



Ethylene glycol toxicosis is often fatal and primarily affects dogs and cats, though all species are susceptible. Most commonly found in vehicle radiator antifreeze, it is also available in a variety of other automotive and household products. Systemic effects include metabolic acidosis, gastrointestinal irritation, early CNS depression, and cerebral edema, progressing to irreversible acute kidney failure. The toxic metabolite of ethylene glycol is oxalic acid, which binds to calcium, resulting in formation of calcium oxalate crystals in the proximal renal tubules. Treatment requires early intervention with fomepizole (4-methylpyrazole) or ethanol.
All animals are susceptible to ethylene glycol toxicosis; however, dogs and cats are most commonly affected. Most cases are associated with ingestion of antifreeze, in which concentrations of ethylene glycol up to 95% are common. These concentrated commercial antifreeze preparations are diluted ~50% with water when used in vehicle cooling systems. For user convenience, a wide variety of ready-to-use products are marketed as 50/50 prediluted ethylene glycol. The widespread availability of antifreeze, its sweet taste, and small minimum lethal dose, along with improper storage, use, and disposal contribute to the frequency of ethylene glycol toxicosis.
Since 2012, antifreeze and engine coolant manufacturers in the United States have added a bittering agent to their products to deter voluntary ingestion; however, the products still may be palatable to some animals. Other sources of ethylene glycol include some heat-exchange fluids used in solar collectors, ice-rink freezing equipment, and some brake and transmission fluids. Cutaneous absorption from topical products that contain ethylene glycol has been reported to cause toxicosis in cats.
Ethylene glycol intoxication occurs most commonly in temperate and cold climates, because antifreeze is used both to decrease the freezing point and to increase the boiling point of radiator fluid. In colder climates, the incidence of ethylene glycol intoxications is seasonal, with most cases occurring in the fall, winter, and early spring, when antifreeze is added to radiator fluid or when cooling systems are flushed.
The minimum lethal dose of undiluted ethylene glycol is 1.4 mL/kg in cats, 4.4–6.6 mL/kg in dogs, 7–8 mL/kg in poultry, 2–10 mL/kg in cattle, 1.6 mL/kg in macaques, and 6.61 mL/kg in guinea pigs. Younger animals may be more susceptible.
Pathogenesis of Ethylene Glycol Toxicosis in Animals

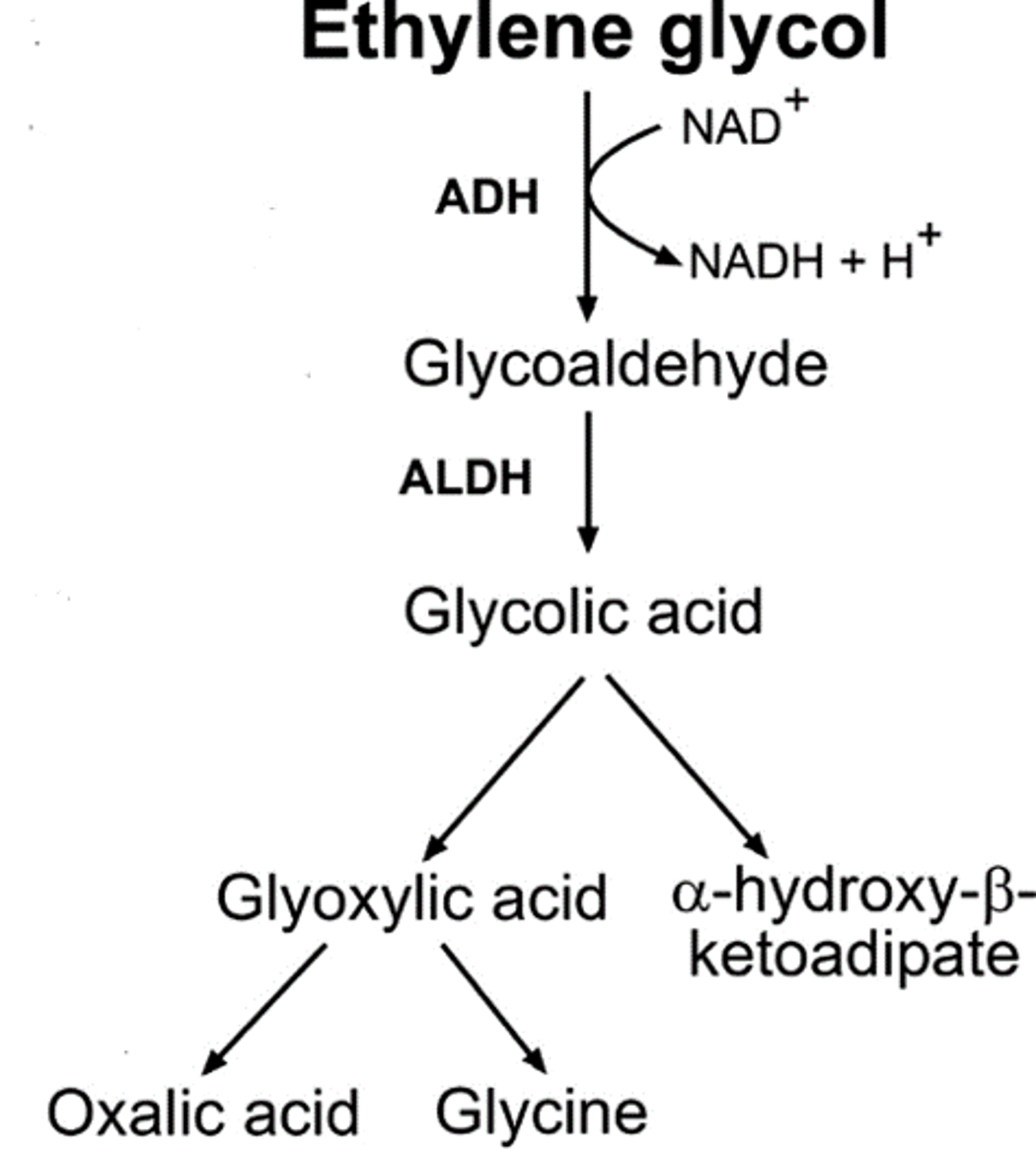
Courtesy of Dr. Tabatha Regehr.
Ethylene glycol is rapidly absorbed from the gastrointestinal tract, with peak absorption in 1–4 hours and a serum half-life of 3 hours. Approximately 50% of ingested ethylene glycol is excreted unchanged by the kidneys; however, a series of oxidation reactions in the liver and kidneys metabolizes the remaining ethylene glycol. Toxic metabolites of ethylene glycol cause severe metabolic acidosis and renal tubular epithelial damage.
The first of two rate-limiting biotransformation steps is the production of glycolaldehyde from ethylene glycol by the enzyme alcohol dehydrogenase. Glycolaldehyde is then rapidly metabolized to glycolic acid. The oxidation of glycolic acid to glyoxylic acid is the second rate-limiting step, which allows glycolic acid to accumulate, resulting in acidosis and nephrotoxicosis. Glyoxylic acid is rapidly metabolized to oxalic acid, glycine, formic acid, and other metabolites. Oxalate is not further metabolized and is cytotoxic to the renal tubular epithelium and exacerbates the metabolic acidosis. Glycolic acid and oxalate are the metabolites thought to be most responsible for acute tubular necrosis associated with ethylene glycol ingestion. Oxalate also combines with calcium to form a soluble complex that is excreted via glomerular filtration. Calcium oxalate crystals form within the lumens of the renal tubules as water is reabsorbed from the glomerular filtrate and the pH decreases (smaller numbers of calcium oxalate crystals may also be observed in the adventitia of blood vessel walls throughout the body).
Clinical Findings of Ethylene Glycol Toxicosis in Animals
Clinical signs are dose- and time-dependent and can be divided into those caused by unmetabolized ethylene glycol and those caused by its toxic metabolites.
Cats and dogs, 30 minutes to 12 hours after ingestion:
Clinical signs mimic ethanol (alcohol) intoxication
Gastrointestinal signs: vomiting
Polydipsia, polyuria
CNS signs: depression, stupor, ataxia, knuckling, decreased proprioception
Brief recovery may occur approximately 12 hours after ingestion
Cats, 12 to 24 hours after ingestion and dogs, 36–72 hours after ingestion:
Oliguric acute kidney failure precedes anuria
Abdomen: painful and enlarged kidneys
Cardiopulmonary signs: tachycardia, tachypnea
Gastrointestinal signs: anorexia, vomiting, diarrhea, oral ulcers, salivation
CNS signs: lethargy, possible seizures, coma, death
Dehydration
Pigs
Gastrointestinal signs: abdominal distension
CNS signs: depression, weakness, reluctance to move, knuckling, ataxia, trembling, collapse
Cardiopulmonary signs: pulmonary edema, muffled heart sounds
Poultry
Gastrointestinal signs: watery feces
CNS signs: drowsiness, ataxia, recumbency; torticollis
Respiratory signs: dyspnea
Ruffled feathers
Cattle
CNS signs: depression, ataxia, paraparesis, recumbency
Epistaxis, hemoglobinuria (larger doses)
Lesions
Renal tubular epithelial necrosis with calcium oxalate crystals in the tubular lumina is characteristic. Calcium oxalate crystals appear birefringent when viewed with polarized light. Pulmonary edema and hemorrhagic gastroenteritis are common secondary findings in dogs and cats. Pigs and cattle often develop renal and perirenal edema. Pigs may also have pulmonary edema with tan fluid in the pleural and peritoneal cavities. Poultry usually do not develop gross lesions.
Diagnosis of Ethylene Glycol Toxicosis in Animals
History, physical examination, and laboratory data
Rapid confirmation via a point-of-care semiquantitative test or measurement of serum ethylene glycol concentration
Without observed ingestion, diagnosis is based on a combination of history, physical examination, and laboratory data. The initial diagnostic profile includes a CBC, serum biochemical analysis, urinalysis including microscopic examination of sediment, blood gas evaluation, and a qualitative or quantitative ethylene glycol test.
Point-of-care, semiquantitative serum ethylene glycol tests for cats and dogs have a minimum level of detection at 20 mg/dL. These colorimetric tests identify a minimum lethal dose for cats at 20 mg/dL and for dogs at 50 mg/dL. This test should be run between 1 and 10–14 hours after ingestion. A combination point-of-care test includes a plasma oxalate concentration to be processed 8–10 hours after ingestion to 24–36 hours after ingestion. Level of detection starts at 0.25 mg/dL. This can both aid in confirming a later-stage ethylene glycol exposure and when estimating prognosis. As serum oxalate concentration increases, prognosis worsens. Quantitative tests are extremely reliable; however, availability is restricted to large specialty hospitals and reference laboratories, which may result in a delay in treatment. Hospital laboratories for human patients that are willing to process samples from veterinary patients may provide rapid quantitative ethylene glycol test results.
Within 3 hours of toxic ingestion, dogs and cats will have metabolic acidosis, an increased anion gap, minimally concentrated or isosthenuric urine with an acidic pH, and marked serum hyperosmolality with an increased osmole gap. Calcium oxalate crystalluria indicates a poor prognosis; it may occur as early as 3 hours after ingestion in cats and 6 hours in dogs. Monohydrate calcium oxalate and dihydrate calcium oxalate crystals may be observed on microscopic evaluation of urine sediment. Monohydrate calcium oxalate crystals are most commonly observed. Historically, urine has been visually assessed under a Wood's lamp because some antifreeze preparations may fluoresce due to the presence of fluorescein. Treatment should begin based on a presumptive diagnosis if no reliable confirmatory testing is available.
Treatment of Ethylene Glycol Toxicosis in Animals
Intravenous fluid therapy
4-methylpyrazole (4-MP, fomepizole), 20% ethanol boluses, or 30% ethanol constant-rate infusion
Supportive care including treatment of metabolic derangements
Gastrointestinal support
Treatment of ethylene glycol toxicosis is aimed at decreasing absorption of ingested ethylene glycol, increasing excretion of unmetabolized ethylene glycol, preventing metabolism of ethylene glycol, and correcting metabolic derangements. Further absorption of ethylene glycol is prevented by induction of emesis, gastric lavage, or both within 1–2 hours of ingestion. However, the rapidity of ethylene glycol absorption from the GI tract suggests these procedures may not be beneficial. Vomiting should not be induced in a dog or cat exhibiting neurologic signs because of increased risk of aspiration. Activated charcoal is not likely to decrease absorption of ethylene glycol from the GI tract.
Once absorption has occurred, excretion of ethylene glycol is increased by fluid therapy designed to correct dehydration, increase urine production, and compensate for expected future losses. Fluid rates should be reassessed often to accommodate changes in hydration and status of ongoing losses.
Fluid replacement volume per hour = Dehydration deficit in mL per hour + Estimated ongoing losses in mL per hour + Maintenance rate fluids [(30 × kg body wt) + 70] ÷ 24 hours in mL per hour
Dehydration should be corrected over 8–12 hours = [(% dehydration) × kg body weight] ÷ 8 (up to 12) hours
Estimated projected losses should be replaced over 4–6 hours = [fluid loss projection ÷ 4 (up to 6) hours]
Calculate maintenance fluid rate per hour = [(30 × kg body wt) ÷ 70] ÷ 24 hours
To prevent metabolism of ethylene glycol, the activity of alcohol dehydrogenase is decreased by direct inactivation or by competitive inhibition. In dogs, 4-methylpyrazole (4-MP, fomepizole) effectively inactivates alcohol dehydrogenase without the adverse effects of ethanol and is the treatment of choice. The dosage for dogs of 4-MP (5% solution [50 mg/mL]) is 20 mg/kg body wt, IV, initially, followed by 15 mg/kg, IV, at 12 and 24 hours, and 5 mg/kg, IV, at 36 hours. Commercial formulations of 4-MP are available. If 4-MP is not available, an ethanol regimen (5.5 mL of 20% ethanol per kg body wt, IV, every 4 hours for five treatments and then every 6 hours for four additional treatments) is recommended.
Cats require a higher (and extra-label) dosage 4-MP than dogs: 125 mg/kg initially, followed by 31.3 mg/kg at 12, 24, and 36 hours after the initial dose. Alternatively, ethanol can be administered, using a bolus protocol of 5 mL of 20% ethanol per kg body wt diluted in IV fluids and administered as a drip over 6 hours for five treatments, and then over 8 hours for four more treatments.
Lastly, for both dogs and cats, 30% ethanol can be administered at 1.3 mL/kg, IV bolus, followed by 0.42 mL/kg per hour constant-rate infusion for 48 hours. This approach may increase ease of monitoring and the maintenance of blood glucose levels. CNS signs may be less likely to wax and wane.
Severe metabolic acidosis (pH < 7.2, bicarbonate < 12 mEq/L) associated with metabolism of ethylene glycol is corrected by administration of sodium bicarbonate. The formula 0.3 − (0.5 × kg body wt) × (24 − plasma bicarbonate) is used to determine the dose, in mEq, of bicarbonate. One-half of this dose should be administered intravenously, slowly to prevent overdose, and plasma bicarbonate concentrations should be monitored every 4–6 hours. Additional doses of bicarbonate based on the above formula are frequently necessary. Monitoring urine pH may also be helpful, with a goal of maintaining the urine pH between 7.0 and 7.5.
Hypoglycemia, a common sequela of ethylene glycol intoxication, can be corrected by supplementing 2.5%–5.0% dextrose while monitoring blood glucose every 4–6 hours. Corrections for hypocalcemia require the ability to monitor serum calcium levels, with ionized calcium testing preferred to total calcium. In dogs, 10% calcium gluconate is administered at 50–150 mg/kg (0.5–1.5 mL/kg) over 20–30 minutes; for cats, 94–140 mg/kg (0.94–1.4 mL/kg) is administered over the same period of time. An ECG should be monitored continuously during administration of intravenous calcium products while also monitoring serum calcium levels.
Urine output, especially in severely compromised patients, should be quantified to determine whether oliguria (0.5 mL of urine per kg per hour) or anuria (< 0.5 mL of urine per kg per hour ) are present. In dogs and cats with azotemia or in oliguric acute kidney failure (urine output of 0.5 mL/kg per hour) or anuric kidney failure (urine output < 0.5 mL/kg per hour), inhibition of alcohol dehydrogenase is of little benefit, because almost all of the ethylene glycol has already been metabolized. Diuresis can be attempted; however, the prognosis for these patients is guarded to poor.
Key Points
Prognosis varies inversely with the amount of time that elapses between ingestion and initiation of treatment.
Point-of-care testing or the ability to obtain a quantified serum ethylene glycol concentration shortly after exposure can decrease the amount of time between exposure and the start of treatment.
Crystalluria, azotemia with oliguria, and anuria are poor prognostic indicators.
For More Information
Jandrey KE, Farrell KS. Ethylene Glycol. In: Hovda LR, Brutlag AG, Poppenga RH, Peterson KL, eds. Blackwell’s Five-Minute Veterinary Consult Clinical Companion, 2nd ed. Ames, IA, Wiley Blackwell 2016, 78–84.
Thrall MA, Connally HE, Grauer, GF, Hamar, DW. Ethylene Glycol. In: Peterson, ME. Talcott PA, eds. Small Animal Toxicology, 3rd ed., St. Louis, MO, Elsevier Saunders 2013, 551–567.
Also see pet health content regarding ethylene glycol poisoning.






