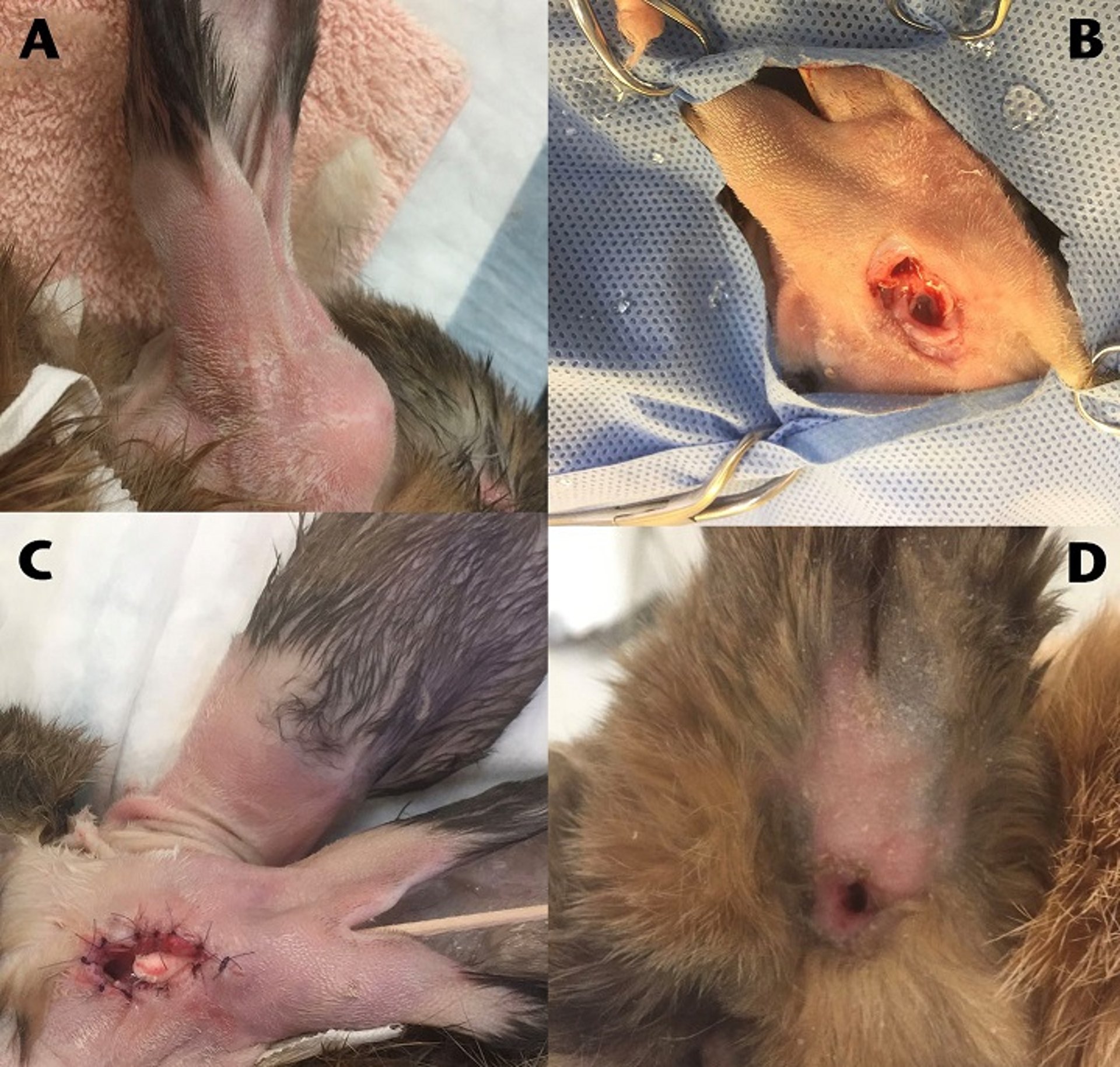
This series depicts a novel surgery for otitis externa. A) Ear base swelling is a common presentation for otitis externa. However, this is not due to the hyperplasia of the cerumen-producing glands; it is purely a problem of mechanical clearing of the cerumen from the ear canal. B) A stoma to the outer ear canal is created at the base to facilitate drainage of cerumen. Access to the inner ear is possible if a bulla osteotomy is needed. C) The opening is marsupialized to avoid closure. Here, a cotton swab is passed through the outer ear canal. D) The stoma a few weeks after surgery, perfectly healed and providing adequate drainage.
Courtesy of Dr. Joerg Mayer.
Conjunctivitis and dacryocystitis (weepy eye) is a common problem in rabbits. Predisposing factors include mechanical irritation, eyelid diseases, and dental disease. Conjunctivitis in rabbits may be associated with other disease processes, especially dacryocystitis. The most incriminated cause of conjunctivitis is P multocida; however, this may be only a secondary infection. Primary infections are less common than opportunistic infections. Transmission is by direct contact or fomites. Affected rabbits rub their eyes with their front feet. Bacterial conjunctivitis can be treated with topical chloramphenicol, ciprofloxacin, or gentamicin combined with systemic broad-spectrum antibiotic therapy if topical treatment alone is ineffective.
Dacryocystitis and acquired nasal duct obstruction may arise from chronic rhinitis that travels up the nasolacrimal duct to the eye or occasionally from dental disease such as tooth root inflammation or abscessation. Dacryocystorhinography or injection of contrast material into the lacrimal punctum will provide good radiographic detail of the duct throughout its course and show the site of obstruction. In long-standing cases of dacryocystitis and conjunctivitis, the punctum and segments of the nasolacrimal duct may progressively narrow and be replaced with scar tissue until they are irreversibly obstructed. To relieve discomfort and inflammation associated with these conditions, the use of topical nonsteroidal anti-inflammatory ophthalmic preparations such as flurbiprofen can be considered. Systemic NSAIDs such as meloxicam should also be used. Treatment can include gentle saline flushing of the duct through the nasolacrimal punctum, but care is warranted to not damage the nasolacrimal duct during flushing. Any mechanical damage to the fragile tear duct can result in permanent epiphora, and owners should be advised accordingly.
Conjunctivitis also accompanies rabbitpox and myxomatosis.
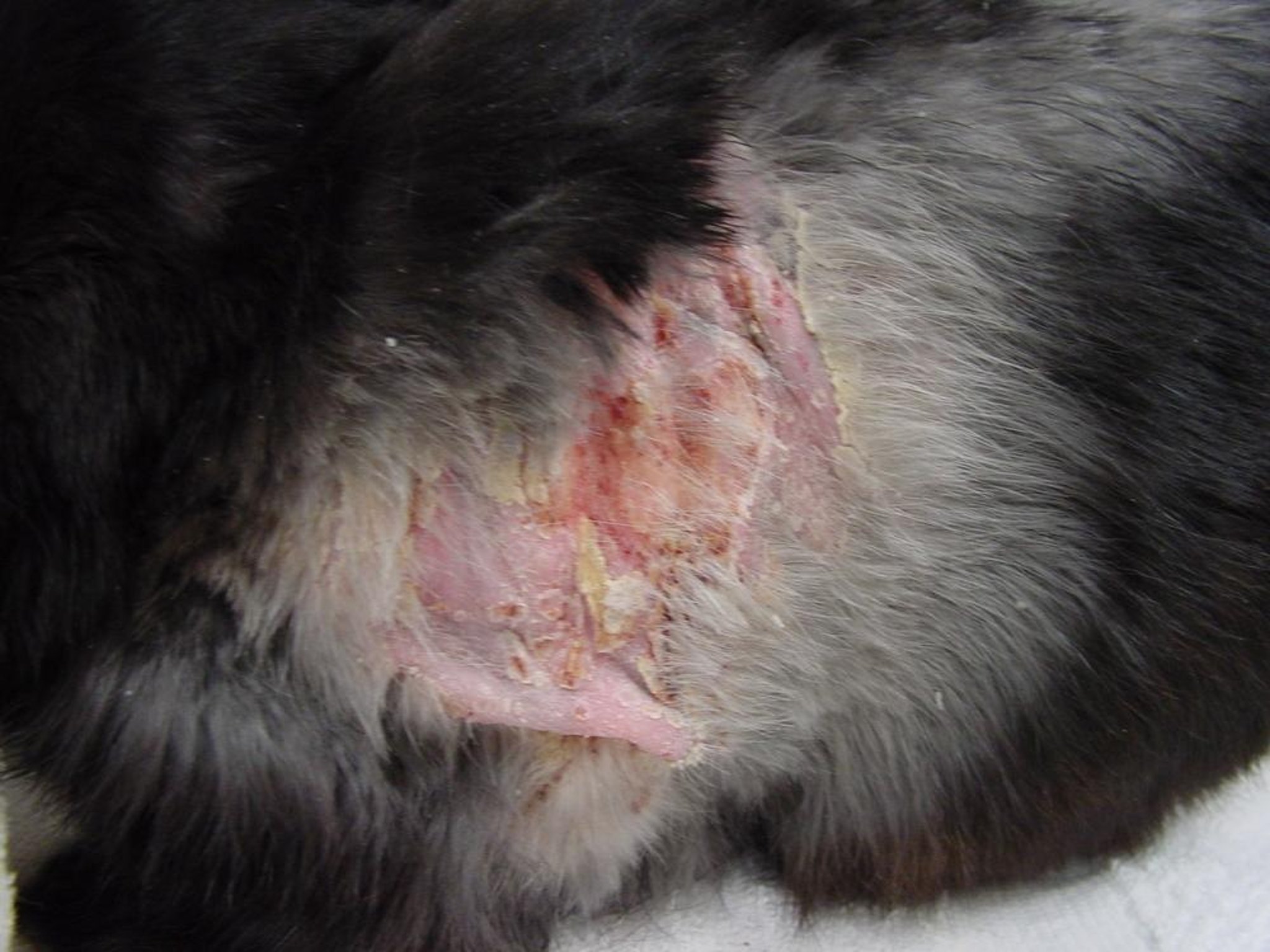
Subcutaneous and visceral abscesses caused by P multocida may be clinically silent for long periods and spontaneously rupture. When bucks penned together fight, their wounds frequently develop abscesses. Abscesses in rabbits are treated differently than abscesses in cats; rupture or drainage via Penrose is not the recommended course. Thick-walled abscesses should be surgically excised en bloc if possible. Open wounds should be debrided or curetted, marsupialized, and left to heal by second intention. Facial abscesses are often related to dental disease. Drainage of the abscess accompanied by systemic antibiotic therapy based on culture and sensitivity tests has been successful, although recurrence can be common.


Note the thick appearance of the purulent material in the open wound. Use of a drain is contraindicated in these cases because the pus is too thick to drain, and the material needs to be surgically removed.
Courtesy of Dr. Joerg Mayer.
Pasteurella can cause genital infections, but several other organisms also may be involved. The spirochete Treponema paraluiscuniculi is the causative agent of rabbit syphilis. Genital infections are manifest by an acute or subacute inflammation of the reproductive tract and most frequently are found in adults, more often in does than bucks. In the case of Treponema, a severe conjunctivitis or dermatosis between the toes can also be a key clinical sign. If both horns of the uterus are affected, the does often become sterile; if only one horn is involved, a normal litter may develop in the other. The only sign of pyometra may be a thick, yellowish gray vaginal discharge. If bloody discharge from the vulva is observed and a large uterine horn can be palpated, uterine adenocarcinoma should be included in the differential diagnosis. Bucks may discharge pus from the urethra or have an enlarged testicle. Chronic infection of the prostate and seminal vesicles is likely, and because venereal transmission may ensue, it is best to cull the animal in a production colony. Surgical removal of the infected reproductive organs in conjunction with antibiotic therapy is indicated for pet rabbits. The contaminated caging and its equipment should be thoroughly disinfected.


This severe case of blepharitis was caused by Treponema paraluis-cuniculi. Note the round area where the lesion has been biopsied, because this is the preferred way to diagnose the condition.
Courtesy of Dr. Joerg Mayer.
Diagnosis of Pasteurellosis in Rabbits
Combination of clinical signs, bacterial culture, and serotyping
A diagnosis of pasteurellosis should not be made solely on the presenting signs, but should include bacterial culture and blood work (CBC and blood chemistry profile). In severely affected cases, more advanced diagnostic tests such as radiography, ultrasonography, or a CT scan may also be needed.
Carriers of P multocida can be identified by an indirect fluorescent antibody test on nasal swabs. A technique that uses small, saline-moistened, pediatric nasopharyngeal swabs has proved superior to the standard, larger nasal swab. The swab is directed medially through the external nares past the turbinates and onto the dorsal surface of the soft palate; sedation is recommended. The swab is then retracted and can be used in the fluorescent antibody test or plated onto a culture medium. An ELISA test to detect antibodies against P multocida may also help detect carriers.
PCR can discriminate between different isolates and is commercially available. It is important to remember that Pasteurella can be sampled from a large percentage of clinically normal rabbits, and culture results must be interpreted carefully and in combination with the clinical signs and the antibiogram from sensitivity testing. Not every strain of Pasteurella is pathogenic. Five serotypes (strains) of Pasteurella have been described, with two of them most commonly involved in pathologic conditions in rabbits. The serotype, identified during a culture and sensitivity test, is tested to determine the most effective antibiotic.
Treatment and Control of Pasteurellosis in Rabbits
Antimicrobial treatment may help control signs but will likely not eliminate infection
Treatment is difficult and will most likely not eradicate the organism. Antibiotics seem to provide only temporary remission, and the next stress (eg, kindling) may cause relapse. Prolonged treatment for 6–8 weeks is often needed. Many of the newer antibiotics are already ineffective because of an increase in resistant strains. Before treatment, a culture and sensitivity should be done to determine the best antibiotic to use.
Antibiotics effective against Pasteurella include enrofloxacin, trimethoprim sulfa, chloramphenicol, penicillin G, and azithromycin. Very often, systemic antibiotic therapy can be augmented by local antibiotic therapy. Gentamicin ophthalmologic drugs instilled into the nostrils can supplement systemic antibiotics for treatment of upper respiratory tract infections. Fluoroquinolones are usually good drugs if no resistance has built up, which is unfortunately common. Oral medication is usually well tolerated and without adverse effects. In case of unsatisfactory results, doxycycline can be added, because both drugs appear to have a synergistic effect. Sometimes, amikacin or azithromycin must be used, based on culture results.
Although medication in the drinking water is not recommended because of the tainting of the flavor and potential underdosing, this is sometimes the only possible route to treat animals on a larger scale. Enrofloxacin (200 mg/L of drinking water for 30 days) can be effective for upper respiratory P multocida infections. Procaine penicillin (60,000 IU/kg/day, SC, for 10–14 days) is also recommended for individual rabbits, but caution is warranted, because deaths from enterotoxemia can follow if the drug is accidentally given orally.
Additional treatments may include anti-inflammatory drugs, careful flushing of the nasolacrimal duct, nebulization therapy, ear and eye drops, administration of fluids, and surgery.

A culture from any discharge or purulent material should always be taken before starting a rabbit on antimicrobials. When possible, an aerobic and anaerobic culture should be taken. Many abscesses in rabbits are due to anaerobic bacteria.
Courtesy of Dr. Joerg Mayer.
Two methods to free a production colony of Pasteurella have been reported. The first involves culture and culling of positive animals; once the colony is Pasteurella-free, it must be maintained in isolation. In the second method, pregnant does past kindling are treated with enrofloxacin. While does remain Pasteurella-culture positive, the kits remain Pasteurella-culture negative. Carriers can be identified by an indirect fluorescent antibody test on nasal swabs.
Key Points
Pasteurella multocida infects most rabbits, but many animals are asymptomatic carriers.
Diagnosis is based on clinical signs and bacterial culture.
Antibiotics can control signs but are unlikely to eliminate infection.
Listeriosis
Listeriosis, a sporadic septicemic disease characterized by sudden deaths or abortions, is most common in does in advanced pregnancy. Poor husbandry and stress may be important in initiating the disease. Clinical signs are variable and nonspecific and include anorexia, depression, and weight loss. In contrast to the disease in cattle and sheep, listeriosis seldom affects the CNS in rabbits. The causal agent, Listeria monocytogenes, spreads via the blood to the liver, spleen, and gravid uterus. At necropsy, the liver consistently contains multiple, pinpoint, gray-white foci. Because diagnosis is rarely made pre-mortem, treatment is seldom attempted. L monocytogenes can infect many animals, including people. It is difficult to isolate with normal methods, and special techniques are often required. This problem is more common in commercial operations than in pet rabbits.
Intestinal Diseases
Intestinal disease is a major cause of death in young rabbits. Although most diarrheal diseases were once lumped together (as the enteritis complex) or simply called mucoid enteritis, specific diseases are being delineated. Diet, antibiotic treatment, and other factors create disturbances of the GI microflora and may predispose rabbits to dysbiosis and intestinal disease. Also see a discussion of GI stasis due to hairballs.
Enterotoxemia in Rabbits
Enterotoxemia is a severe diarrheal disease, primarily of rabbits 4–8 weeks old when naturally infected; it also can affect rabbits at all life stages if an inappropriate antibiotic is given orally. Signs are lethargy, rough coat, greenish brown fecal material covering the perineal area, and death within 48 hours. Often, a rabbit looks healthy in the evening and is dead the next morning. Necropsy reveals the typical lesions of enterotoxemia, ie, a fluid-distended intestine with hemorrhagic petechiae on the serosal surface. The primary causative agent is Clostridium spiroforme, which produces an iota toxin. Little is known about transmission of the organism; it is assumed to be a commensal normally present in low numbers. The type of diet seems to be a factor in development of the disease; enterotoxemia is seen less often when high-fiber diets are fed. Because most beta-lactams, lincomycin, clindamycin, and erythromycin induce Clostridium-related (eg, Clostridium difficile) enterotoxemia because of their selective effect on normal, gram-positive bacteria, their oral use is contraindicated in rabbits. Enterotoxemia is a consideration for these antibiotic therapies.
These diarrheas are remarkably similar to those that occur naturally (described above as enterotoxemia). Treatment of colony rabbits is seldom attempted because of the rapidity of death. However, when population size permits, cholestyramine has been used with promising results, both as a preventive and a treatment. Reducing stress of the young rabbits (weaning, etc) and ad lib feeding of hay or straw are helpful in prevention. Adding 250 ppm of copper sulfate to the diet of young rabbits also helps prevent enterotoxemia. Individual animal treatment for enterotoxemia should include aggressive fluid therapy and intensive supportive care. Monitoring of hydration status, body temperature, and heart rates is extremely important. There is little evidence that antibiotics are helpful. Prognosis for advanced cases is often poor.
Diagnosis of enterotoxemia depends on history, signs, lesions, and demonstration of C spiroforme. A stained fecal smear can be examined to look for the clostridial organisms. Very often, the Clostridium contains a spore that gives it the appearance of a safety pin. Centrifugation of intestinal contents at 20,000 g for 15 minutes followed by culture of the supernatant-pellet interface will reveal the organism. For a definitive diagnosis, the presence of iota toxin in the supernatant of centrifuged cecal contents can be demonstrated by in vivo or in vitro assays.

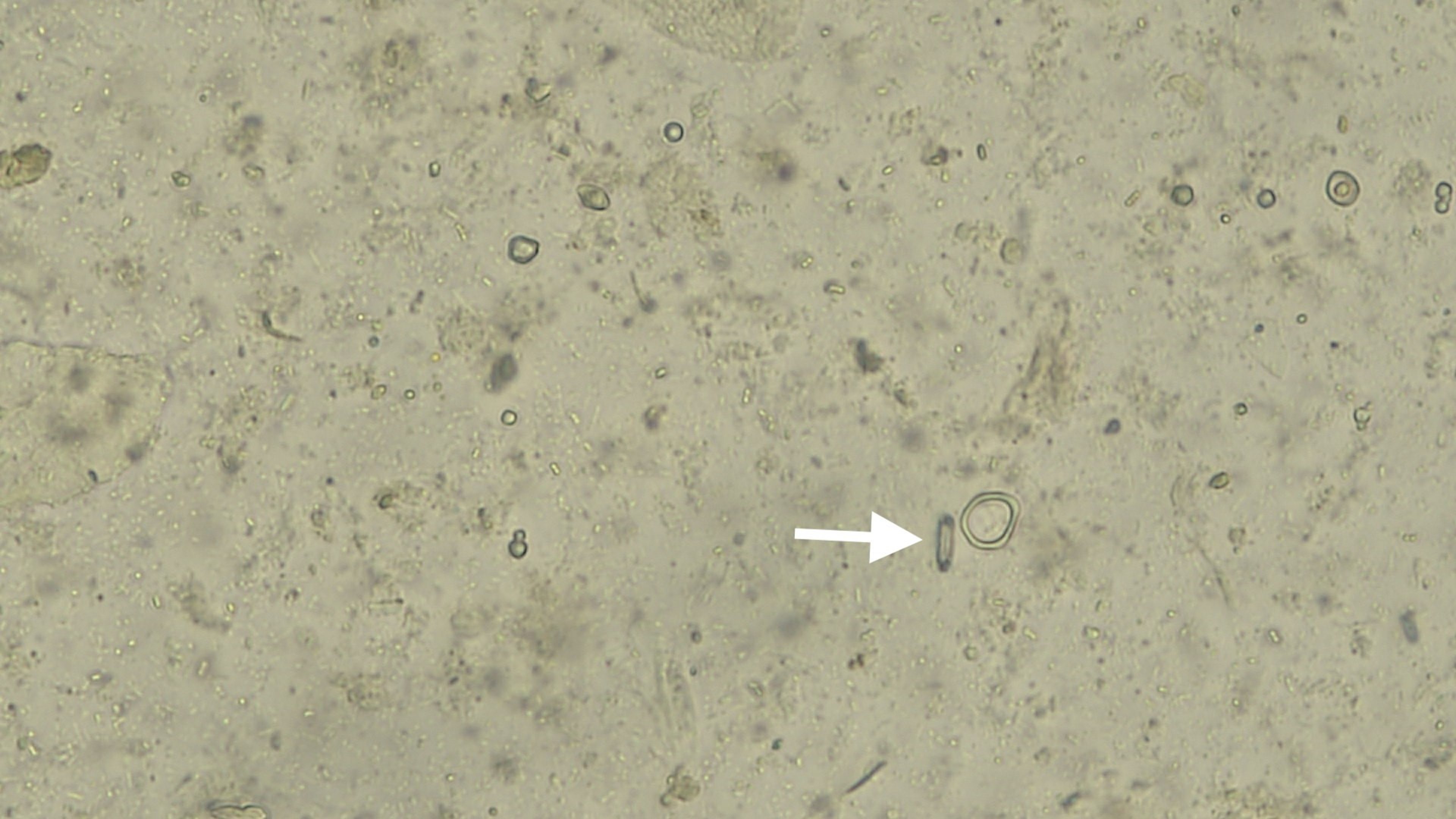
Note the clostridial cell in the unstained, fresh fecal smear (white arrow). The bacteria contains a spore that gives it a typical safety pin appearance.
Courtesy of Dr. Joerg Mayer.
Tyzzer Disease in Rabbits

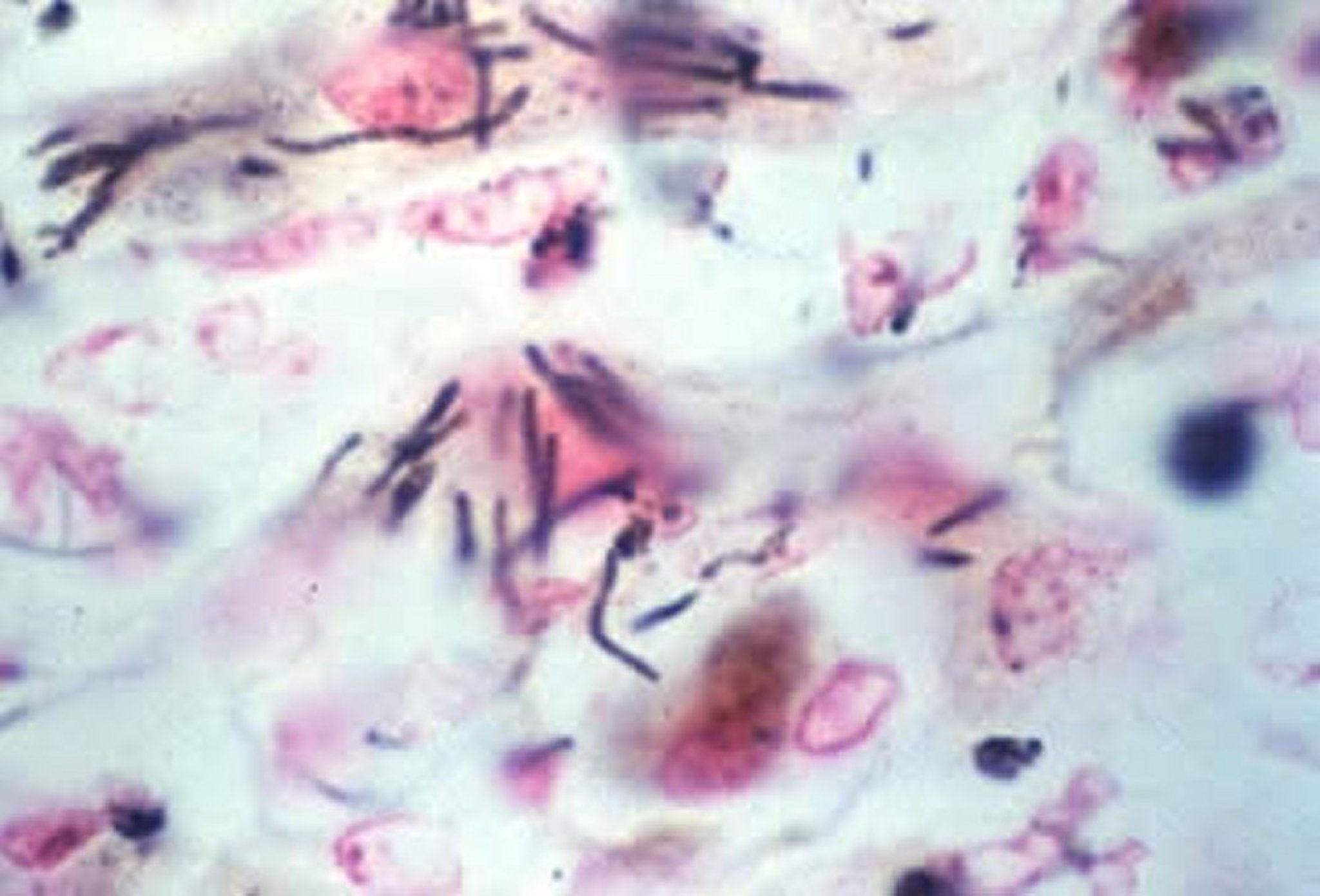
Clostridium piliforme, rabbit, silver stain, high power. Note the characteristic bundling of the black, silver-stained rods in this liver section.
Courtesy of Dr. John Prescott.
Tyzzer disease, caused by Clostridium piliforme, is characterized by profuse watery diarrhea, anorexia, dehydration, lethargy, staining of the hindquarters, and death within 1–3 days in weanling rabbits 6–12 weeks old. Acute outbreaks have been associated with >90% mortality. Some rabbits may develop chronic infections that present clinically as a wasting disease. Infection occurs by ingestion and is associated with poor sanitation and stress. The lesions consist of necrotic enteritis along with multifocal necrosis in the liver and heart. Necrotic patches on the serosal surface of the cecum are typical lesions for this disease. Diagnosis is made histologically; special stains (eg, Giemsa or Warthin-Starry silver) show the characteristic intracellular bacterium. Culturing is impractical, because the bacterium does not grow on artificial media. Serologic tests are available from animal diagnostic laboratories. Tyzzer disease affects a wide spectrum of other species but has not been reported in people, although titers have been documented in pregnant women. Although antibiotics used in treatment of other animals have not been effective in rabbits, oxytetracycline has been of some value in limiting an outbreak. No vaccine is available. Aggressive disinfection and decontamination of the housing facility to reduce the presence of hardy spores is indicated with either 1% peracetic acid or 3% hypochlorite.
Colibacillosis in Rabbits
Escherichia coli as a cause of rabbit diarrhea has been confused by the circumstance that E coli often proliferate when rabbits develop diarrhea for any reason. Enteropathogenic strains of E coli (serotype O103) commonly express the eae gene, which codes for intimin, an outer membrane protein associated with the attaching and effacing lesions. Serotypes O15:H, O109:H2, O103:H2, O128, and O132 are also important. Healthy rabbits do not have E coli of any strain associated with their GI tract.
Two types of colibacillosis are seen in rabbits, depending on age. Rabbits 1–2 weeks old develop a severe yellowish diarrhea that results in high mortality. It is common for entire litters to succumb to this disease. In weaned rabbits 4–6 weeks old, a diarrheal disease very similar to that described for enterotoxemia is seen. The intestines are fluid filled, with petechial hemorrhages on the serosal surface, similar to the pathology described for both Tyzzer disease and enterotoxemia. Death occurs in 5–14 days, or rabbits are left stunted and unthrifty. Diagnosis is made by isolating E coli on blood agar and then having the isolate biotyped or serotyped. Electron micrographs of E coli attached to the mucosa are also helpful. In severe cases, treatment is not successful; in mild cases, antibiotics may be effective. Severely affected rabbits should be culled, and facilities thoroughly sanitized. High-fiber diets appear to help prevent the disease in weaned rabbits.
Proliferative Enteropathy in Rabbits
Proliferative enteropathy caused by Lawsonia intracellularis has been reported to cause diarrhea in weanling rabbits. Clinical signs include diarrhea, depression, and dehydration, which resolve over 1–2 weeks. Disease does not cause death unless associated with a dual infection with another enteropathogenic agent. Diagnosis is based on necropsy findings of a thickened and corrugated ileum and histologic identification of the rod-shaped to curved or spiral silver-staining organism in crypt enterocytes. The organism requires cell-containing media (enterocytes) for culture. Immunohistochemistry and PCR may be useful to identify L intracellularis. Isolation of sick animals and symptomatic treatment is advised. Chloramphenicol or florfenicol is the treatment of choice, but some rabbits appear sensitive to these antibiotics when given orally, so careful GI monitoring is required.
Mucoid Enteropathy in Rabbits
Mucoid enteropathy is a distinct diarrheal disease of rabbits, characterized by minimal inflammation, hypersecretion, and accumulation of mucus in the small and large intestines. The cause is unknown, and it may occur concurrent with other enteric diseases. Predisposing factors include dietary changes, a low indigestible fiber diet (dietary fiber < 6%) , antibiotic treatments, environmental stress, and challenges with other bacteria. Clinical signs are gelatinous or mucus-covered feces, anorexia, lethargy, subnormal temperature, dehydration, rough coat, and often a bloated abdomen due to excess water in the stomach. A firm, impacted cecum may be palpable. The perineal area is often covered with mucus and feces. Diagnosis is based on clinical signs and necropsy findings of gelatinous mucus in the colon. Rabbits may live for ~1 week. Treatment is difficult and often unrewarding in severe cases, but intense fluid therapy, antibiotics, and analgesics should be tried. Prevention is the same as for any rabbit enteropathy by focusing on an adequate, fiber-rich diet.
Mastitis
(Blue Breasts)
Mastitis is common in commercial rabbitries and is occasionally seen in smaller units but rarely in pet rabbits. Poor sanitation enhances spread throughout the rabbitry. Mastitis affects lactating does and may progress to a septicemia that rapidly kills the doe. Generally, it is caused by staphylococci, but streptococci and other bacteria have been isolated. Initially, the mammary glands become hot, reddened, and swollen. Later, they may become cyanotic, hence the common name, “blue breast.” The doe will not eat but may crave water. Fever ≥105°F (40.5°C) is often noted. If antibiotic treatment is started early (the first day the doe goes off feed), the rabbit may be saved and damage limited to one or two mammary glands. If more than two glands are lost, keeping the doe may not be economical. Because penicillin often causes diarrhea in rabbits, does should be treated only after the pelleted ration has been replaced with hay or some other high-fiber diet ( see Enterotoxemia). Kits should not be fostered to another doe, because they will spread the infection to the foster mother. Hand-rearing of infected young may be attempted but is difficult. The incidence of mastitis can be reduced if nest boxes are maintained without rough edges to the entrance, which can traumatize the teats when the doe jumps in and out of the nest box. It is essential for the nest box to be sanitized before and after use. Vaccines have not proved to be beneficial to prevent mastitis.
Treponematosis
(Vent Disease, Syphilis, Spirochetosis)
Treponematosis, a specific venereal disease of domestic rabbits, is caused by the spirochete Treponema paraluiscuniculi. It is seen in both sexes and is transmitted by breeding and from the doe to offspring. Although closely related to the organism that causes human syphilis (T pallidum), T paraluiscuniculi is not transmissible to other domestic animals or people. The incubation period is 3–6 weeks. Small vesicles or ulcers are formed, which ultimately become covered with a heavy scab. These lesions usually are confined to the genital region, but the lips and eyelids may be involved. Infected rabbits should not be bred. Diagnosis is based on the lesions and observation of the spirochete’s corkscrew motility under darkfield microscopy. Serologic tests used to diagnose T pallidum, such as the VDRL slide test and the rapid-plasma regain card test, are widely available and can be used to diagnose T paraluiscuniculi. Hutch burn is a differential diagnosis.


Note the cutaneous lesions typical of Treponema paraluiscuniculi infection at the genital area and around the nostrils. The scabs are usually dry, and no discharge is noted.
Courtesy of Dr. Joerg Mayer.
Benzathine penicillin G, 42,000 IU/kg, SC, at weekly intervals for 3 weeks, is necessary to eradicate treponematosis from a herd. Procaine penicillin (60,000 IU/kg/day, SC, for 7 days) is also recommended for individual rabbits. All rabbits must be treated even if no lesions are present. Lesions usually heal within 10–14 days, and recovered rabbits can be bred without danger of transmitting the infection.
Dermatophytosis
(Ringworm)

Ringworm in rabbits is a zoonotic disease, and owners should be informed. Often, topical and systemic medication is needed to successfully cure the condition.
Courtesy of Dr. Joerg Mayer.
Clinical dermatophytosis commonly affects individual rabbits, but epizootics can also occur. Ringworm is generally associated with poor husbandry, poor nutrition, and other environmental stressors. The cause is most commonly Trichophyton mentagrophytes and occasionally Microsporum canis. Transmission is by direct contact. Fomites, such as hair brushes, that evade proper disinfection can play a significant role in spreading infection. Asymptomatic carriers are very common. The lesions usually appear first on the head and may spread to any area of the skin. Affected areas are circular, raised, reddened, and capped with white, bran-like, flaky material. A negative result with a Wood’s lamp illumination does not exclude dermatophytosis, because all agents do not fluoresce. Hair plucked from the edge of the lesion may be cultured on special media, such as dermatophyte test media or Sabouraud’s agar. A KOH skin scraping taken from the periphery of the lesion that reveals fungal forms confirms the diagnosis.
Because rabbits with active infections are infectious for people and other animals, they should be either isolated and treated or euthanized. Griseofulvin at an individual dosage of 25 mg/kg body wt/day, PO, for 4 weeks, or in the feed at 825 mg/kg of feed, is effective but not approved for use in rabbits; it should not be used in rabbits intended for human consumption. Griseofulvin may be teratogenic and should not be used in pregnant does. Extra-label treatment with oral itraconazole (5 mg/kg/day, PO, for 4–6 weeks) or topical clotrimazole or miconazole may be effective. For rabbitries, treatment with either 1% copper sulfate as a dip or 8 oz of MECA (metabolized chlorous acid/chlorine dioxide compound, 1:1:10 mix of base:activator:water) sprayed on six times in a 26-day period was shown to be effective.
Tularemia
Tularemia is rare in domestic rabbits, but wild rabbits and rodents are highly susceptible and have been involved in most epizootics. Up to 90% of human cases of tularemia are linked to wild lagomorph exposure. The etiologic agent, Francisella tularensis, is an aerobic nonmotile, gram-negative, pleomorphic, bipolar coccobacillus prevalent in the south central USA. It is highly infectious and passed through the skin, through the respiratory tract via aerosols, by ingestion, and via bloodsucking arthropods. Tularemia causes an acute fatal septicemia. Diagnosis is based on necropsy findings of septicemic bacterial disease with numerous small, bright-white hepatic foci, congestion, and enlargement of the liver and spleen. Treatment of the animal is not indicated. Tularemia is a reportable disease.





