



Teschovirus encephalomyelitis (TE) is a sporadic disease of swine caused by neurotropic infection with Teschovirus A (TV A). The severity of clinical signs correlates with the severity and distribution of lesions within the spinal cord and brain. The disease was initially reported in 1929 in the district of Teschen, Czech Republic (Teschen disease), and it was later recognized in England (Talfan disease) and Denmark (benign enzootic paresis). Severe outbreaks are usually associated with highly pathogenic strains of Teschovirus A1, whereas less-severe outbreaks are frequently associated with other genotypes (ie, TV A2, A3, A4, A5, A6 and A11). Currently, commercial vaccines are unavailable for prevention of teschovirus encephalomyelitis, and treatment of affected animals is frequently palliative, consisting of supportive care. No outbreaks of CNS disease have been associated with Teschovirus B.
Etiology, Epidemiology, and Pathogenesis of Teschovirus Encephalomyelitis
Teschovirus A, genus Teschovirus, family Picornaviridae (previously porcine teschovirus), the etiologic agent of TE, is a single-stranded, linear, nonsegmented RNA virus. Teschovirus A includes 14 different known genotypes (TV A1–A14), although only a few have been associated with CNS disease. Wild boars (Sus scrofa) and domestic pigs (Sus Scrofa f domesticus) have been identified as the natural host for Teschovirus A. It is unknown whether other animals are susceptible to natural infection.
The most severe forms of TE are associated with highly pathogenic strains of Teschovirus A1 (TV A1). The virus is ubiquitous and has a worldwide distribution. Outbreaks of disease associated with neuropathogenic strains other than TV A1 have been widely reported.
Economic losses in affected herds can be extensive, and currently there are no effective treatments. TV A strains not previously described appear to be emerging, in addition to strains that have traditionally predominated. A majority of infections are asymptomatic; clinical signs of disease are thought to occur sporadically. The virus is consistently found in feces from all age categories.
The pathogenicity of all serotypes has not been fully assessed, and sero(geno)types can be further divided into different biotypes that can be either pathogenic or nonpathogenic. The different genotypes of Teschovirus A conceptually exist in nature as quasispecies, and events of interspecies recombination have been described. In the past, TV A has also been implicated as the putative cause of reproductive (abortions), respiratory, and gastroenteric (diarrhea) disease. In 1959, with the release of the FAO/WHO/OIE Animal Health Yearbook, TE was made internationally notifiable. In 2006, the OIE removed former List B of notifiable diseases, establishing a single list (OIE listed diseases) that excluded the reporting of TE as a notifiable disease. However, in many countries, outbreaks of TE must still be reported to regulatory authorities.
Direct and indirect contact with secretions (mostly feces) from infected animals has been reported as the most relevant route of transmission for TV A. After oral ingestion, the virus replicates in the tonsils and in different portions of the gastrointestinal tract. The large intestine and the ileum appear to be more prone to primary replication when compared with other segments of the gastrointestinal tract; however, differences across genotypes may exist. Some studies have documented a transient viremia after the initial replication in the gastrointestinal tract, while other research has suggested that the virus enters via neurons within the enteric nervous system and disseminates to the CNS by retrograde axonal transport. Both routes of dissemination have been documented.
Clinical Findings of Teschovirus Encephalomyelitis


The incubation period of teschovirus encephalomyelitis is variable but typically is approximately 8–14 days postexposure. Initial clinical signs may include pyrexia, lethargy, anorexia, and, less commonly, diarrhea. Locomotor deficits (ataxia, hypermetria, paresis, and hemiparesis) are usually the first clinical signs noted by attending veterinarians. The severity and progression of clinical signs is highly dependent on the infectious dose, the neurovirulence of the strain involved (highly pathogenic versus low pathogenic), and the presence of homologous neutralizing antibodies in the affected animal. In mild cases, animals may recover days after the onset of disease. In severe cases, disease progression is followed by severe clinical signs (lateral recumbency, tremors, flaccid paralysis, nystagmus, and opisthotonus). In terminal stages, dehydration, hypothermia, and coma are commonly reported. Death follows shortly after.
Lesions
No specific gross lesions are observed within the CNS. Lesions in other organs are nonspecific and usually are related to prolonged prostration. Occasionally, soft intestinal and colonic contents may be noted in necropsy. Histologic lesions are characterized as mild to severe and include multifocal nonsuppurative encephalomyelitis, with degeneration and necrosis of neurons particularly affecting the grey substance in the ventral horns of the spinal cord; also lymphocytic infiltration of perivascular spaces, multifocal areas of gliosis, satellitosis and ganglioneuritis of spinal root, and spinal ganglion.
Diagnosis of Teschovirus Encephalomyelitis
Presumptive diagnosis by evaluation of histologic lesions post-mortem.
The absence of specific gross lesions at necropsy and a previous history of disease supports a presumptive diagnosis.
Diagnostic confirmation requires virus isolation via specific laboratory testing, ruling out similar viral illnesses
A presumptive diagnosis of teschovirus encephalomyelitis is mostly achieved by means of evaluation of histologic lesions in animals that die (or are euthanized). Submission of samples for laboratory analysis of multiple segments of spinal cord (lumbar, thoracic, cervical), brainstem, cerebellum, and cerebrum (fresh and fixed in formalin) is essential for accurate diagnosis. Recently, with the identification of other neurotropic viral infections in swine (eg, porcine astrovirus type 3, Sapelovirus A), the diagnosis of TE has become more challenging; it is difficult to differentiate clinical disease and histologic lesions from TE from those due to other viruses. Multiple diagnostic techniques (virus isolation, PCR assay, in situ hybridization, next-generation sequencing, immunofluorescence) can identify the agent or detect the specific immune response mounted against the virus (ELISA, agar gel immunodiffusion, complement fixation and virus neutralization) and are available to identify TV A. Definitive diagnosis requires viral isolation from CNS samples of affected animals obtained aseptically, with the ruling out of other neurotropic agents.

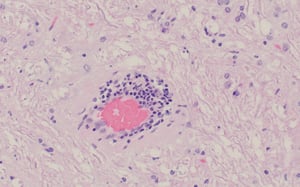
Affected blood vessels are cuffed with lymphocytes and plasma cell and may have a reactive endothelium.
Affected blood vessels are cuffed with lymphocytes and plasma cell and may have a reactive endothelium.
Courtesy of Dr. Matias Ferreyra.
Photomicrograph of marked perivascular mononuclear cuffing. Rarely, there are scattered eosinophils within the infiltrate. This is frequently observed in affected animals that are markedly dehydrated and cannot reach water outlets (secondary salt toxicosis). This lesion in some cases is almost indistinguishable from chronic salt toxicosis, so other ancillary molecular methods are needed for proper diagnosis.
Photomicrograph of marked perivascular mononuclear cuffing. Rarely, there are scattered eosinophils within the infiltra
Courtesy of Dr. Matias Ferreyra.
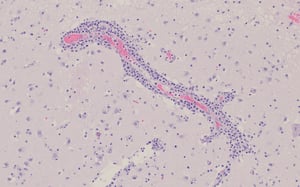
Photomicrograph of a focally extensive area of gliosis between a group of mildly degenerated neurons with mild cuffing of capillary perivascular spaces.
Photomicrograph of a focally extensive area of gliosis between a group of mildly degenerated neurons with mild cuffing
Courtesy of Dr. Matias Ferreyra.
Multifocal blood vessels are cuffed by up to 6-cell thick concentric layers of mononuclear cells, chiefly lymphocytes and plasma cells, and there is an increased number of glial cells within the neuropil, focally forming a glial nodule between affected vessels.
Multifocal blood vessels are cuffed by up to 6-cell thick concentric layers of mononuclear cells, chiefly lymphocytes a
Courtesy of Dr. Matias Ferreyra.
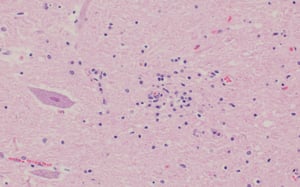
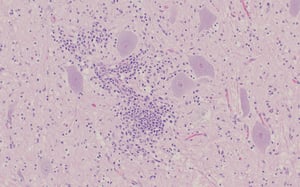
An area of mild perivascular cuffing and gliosis is adjacent to a hypereosinophilic angular neuron.
An area of mild perivascular cuffing and gliosis is adjacent to a hypereosinophilic angular neuron.
Courtesy of Dr. Matias Ferreyra.
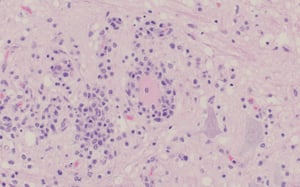
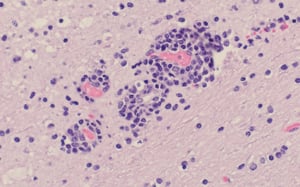
The mononuclear infiltrate surrounds a necrotic neuron. Adjacent neurons are mildly to moderately degenerated, and there is concurrent gliosis, astrocytosis, and mild perivascular cuffing.
The mononuclear infiltrate surrounds a necrotic neuron. Adjacent neurons are mildly to moderately degenerated, and ther
Courtesy of Dr. Matias Ferreyra.
Affected blood vessels are cuffed with lymphocytes and plasma cell and may have a reactive endothelium.
Affected blood vessels are cuffed with lymphocytes and plasma cell and may have a reactive endothelium.
Courtesy of Dr. Matias Ferreyra.
Photomicrograph of marked perivascular mononuclear cuffing. Rarely, there are scattered eosinophils within the infiltrate. This is frequently observed in affected animals that are markedly dehydrated and cannot reach water outlets (secondary salt toxicosis). This lesion in some cases is almost indistinguishable from chronic salt toxicosis, so other ancillary molecular methods are needed for proper diagnosis.
Photomicrograph of marked perivascular mononuclear cuffing. Rarely, there are scattered eosinophils within the infiltra
Courtesy of Dr. Matias Ferreyra.
Photomicrograph of a focally extensive area of gliosis between a group of mildly degenerated neurons with mild cuffing of capillary perivascular spaces.
Photomicrograph of a focally extensive area of gliosis between a group of mildly degenerated neurons with mild cuffing
Courtesy of Dr. Matias Ferreyra.
Multifocal blood vessels are cuffed by up to 6-cell thick concentric layers of mononuclear cells, chiefly lymphocytes and plasma cells, and there is an increased number of glial cells within the neuropil, focally forming a glial nodule between affected vessels.
Multifocal blood vessels are cuffed by up to 6-cell thick concentric layers of mononuclear cells, chiefly lymphocytes a
Courtesy of Dr. Matias Ferreyra.
An area of mild perivascular cuffing and gliosis is adjacent to a hypereosinophilic angular neuron.
An area of mild perivascular cuffing and gliosis is adjacent to a hypereosinophilic angular neuron.
Courtesy of Dr. Matias Ferreyra.
The mononuclear infiltrate surrounds a necrotic neuron. Adjacent neurons are mildly to moderately degenerated, and there is concurrent gliosis, astrocytosis, and mild perivascular cuffing.
The mononuclear infiltrate surrounds a necrotic neuron. Adjacent neurons are mildly to moderately degenerated, and ther
Courtesy of Dr. Matias Ferreyra.
Differential diagnoses include neurotropic infections due to porcine astrovirus type 3, Sapelovirus A, porcine reproductive and respiratory syndrome virus (PRRSV), porcine circovirus 2 (PCV2), suid herpesvirus 1 (pseudorabies), classical swine fever virus, Japanese encephalitis virus, porcine hemagglutinating encephalomyelitis virus and rabies virus. Other differentials include, salt, selenium, and insecticide intoxication, aflatoxicosis, lead poisoning, peracute cases of S suis meningoencephalitis, and edema disease (enterotoxigenic strains of Escherichia coli).
Treatment and Control of Teschovirus Encephalomyelitis
Treatment of affected animals is palliative, including supportive care
Rapid diagnosis and appropriate biosecurity measures are key to controlling the disease
Complete eradication of Teschovirus A in commercial herds is virtually impossible. Control measures primarily focus on decreasing the likelihood of introduction of new, highly virulent strains. Disease control and spread have been successfully achieved via the implementation of nonspecific strategies, including stamping out of disease in affected areas, vaccination in response to the outbreak (ring vaccination), restriction of animal movements, and disinfection of premises. Currently, disease prevention in countries where highly pathogenic strains of TV A are not endemic is attained mostly by practicing strict general biosecurity measures. Additionally, a timely and appropriate diagnosis followed by the implementation of strict biosecurity measures may decrease the spread of disease in a specific population.
Key Points
The characteristic locomotor clinical signs (ataxia, paresis, paralysis) are frequently the first clinical signs noted by attending veterinarians.
The severity of clinical signs correlates with the severity and distribution of lesions within the spinal cord and brain.
Animal age is an important risk factor when considering the likelihood of severe clinical disease; mature animals appear less susceptible than younger animals (suckling and nursery pigs).
For More Information
Teschovirus Encephalomyelitis in OIE Terrestrial Manual 2018.
Teschovirus Encephalomyelitis and Porcine Teschovirus Infections. The Center for Food Security and Public Health, Iowa State University.
Malik YS, Bhat S, Vlasova AN, et al. Teschovirus. Emerg Transbound Animal Vir. 2020:123–136. Published online 2020 Feb 23. doi: 10.1007/978-981-15-0402-0_6


