



Epidermal Inclusion Cyst in Horses
Epidermal inclusion cysts (also called "atheromas") are unilateral swellings present in the dorsolateral wall of the nasal diverticulum of horses. Diagnosis is made by visual inspection and confirmed by aspiration of characteristic thick, brown fluid from the cyst. Injection of the cyst with 10% formalin or surgical removal is recommended.
Redundant Alar Fold in Horses
Horses with excessive alar folds can present for respiratory noise and/or exercise intolerance. Diagnosis is made by visual inspection and placing a large temporary mattress suture through each alar fold, tying over the bridge of the nose and then working the horse to observe reduced noise or improved tolerance to exercise. Surgical resection of the redundant alar fold is recommended if the diagnosis is confirmed.
Diseases of the Nasal Septum

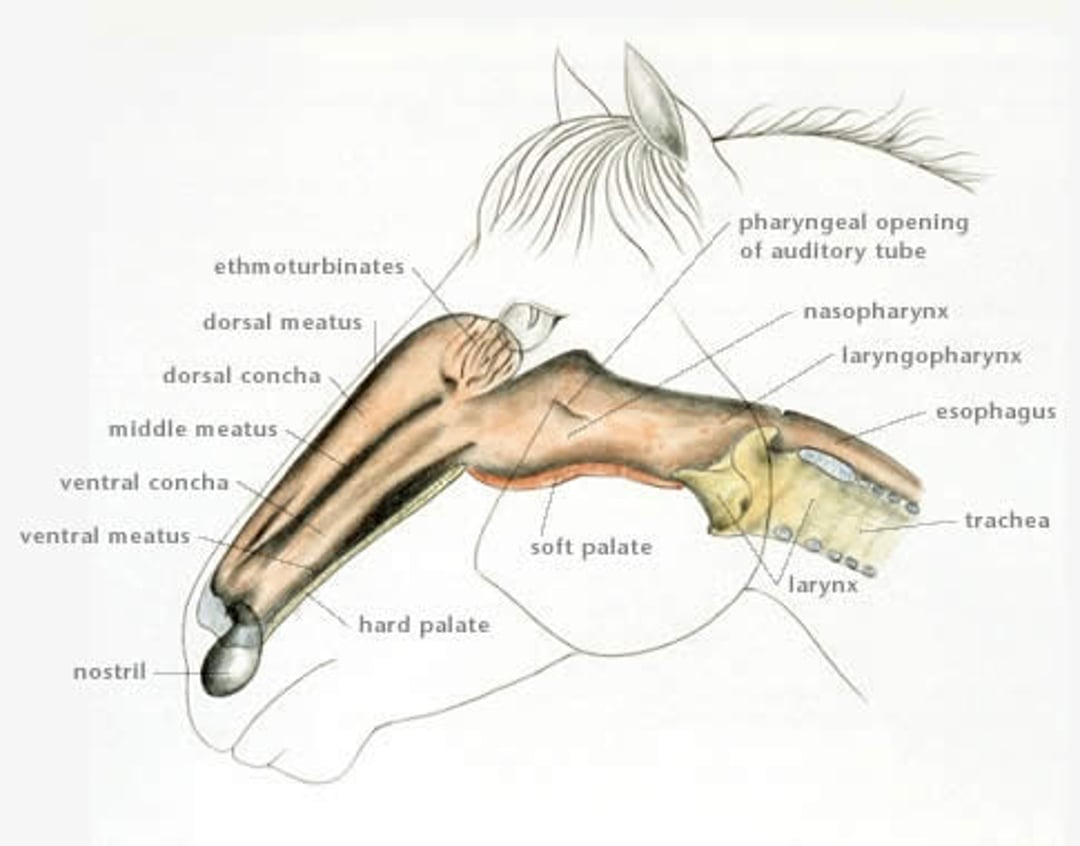
Illustration by Dr. Gheorghe Constantinescu.
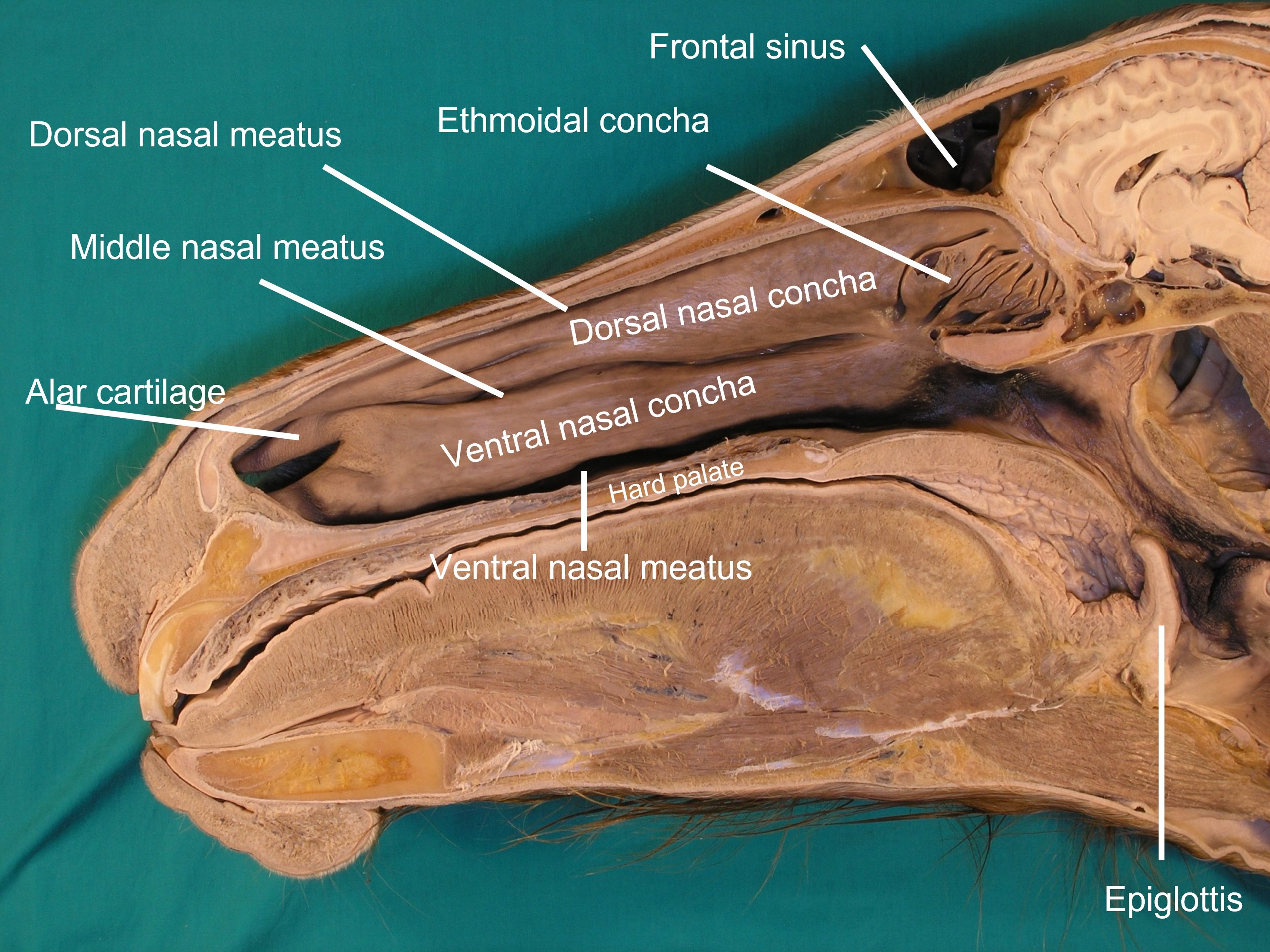
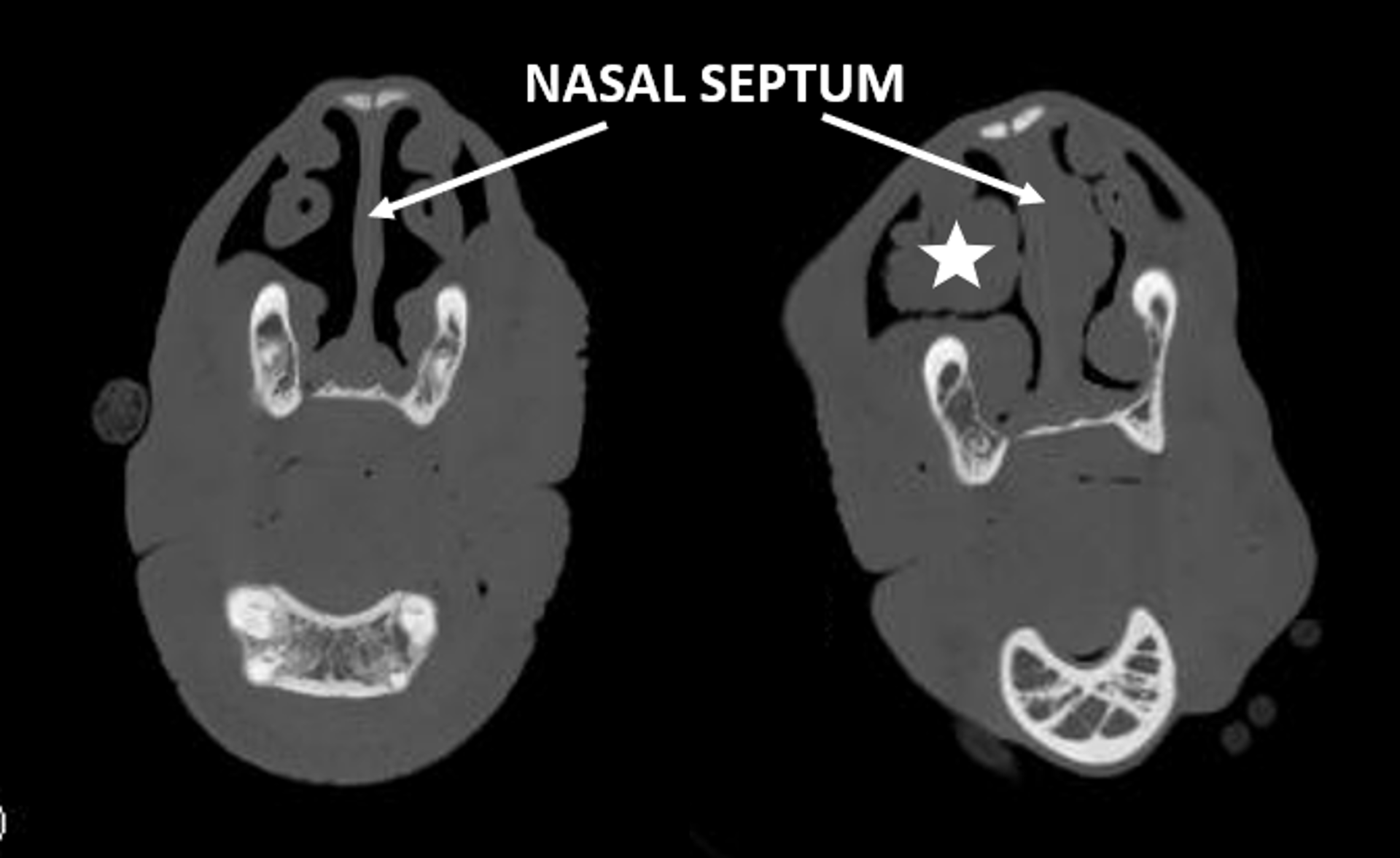
Diseases of the nasal septum are rare. Most nasal septal disorders are congenital abnormalities that remain undetected until the horse is exercised. Traumatic injury to the bridge of the nose as a juvenile can produce nasal septal deviation and thickening. Other less common diseases of the nasal septum include amyloidosis, fungal infection, and squamous cell carcinoma. Thickening or deviation of the nasal septum causes low-pitched stertorous breathing during exercise. Facial deformity may be seen. Septal abnormalities may be detected by palpation, visual inspection, and endoscopic examination. Dimensions of the nasal cavity are difficult to appreciate via endoscopic examination; however, abnormalities of the mucosa are easily identified. Precise dorsoventral radiographs of the skull provide definitive evidence of septal deformity, deviation, and thickening. Additionally, CT scan of the skull can allow precise location of the nasal septal defect and help with surgical planning if nasal septal resection is pursued. Histologic examination of any nodules or discrete lesions on the septum will identify tumors, amyloidosis, or fungal infections.
Surgical resection of the nasal septum is the only treatment option in most cases. The entire diseased portion of the septum can be excised using obstetrical wire by transecting the septum on the dorsal, ventral, and caudal border. Care is taken with transection of the cranial border, leaving at least 5 cm of rostral septum to prevent collapse of the external nares. Hemorrhage can be substantial during this procedure (4–8 L). The nasal passages are packed with sterile gauze soaked in saline or in 1:100,000 epinephrine solution to minimize blood loss. Before the horse recovers from anesthesia, a tracheotomy is performed.
Postoperative care includes parenteral antimicrobials and NSAIDs. The packing and tracheotomy tube are removed 48–72 hours after surgery. All incisions heal by second intention within 3 weeks. Horses should be rested for ~2 months before returning to normal activity. After surgery, most horses make a respiratory noise during work, although less than before surgery, and exercise tolerance is improved. Shortening of the upper jaw, incisor malalignment, or nostril collapse can develop if the procedure is performed in immature horses. Ideally, the surgery should be delayed until maturity.

Courtesy of Dr. Dewey Wilhite, Auburn University.

Courtesy of Dr. Lindsey Boone, Auburn University.
Nasal Polyps
Nasal polyps are pedunculated growths that arise from the mucosa of the nasal cavity, nasal septum, or tooth alveolus. Polyps are usually unilateral and single but can be bilateral and multiple. They form in response to chronic inflammation by hypertrophy of the mucous membrane or exuberant proliferation of fibrous connective tissue. There is no age, breed, or gender predilection.
Clinical signs include:
reduced airflow through affected nasal passage
inspiratory dyspnea
unilateral, malodorous, mucopurulent nasal discharge
low-volume epistaxis
Occasionally nasal polyps extend rostrally and protrude beyond the nostrils. More often, polyps are detected via endoscopic and radiographic examination, and histopathologic evaluation of biopsy samples provide a definitive diagnosis. Surgical excision is performed via an incision in the false nostril, a trephine opening, or a bone flap.
Choanal Atresia
Choanal atresia is a rare, congenital malformation caused by persistence of the bucconasal membrane that separates the primitive buccal or oral cavity from the nasal pits during embryonic development. This membrane prevents passage of air from the nose into the pharynx to pass into the trachea and lungs. Bilateral and unilateral cases have been described in horses. Clinical signs are evident immediately after birth in foals with bilateral disease, because dyspnea is severe and air cannot be detected passing through the nostrils. An endoscope or stomach tube passed through the ventral meatus will be obstructed at the level of the medial canthus of the eye.
Bilateral complete choanal atresia is a life-threatening condition, and a tracheotomy must be performed immediately after birth. It may be possible to perforate the thin membrane via endoscopic laser excision or via a laryngotomy. If the membrane is hard (osseous), a nasal flap centered along the caudal midline of the nasal passage is made to access the membrane for surgical removal. Indwelling tube stents should be inserted through both choanae and left in place for 2–6 weeks to ensure appropriate healing.
Cleft Palate



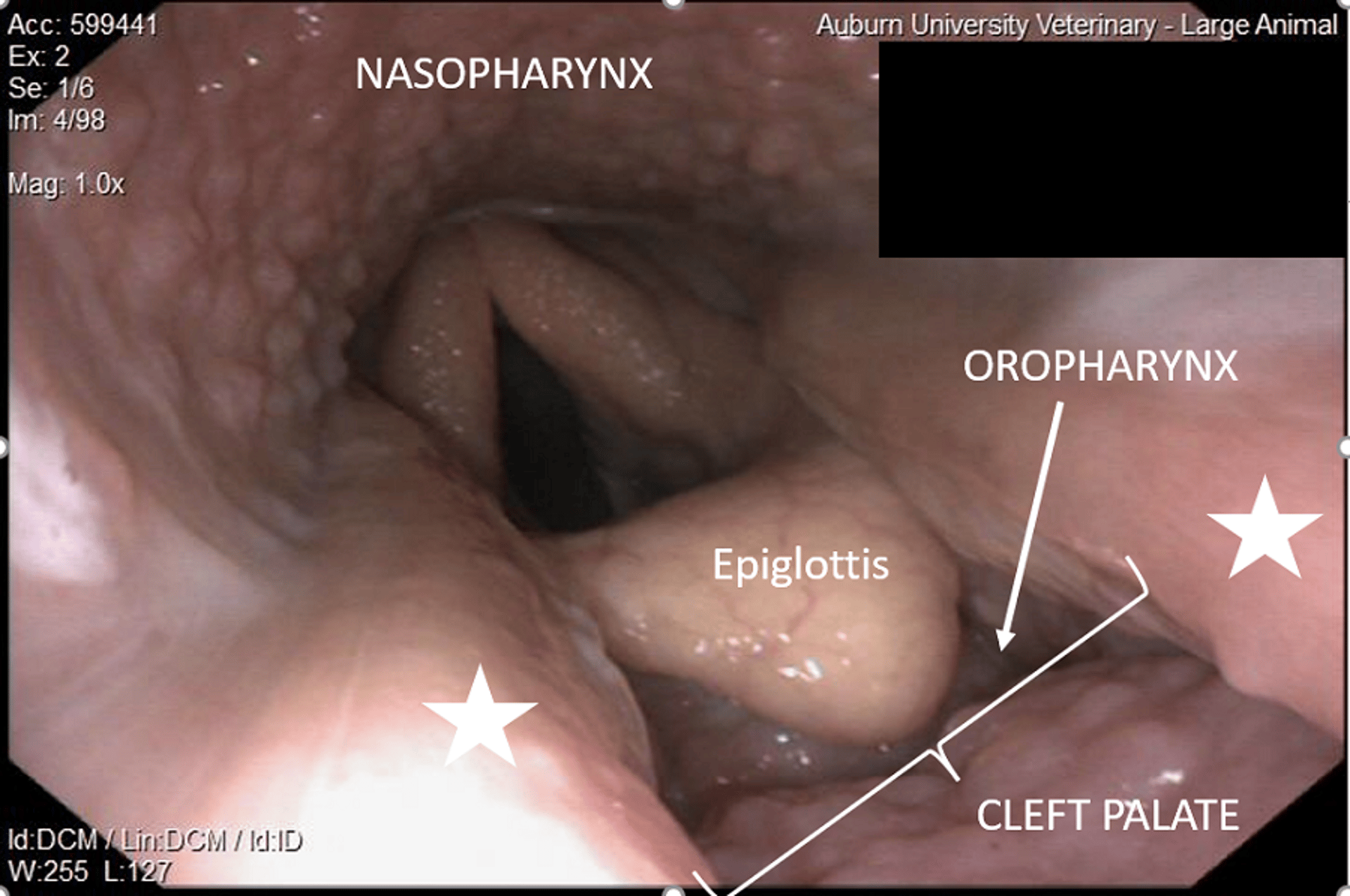
Courtesy of Dr. Lindsey Boone, Auburn University.
Cleft palate is a rare, congenital malformation due to failure of closure of the palatal fold, causing defects in the soft and/or hard palate. Foals may present after owners observe milk dribbling from the nose shortly after nursing and the presence of cough due to aspiration of milk. Diagnosis is made via oral and endoscopic examination of the hard and soft palate. If the cleft is small, involves only the soft palate, and aspiration is minimal, surgery may be delayed to allow treatment of aspiration pneumonia and allow the horse to be more mature before undergoing extensive surgery. If the defect is large (involving > 20% of the soft palate), asymmetric, or involves the hard palate, the prognosis is considered poor and euthanasia should be considered. When surgical correction is elected, the foal must be stabilized beforehand. This includes ensuring adequate passive transfer of immunity and treatment/control of aspiration pneumonia. Surgical repair is performed through the oral cavity, pharyngotomy, laryngotomy, or mandibular symphysiotomy. Postoperatively, foals are treated with parenteral antimicrobials, NSAIDs, and enteral feeding via a nasogastric feeding tube. The most common complication is dehiscence of the surgical repair.
For More Information
Also see pet health content regarding disorders of the nasal passages in horses.






