



Newcastle disease is a severe, systemic, and fatal viral disease of poultry due to virulent strains of avian paramyxovirus type 1. Clinical signs in unvaccinated birds include sudden death, lethargy, and respiratory distress. Diagnosis is based on laboratory confirmation. Vaccines prevent clinical signs but not infection, and the control of the disease is challenging in enzootic regions.
Newcastle disease (ND) is an infection of domestic poultry and other bird species with virulent Newcastle disease virus (NDV). Newcastle disease is not a food safety or public health concern. Virulent NDV is capable of producing a devastating disease in domestic fowl, with vast social and economic consequences. It is a worldwide problem that presents primarily as an acute respiratory disease; however, depression, nervous signs, or diarrhea may be the predominant clinical form.
Severity of ND depends on the virulence and genetic type of the infecting virus and host susceptibility. There is no treatment for Newcastle disease, and, in many countries, infected and susceptible birds in the vicinity of an outbreak are culled to contain transmission of the disease.
Prevention is accomplished through vaccination and strict biosecurity. Real-time RT-PCR is the test of choice to detect viral RNA typical of virulent NDV and confirm infection in birds with clinical signs of disease. Occurrence of the disease in poultry is notifiable and may result in trade restrictions.
Etiology and Pathogenesis of Newcastle Disease in Poultry
Newcastle disease virus, synonymous with avian paramyxovirus type 1 (APMV-1), is an RNA virus and the most important of the 22 known APMV serotypes as a pathogen for poultry.
The original classification of NDV isolates into one of three pathotype groups based on their pathogenicity in chickens as virulent (velogenic), moderately virulent (mesogenic), or of low virulence (lentogenic) has been abbreviated for regulatory purposes. Velogens and mesogens are now classified as virulent NDVs (vNDVs), the cause of Newcastle disease and reportable infection; infections with lentogens, the NDVs of low virulence (loNDVs) widely used as live vaccines, are not reportable.
Severity of infection depends on:
virus virulence
virus tropism
age, immune status, and susceptibility of host species
External factors such as stress, environmental temperature, and season have a lesser impact on disease course.
Chickens are the most susceptible and waterfowl the least susceptible of domestic poultry; however, some differences may be observed if the NDV strain is adapted to a particular species. The virus infects susceptible birds through the respiratory or digestive tract when they inhale contaminated dust or aerosolized virus or ingest contaminated materials.
In field outbreaks the incubation period varies from 4 to 6 days; however, clinical signs may appear as early as 2 days and as late as 15 days postinfection.
Epidemiology of Newcastle Disease in Poultry
Virulent Newcastle disease strains are endemic in poultry in most of Asia, Africa, Mexico and some countries of South America. Other countries, including the US and Canada, are free of those strains in poultry and maintain that status with import restrictions, active surveillance and monitoring, and culling infected poultry and susceptible birds within infected premises/zones.
Cormorants, pigeons, and imported psittacine species can be infected with vNDV and occasionally have also been sources of vNDV infections in poultry. Newcastle disease virus strains of low virulence are prevalent in free-living wild birds, live bird markets, and poultry, especially waterfowl.
Migratory waterfowl and Charadriiformes (shorebirds) can be infected with loNDV and vNDV and can shed NDV without any apparent clinical signs of illness. Infection of domestic poultry with naturally circulating loNDV can contribute to respiratory distress in young naive birds and lower productivity in adult birds.
Transmission of Newcastle Disease in Poultry
Infected birds shed virus in exhaled air, respiratory discharge, and feces. Virus is shed during the incubation period, during the clinical stage, and for a varying but limited period during convalescence. Virus may also be present in all parts of the carcass and in eggs laid during acute vNDV infections.
The role of vertical transmission of NDV is unclear and disputable because hatchlings can become infected by contaminated feces, eggshells, or environment. Chickens are readily infected by aerosols and by ingesting contaminated water or food. Infected chickens and other domestic and wild birds may be sources of NDV.
The main modes of transmission are:
movement of infected birds: poultry; wild, exotic, and companion birds; racing and show birds
movement of poultry products
movement of people and contaminated equipment or litter (main mode of virus transmission between poultry flocks and farms)
Transmission via movement of contaminated feed and vehicles and through poorly inactivated vaccines has a lesser role in virus transmission but has been documented.
Clinical Signs of Newcastle Disease in Poultry
There are no pathognomonic clinical signs for Newcastle disease. Onset is rapid, and signs appear throughout the flock as early as 2 days (average 4–6) after aerosol exposure. Transmission is slower if the fecal-oral route is the primary means of transmission, particularly for caged birds. Young birds are the most susceptible.
Observed clinical signs depend on whether the infecting virus has a predilection for respiratory and digestive systems (viscerotropic) or nervous systems (neurotropic).
Clinical signs of infection with viscerotropic velogenic NDV in chickens include:
lethargy
inappetance (anorexia)
respiratory distress (sometimes birds make a whistling sound)
clear mucus discharge from the mouth
prostration
sudden death (sometimes the only finding)
up to 100% morbidity and mortality, especially in naive populations

In some cases, periorbital and head edema develop. The comb may become blue due to hypoxia, and some strains cause hemorrhage. Birds that do not die within several days after infection may have watery greenish diarrhea and show nervous signs including tremor, twisted necks (torticollis), and opisthotonus (especially in vaccinated poultry).
Egg production may be interrupted or stop completely. Eggs may be abnormal in color, shape, or surface and have watery albumen (may be the only sign in fully vaccinated hens). Well-vaccinated birds may appear clinically normal aside from decreased egg production; however, these birds will shed virus in saliva and feces. Poorly and suboptimally vaccinated birds may develop neurologic signs 10–14 days after infection and may recover.


Pigeon with torticollis.
Courtesy of Dr. Kiril Dimitrov.


Eggs with abnormal shape.
Courtesy of Southeast Poultry Research Laboratory of the USDA Agricultural Research Service.

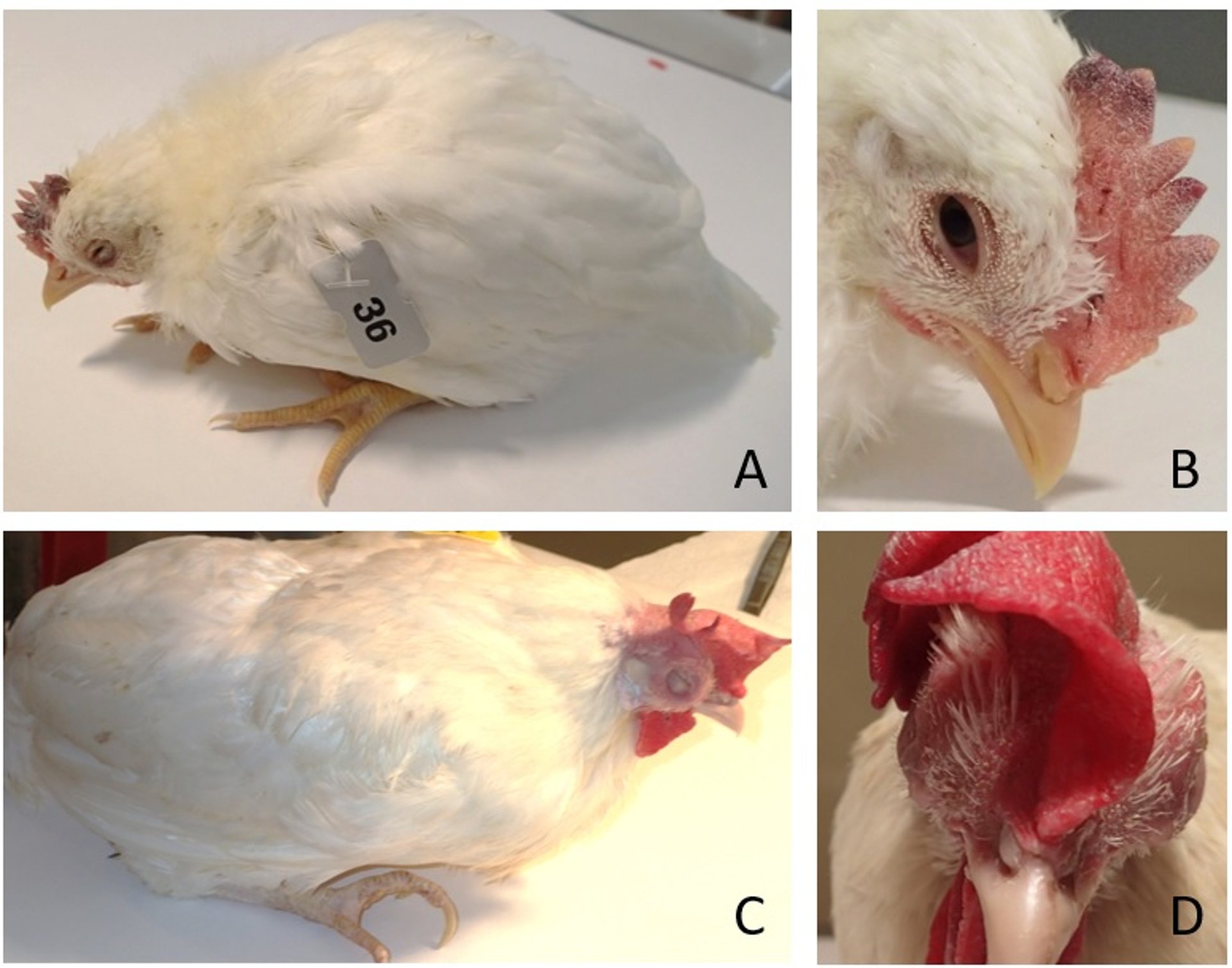
Lethargy in young chicken (A); necrotic/hemorrhagic areas of comb in young chicken (B); lethargy with periorbital edema in adult hen (C); and head swelling in adult hen (D).
Courtesy of Southeast Poultry Research Laboratory of the USDA Agricultural Research Service. Images by Kiril Dimitrov.
Clinical findings of infection with neurotropic velogenic NDV in chickens include respiratory distress with sneezing, coughing, and nasal discharge. Respiratory signs may accompany neurologic signs, but usually follow:
tremors and convulsions
paralysis of wings and legs
torticollis
circling with clonic spasms
complete paralysis
up to 100% morbidity and 50% mortality (up to 90% in young birds)
Clinical signs of infection of chickens with mesogenic NVD include:
respiratory signs with gasping, coughing, sneezing, and rales in young birds
decrease in egg production, which returns to normal in a few weeks
neurologic signs in protracted cases
low mortality (may be higher in young birds)
Infections with loNDV vary from inapparent to an onset with mild respiratory signs, but secondary infections may exacerbate the clinical presentation. While adult birds commonly have subclinical infection, young birds may show gasping, coughing, sneezing, and rales. In turkeys, clinical signs largely resemble those in chickens but often are milder. Decrease in egg production is typical, and eggs have soft shells and abnormal shape.
Conjunctivitis, rhinitis, difficult breathing (dyspnea), diarrhea, and nervous signs (tremors, ataxia, and torticollis) are typical in pigeons. Mortality can reach 40%. Infection in cormorants and exotic birds (particularly psittacines) is characterized by inability to fly and leg and wing paralysis. Infection of chickens with some pigeon- or cormorant-adapted NDV strains may lead to neurologic clinical signs but is inapparent in most cases.
Lesions
Remarkable gross lesions are usually present only in infection with viscerotropic velogenic Newcastle disease viruses. Petechiae may be observed on the serous membranes; hemorrhages of the proventricular mucosa and intestinal serosa are accompanied by multifocal necrotic hemorrhagic areas on the mucosal surface of the intestine, especially at lymphoid foci such as cecal tonsils and Peyer's patches. Splenic and thymic necrosis, hemorrhages, and edema may also be present.

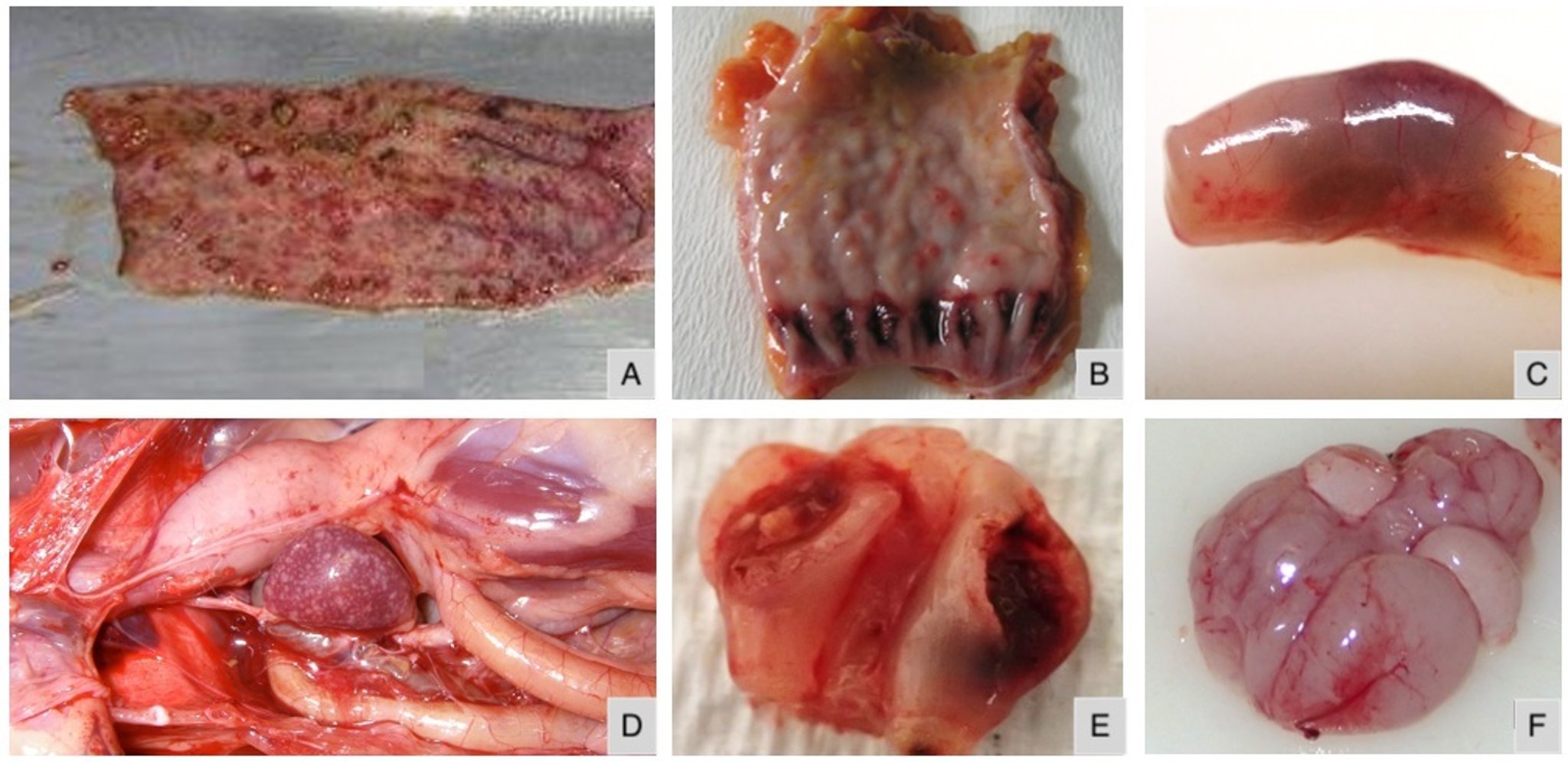
Hemorrhages and necrosis of intestines, longitudinal section (A); hemorrhages in proventricular mucosa (B); intact small intestine with hemorrhages (C); enlarged and mottled spleen with multifocal necrosis (D); necrotic and hemorrhagic cecal tonsils (E); hyperemia and mild multifocal petechial hemorrhages in the meninges of the encephalon due to infection of chickens with cormorant-adapted vNDV (F).
Courtesy of Southeast Poultry Research Laboratory of the USDA Agricultural Research Service.
In chickens, congestion and hemorrhage of the trachea and lung may be observed with velogenic viscerotropic Newcastle disease virus. Egg yolk peritonitis with atrophied follicles may be found in laying birds. In contrast, lesions in birds infected with loNDV strains may be limited to congestion and mucoid exudates present in the respiratory tract with opacity and thickening of the air sacs. Secondary bacterial infections increase the severity of respiratory lesions.
Hyperemia and mild multifocal petechial hemorrhages can be observed in the meninges of the encephalon in infection of chickens with cormorant-adapted NDV strains.
Diagnosis of Newcastle Disease in Poultry
Newcastle disease virus isolation
Detection of vNDV RNA
Detection of NDV-specific antibodies
The clinical signs and gross lesions due to infection with virulent Newcastle disease virus are not pathognomonic and therefore cannot be used alone for diagnosis of Newcastle disease. Laboratory confirmation is required for diagnosis of Newcastle disease.
The virus can be isolated from oropharyngeal or cloacal swabs or tissues from infected birds by inoculation of the allantoic cavity of 9- to 11-day-old SPF embryonated chicken eggs. Infection is confirmed by recovery of a hemagglutinating virus that is inhibited with NDV antiserum or by detection of NDV RNA by real-time RT-PCR. Real-time RT-PCR can be used for detection of viral RNA directly from clinical samples (swabs, tissues, feces, and discharges), and the assay can discriminate vNDV from loNDV.
In the absence of recent vaccination, a rise in NDV antibody titer by hemagglutination-inhibition or ELISA of paired serum samples indicates NDV infection. To confirm diagnosis, identification of an isolate as vNDV is established by the rapidity of killing day-old SPF chicks inoculated by the intracerebral route, the intracerebral pathogenicity index, or genomic sequencing and identification of a specific amino acid motif at the cleavage site of the fusion protein (F) precursor (F0).
Reference laboratories use nucleotide sequence analysis to detect genetic differences for comparison of isolates from different outbreaks and to identify the source of those infections.
Differential Diagnosis of Newcastle Disease in Poultry
The acute form of Newcastle disease should be differentiated from other diseases known to cause high mortality with sudden death, or lethargy and respiratory signs, such as highly pathogenic avian influenza.
Among suboptimally vaccinated birds in whom the onset of clinical signs is not rapid and the mortality is not as high, the mild forms of NDV and infections need to be differentiated from:
Prevention of Newcastle Disease in Poultry
No medication has been shown to impact the course of virulent Newcastle disease virus infection, and treatment with antivirals is not recommended. In cases of flocks affected by loNDV, supportive care with antimicrobials against secondary infections may alleviate clinical signs and decrease morbidity and mortality. Prevention of Newcastle disease is achieved through biosecurity and vaccination.
Biosecurity
Practicing strict biosecurity and implementing strategies to prevent introduction (or transmission) of vNDV into poultry premises are efficient preventive and intervention measures. Routine disinfection procedures, feed and water quality, and pest and litter management should be properly controlled.
Many countries practice outbreak containment by culling infected and susceptible birds in a controlled zone to prevent further transmission of disease. Respective authorities should be immediately notified in case of a suspected vNDV infection. Regulations on the importation of live birds and poultry products, especially from endemic regions, facilitate the control of international transmission of vNDV.
Vaccination
Vaccines are available for chickens, turkeys, and pigeons and are used to induce an antibody response; therefore, vaccinated birds must be exposed to a larger dose of vNDV to be infected. Unfortunately, ND vaccines do not provide sterile immunity, and in many areas of the world, vaccines are used to prevent losses from sickness and death.
While there is an increasing number of reports of Newcastle disease outbreaks in vaccinated poultry, approved vaccines prevent clinical signs of disease under experimental conditions. Passively transferred maternal antibodies and antibodies from previous immunizations impact vaccination against NDV, and vaccination protocols with multiple deliveries (boosters) need to be carefully and properly designed. Field and environmental conditions, as well as concurrent infections, may also negatively impact immune response to vaccination.
Live Virus Vaccines
Live lentogenic virus vaccines, chiefly B1 and LaSota strains, are widely used and typically administered to poultry by mass application in drinking water or by spray. Mucosal immunity induced in birds vaccinated by live virus vaccines applied by these routes decreases the amount of vNDV the vaccinated birds will shed if infected with vNDV, compared with the immune response induced by an inactivated virus vaccine.
Mass vaccination methods are less labor intensive; however, if they are not applied properly, they may lead to < 85% of the flock being immunized, the threshold needed for herd immunity. Alternatively, individual administration of live virus vaccines is via the nares or conjunctival sac. Healthy chicks are vaccinated as early as day 1 of life. However, delaying vaccination until the second or third week avoids maternal antibody interference with an active immune response.
Inactivated Virus Vaccines
Oil-adjuvanted inactivated virus vaccines are also used after live virus vaccine in breeders and layers. They may be used alone in situations where live virus may be contraindicated (eg, in pigeons). In countries where vNDV is endemic, a combination of live and inactivated virus vaccine can be used; alternatively, if permitted by law, a live mesogenic strain virus vaccine may be used in older birds.
The frequency of revaccination to protect chickens throughout life largely depends on the risk of exposure and virulence of the field virus challenge. Administering inactivated virus vaccines is more labor intensive, because each bird has to be handled individually. Accidental inoculation of human tissues with oil-based vaccines requires prompt medical treatment.
Vectored Recombinant Vaccines
Fowlpox or turkey herpesvirus–vectored NDV vaccines are commercially available for chickens and have the advantage of being able to be administered in ovo at the hatchery. These vaccines must be reconstituted as directed by the manufacturer. Because they take 3–4 weeks to produce a protective level of immunity, a window of exposure occurs during which chickens are susceptible to vNDV infection and biosecurity becomes even more important.
Zoonotic Risk of Newcastle Disease in Poultry
All Newcastle disease virus strains can produce a transitory conjunctivitis in humans; however, the condition has been limited primarily to laboratory workers and vaccination teams exposed to large quantities of virus. Before poultry vaccination was widely practiced, conjunctivitis from NDV infection occurred in crews eviscerating poultry in processing plants. The disease has not been reported in people who rear poultry or consume poultry products.
Key Points
Newcastle disease is caused by virulent strains of avian paramyxovirus type 1 (aka Newcastle disease virus).
The disease has no pathognomonic clinical signs or lesions; laboratory confirmation is needed for diagnosis.
Gross lesions include petechiae in the GI tract and edema of the head.
Clinical signs involve the respiratory and often nervous systems, as well as misshapen eggs.
Newcastle disease is successfully controlled by vaccination in commercial poultry, but no treatment is available.
For More Information
Animal disease information: Virulent Newcastle disease (vND). USDA Animal and Plant Health Inspection Service. January 9, 2023. https://www.aphis.usda.gov/aphis/ourfocus/animalhealth/animal-disease-information/avian/virulent-newcastle/vnd
Emergency management: Virulent Newcastle disease (vND). USDA Animal and Plant Health Inspection Service. December 7, 2022. https://www.aphis.usda.gov/aphis/ourfocus/animalhealth/emergency-management/vnewcastle-disease
Suarez DL, Miller PJ, Koch G, Mundt E, Rautenschlein S. Newcastle disease, other avian paramyxoviruses, and avian metapneumovirus infections. In: Swayne DE, Boulianne M, Logue CM, McDougald CR, Nair V, Suarez DL, et al, eds. Diseases of Poultry. 14th ed. Wiley-Blackwell; 2020;111–166. doi:10.1002/9781119371199.ch3
Dimitrov KM, Afonso CL, Yu Q, Miller PJ. Newcastle disease vaccines—A solved problem or a continuous challenge? Vet Microbiol. 2017;206:126–136. doi:10.1016/j.vetmic.2016.12.019





