



Sarcoptic Mange (Canine Scabies) in Dogs

Courtesy of Dr. Michael W. Dryden.
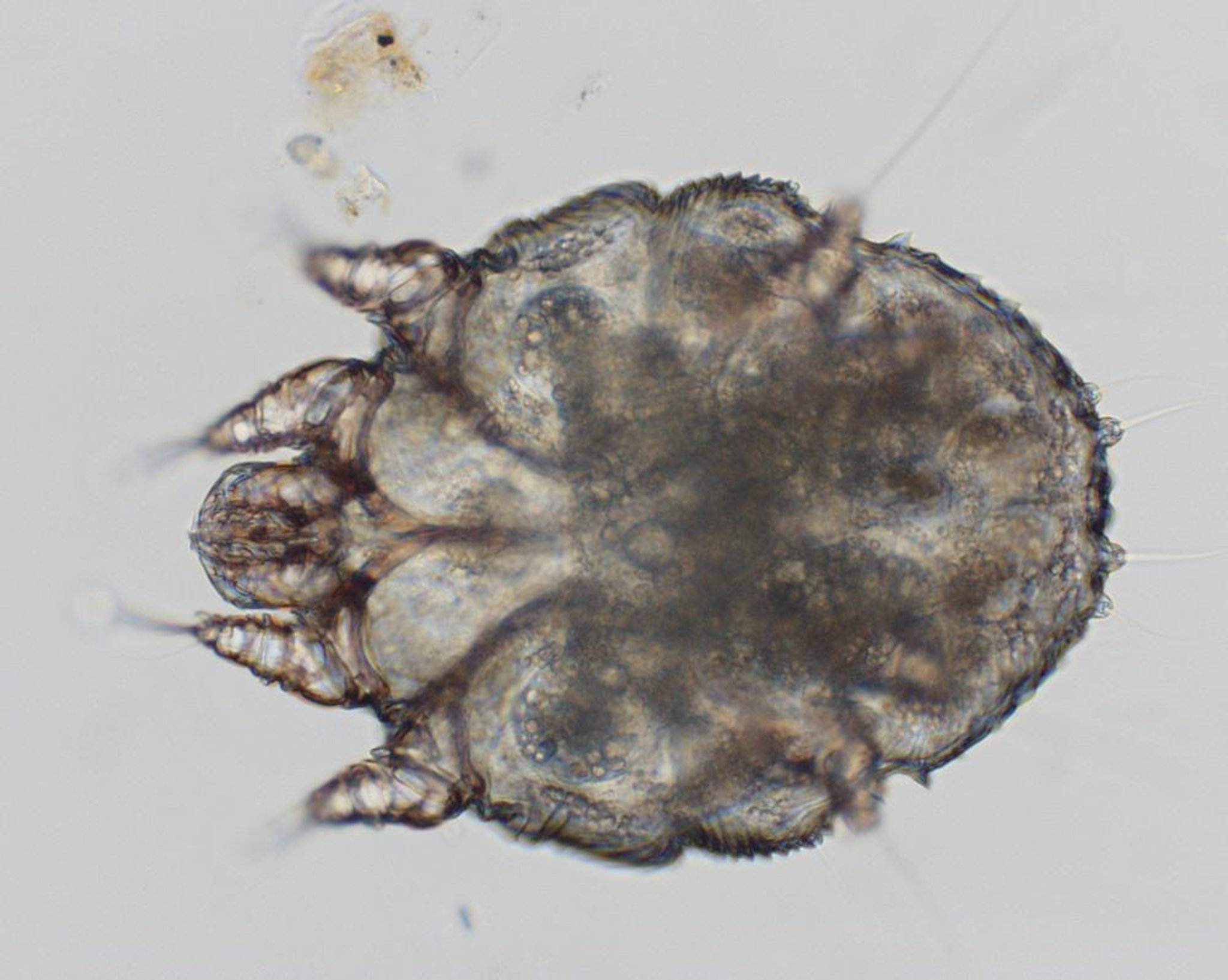
Sarcoptes scabiei var canis infestation is a highly contagious disease of dogs that occurs worldwide. The mites are mostly host specific, but the disease is zoonotic, and humans who come in contact with infested dogs may be infected. Adult mites are 0.2–0.6 mm long and roughly circular in shape; their surface is covered with small, triangular spines, and they have four pairs of short legs. Females are almost twice as large as males. The entire life cycle (17–21 days) is spent on the host dog. Female mites burrow into the stratum corneum to lay their eggs. Sarcoptic mange is readily transmissible between dogs by means of direct contact; transmission via indirect contact may also occur by combs, brushes, towels, and blankets.
Clinical signs of sarcoptic mange may develop anytime from 10 days to 8 weeks after contact with an infested animal. Asymptomatic carriers may exist. Intense pruritus is characteristic and probably due to hypersensitivity to mite products. Primary lesions consist of papulocrustous eruptions with thick, yellow crusts, excoriation, erythema, and alopecia. Secondary bacterial and yeast infections may develop. Typically, lesions start on the ventral abdomen, chest, ears, elbows, and hocks and, if untreated, become generalized.
Dogs with chronic, generalized sarcoptic mange develop seborrhea, severe thickening of the skin with fold formation and crust buildup, peripheral lymphadenopathy, and emaciation; dogs so affected may even die. “Scabies incognito” has been described in well-groomed dogs; these dogs, infested with sarcoptic mites, are pruritic, but demonstrating the mites on skin scrapings is difficult because the crusts and scales have been removed by regular bathing. Atypical, including localized, clinical forms that are probably linked to extensive use of insecticides or acaricides are being increasingly seen.


Courtesy of Dr. Michael W. Dryden.
Diagnosis of sarcoptic mange is based on the history of severe pruritus of sudden onset, possible exposure, and involvement of other animals, including humans. Making a definitive diagnosis is sometimes difficult because of negative skin scrapings. Concentration and flotation of several scrapings may increase chances of finding the mites, eggs, or feces. Several extensive superficial scrapings should be done of the ears, elbows, and hocks; nonexcoriated areas should be chosen. A centrifugation fecal flotation using sugar solutions may reveal mites or eggs. A specific and sensitive commercially available ELISA to detect specific antibodies has been developed and may be useful.
Systemic treatments of scabies are based on administration of macrocyclic lactones, some of which are FDA approved for this purpose. Among them, selamectin is given as a spot-on formulation at 6–12 mg/kg. Selamectin should be administered once as a single topical dose. A second monthly dose may be required in some dogs. This drug is safe, even in ivermectin-sensitive breeds. Another FDA-approved treatment is the imidacloprid-moxidectin formulation, available as a spot-on. It should be given in two doses of 2.5 mg/kg (moxidectin), 4 weeks apart; additionally, although topical application is safe in avermectin-sensitive dogs, oral uptake should be prevented in breeds at risk of avermectin sensitivity.
Other endectocides, such as milbemycin oxime and ivermectin, which are not registered for treatment of sarcoptic mange in dogs, have reportedly been effective depending on the dosage and route of administration. The recommended dosage for milbemycin oxime is 2 mg/kg, PO, weekly for 3–4 weeks; potential toxicity should be considered in dogs with avermectin sensitivity. Ivermectin (200 mcg/kg, PO or SC, 2–4 treatments 2 weeks apart) is very effective and usually curative. Ivermectin at this dosage is contraindicated in avermectin-sensitive breeds. Additionally, the microfilaremic (Dirofilaria immitis) status of the dog should be evaluated before treatment with a macrocyclic lactone.
The new isoxazoline class of drugs (afoxolaner, fluralaner, and sarolaner) have also recently been shown to be effective against sarcoptic mange in dogs. However, none are currently FDA approved.
If older topical treatments are used, hair can be clipped, the crusts and dirt removed by soaking with an antiseborrheic shampoo, and an acaricidal dip applied. Lime sulfur is highly effective and safe for use in young animals; several dips 7 days apart are recommended. Amitraz is an effective scabicide, although it is not approved for this use. It should be applied as a 0.025% solution at 1- or 2-week intervals for 2–6 weeks. In addition, the owner must observe certain precautions to avoid self-contamination. Fipronil spray is reportedly effective but should be considered an aid in control rather than a primary therapy.
Because mites can be difficult to detect, if Sarcoptes is suspected but no mites are found, a therapeutic trial is warranted. This is not an uncommon situation and, frequently, cases of sarcoptic mange are inappropriately treated as another type of allergic skin disease for weeks or months before requiring referral to a board-certified specialist in veterinary dermatology. Additionally, treatment should include all dogs in contact with the infested dog.
Notoedric Mange (Feline Scabies) in Cats
Notoedric mange is a highly contagious disease of cats and kittens caused by Notoedres cati, which can opportunistically infest other animals, including humans. Although uncommon to rare in northern temperate areas, it is not uncommon in subtropical or tropical zones. The mite is similar to the sarcoptic mite, with similar life cycles. Pruritus is severe. Crusts and alopecia are seen, particularly on the ears, head, and neck (face mange), and can become generalized. Mites can be found quite easily in skin scrapings. Treatment is both topical and systemic. Nonapproved but effective and safe treatments include selamectin (6 mg/kg, spot-on) and moxidectin (1 mg/kg, spot-on, in the imidacloprid-moxidectin formulation). Ivermectin (200 mcg/kg, SC) has also been used. Another effective topical therapy is lime sulfur dips at 7-day intervals.
Otodectic Mange in Cats and Dogs
Otodectes cynotis mites are a common cause of otitis externa, especially in cats but also in dogs. Mites that belong to the family Psoroptidae are usually found in both the vertical and horizontal ear canals but are occasionally seen on the body. Clinical signs include head shaking, continual ear scratching, and ear droop. Pruritus is variable but may be severe. Dark brown cerumen accumulation in the ear and suppurative otitis externa with possible perforation of the tympanic membrane may be seen in severe cases. Affected and in-contact animals should receive appropriate parasiticide treatment in the ears. Approved systemic therapies include topically applied selamectin and moxidectin. Direct applications to the external ear canal of cats using approved ivermectin and milbemycin formulations are also effective. As a general rule, ear cleansing with an appropriate ceruminolytic agent is indicated as part of any treatment.
Cheyletiellosis (Walking Dandruff) in Animals


Courtesy of Dr. Michael W. Dryden.
Cheyletiella blakei infests cats, C yasguri infests dogs, and C parasitovorax infests rabbits, although cross-infestations are possible. Chyletiellosis is very contagious, especially in animal communities. Human infestation is frequent. Mite infestations are rare in flea-endemic areas, probably because of the regular use of insecticides. These mites have four pairs of legs and prominent, hook-like mouthparts. They live on the surface of the epidermis, and their entire life cycle (3 weeks) is spent on the host. Female mites can, however, survive for as long as 10 days off the host.
Clinical disease is characterized by scaling, with a dorsal distribution, and pruritus, which varies from none to severe. Cats can develop dorsal crusting or generalized miliary dermatitis. Asymptomatic carriers may exist. The mites and eggs may not be easy to find, especially in animals that are bathed often. Acetate tape preparations, superficial skin scrapings, and flea combing can be used to make the diagnosis.


Courtesy of Dr. Louise Bauck.
Both topical and systemic acaricides are effective against cheyletiellosis, although no drugs are currently approved for this indication. In addition to treatment of the affected animals, it is necessary to treat all in-contact animals. Topical drugs include lime sulfur, fipronil spot-on and spray, permethrin, and amitraz (the latter two are contraindicated in cats). Extra-label systemic drugs include selamectin spot-on, milbemycin oxime (PO), and ivermectin (SC). Care must be taken to avoid or minimize the risks of adverse reactions. The treatment period depends on the selected drug but must be long enough to eradicate the mites from both the animals and their environment, which can be difficult in animal communities (eg, breeding colonies, kennels). In practice, treatment lasts 6–8 weeks and should continue for a few weeks beyond clinical cure until parasitologic cure is achieved.
Canine Demodicosis

Courtesy of Dr. Michael W. Dryden.
Canine demodicosis occurs when large numbers of Demodex canis mites inhabit hair follicles and sebaceous glands. In small numbers, these mites are part of the normal flora of canine skin and usually cause no clinical disease. The mites are transmitted from dam to puppies during nursing within the first 72 hours after birth. The mites spend their entire life cycle on the host, and the disease is not considered to be contagious. The pathogenesis of demodicosis is complex and not completely understood; evidence of hereditary predisposition for generalized disease is strong. Immunosuppression, natural or iatrogenic, can precipitate clinical disease in some cases. Secondary bacterial deep folliculitis, furunculosis, or cellulitis may occur. Two other Demodex species have been recognized, Demodex cynois and Demodex injai, but little is known about their life cycle or pathogenesis.


Courtesy of Dr. Michael W. Dryden.
Three forms of demodicosis are seen in dogs: localized demodectic mange, juvenile-onset generalized demodicosis, and adult-onset generalized demodicosis. Localized demodicosis is seen in dogs usually <1 year old, and most of these cases resolve spontaneously. Lesions often consist of one to five well-demarcated small areas of alopecia, erythema, and scaling. Lesions are usually confined to areas around the lips, periorbital area, and forelimbs but may be found in other locations. Pruritus is usually absent or mild. A small percentage of these cases, especially the diffuse localized forms, progress to a more severe generalized form.
Juvenile-onset generalized demodicosis is the result of an inherited immunologic defect with functional abnormality associated with the cell-mediated immune system. Mites proliferate excessively, causing destruction of the hair follicles they normally inhabit. It is a severe disease of young dogs, with generalized lesions (erythema, papules, alopecia, oily seborrhea, edema, hyperpigmentation, and crusts) that are usually aggravated by secondary bacterial infections (pyodemodicosis). Accompanying pododermatitis is common. Dogs can have systemic illness with generalized lymphadenopathy, lethargy, and fever when deep pyoderma, furunculosis, or cellulitis occurs. Diagnosis is typically not difficult; deep skin scrapings or hair plucking typically reveal mites, eggs, and larval forms in high numbers.
The third form of demodicosis is adult-onset generalized demodicosis and clinically appears similar to juvenile-onset generalized demodicosis but is seen in adult dogs, typically >3 years old, though it may occur in those as young as 1.5 years. It is typically associated with or triggered by a neoplastic process or debilitating disease that may be causing immunosuppression, such as malignant lymphosarcoma, malignant melanoma, hyperadrenocorticism, hypothyroidism, diabetes mellitus, etc. However, in many cases, an underlying immunosuppressive condition may not be found.
Localized demodicosis can generally be left untreated. The prognosis for this form is usually good, and spontaneous recovery is frequent. In contrast, treatment is required in cases of generalized demodicosis, for which prognosis has historically been guarded. Historically, whole-body amitraz dips (0.025%) applied every 2 weeks were the approved treatment in the US for generalized demodicosis. However, amitraz dips are no longer available, and although not currently FDA approved, alternative therapies are being used.
Other treatment protocols include the macrocyclic lactones, milbemycin oxime (0.5–1 mg/kg/day, PO), moxidectin, and ivermectin, and all have demonstrated varying degrees of effectiveness. Moxidectin is available as a spot-on formulation in combination with a flea product (imidacloprid) and should be given at 2.5 mg/kg at 1- to 4-week intervals. More frequent applications are associated with higher degrees of success. Other reportedly successful but unapproved systemic treatments include moxidectin (400 mcg/kg/day, PO) and ivermectin (300–600 mcg/kg/day, PO). For the latter, different therapeutic protocols have been proposed with a gradually increased dosage and close monitoring of treated animals to detect any potentially toxic effect. Ivermectin is contraindicated in Collies and Collie crosses. However, idiosyncratic toxicity may be seen in any breed. Testing for mutation in the MDR1 allele (ABCB1) may be required before initiating therapy.
More recently, systemic (topical or oral) isoxazolines have become the preferred treatment for both juvenile- and adult-onset generalized demodicosis. Although demodicosis is not an FDA-approved indication, the dose and administration frequency are the same as the labeled dosage for flea or tick control. Studies have demonstrated effectiveness when administered monthly (afoxolaner, lotilaner, or sarolaner) or once every 12 weeks (fluralaner). Studies indicate that adult-onset cases may take longer to completely resolve than juvenile-onset cases.
Local and systemic corticosteroids are contraindicated in any patient diagnosed with demodicosis. Secondary bacterial infections must be treated aggressively with an appropriate antimicrobial. Antiparasitic therapy must be continued not only until clinical signs abate but also until at least two consecutive negative skin scrapings are obtained at 1-month intervals. Although some dogs respond rapidly, others may need several months of treatment. Recurrence within the first year of treatment is not uncommon. As the sole prophylactic measure, dogs developing juvenile-onset generalized demodicosis should not be used for breeding. For dogs with adult-onset generalized demodicosis, an attempt should be made to find and treat the underlying immunosuppressive condition.
Feline Demodicosis
Feline demodicosis is an uncommon to rare skin disease caused by at least two species of demodectic mites. Demodex cati is thought to be a normal inhabitant of feline skin. It is a follicular mite, similar to but narrower than the canine mite, that can cause either localized or generalized demodicosis. One other species of Demodex (named D gatoi) is shorter, with a broad abdomen, and is found only in the stratum corneum. It causes a contagious, transmissible, superficial demodicosis that is frequently pruritic and can be generalized. In follicular localized demodicosis caused by D cati, there are one or several areas of focal alopecia most commonly on the head and neck. In generalized disease, alopecia, crusting, and potential secondary pyoderma of the whole body are seen. The generalized form is often associated with an underlying immunosuppressive or metabolic disease such as feline leukemia virus infection, feline immunodeficiency virus infection, diabetes mellitus, or neoplasia. In some cases, ceruminous otitis externa is the only clinical sign.
Diagnosis of feline demodicosis is made by superficial (D gatoi) and deep (D cati) skin scrapings, although mite numbers are often small, especially with D gatoi. Medical evaluation is indicated in cats with generalized disease. Dermatophyte cultures are essential, because dermatophytosis and demodicosis can be concomitant conditions. Prognosis of generalized demodicosis is unpredictable because of its potential relationship with systemic disease. Some cases spontaneously resolve. Weekly lime sulfur dips (2%) were the most common treatment and were considered safe and usually effective; however, the newer transdermal isoxazolines fluralaner and sarolaner-selamectin have demonstrated their effectiveness and are now the preferred treatments.
Trombiculosis in Cats and Dogs


Courtesy of Dr. Michael W. Dryden.
Trombiculosis is a common, seasonal, noncontagious acariasis caused by the parasitic larval stage of free-living mites of the family Trombiculidae (chiggers). It can affect domestic carnivores, other domestic or wild mammals, birds, reptiles, and humans. Two common species found in cats and dogs, Neotrombicula autumnalis and Eutrombicula alfreddugesi, are reported in Europe and in America, respectively. Adults (harvest mites) and nymphs look like small spiders and live on rotting detritus.
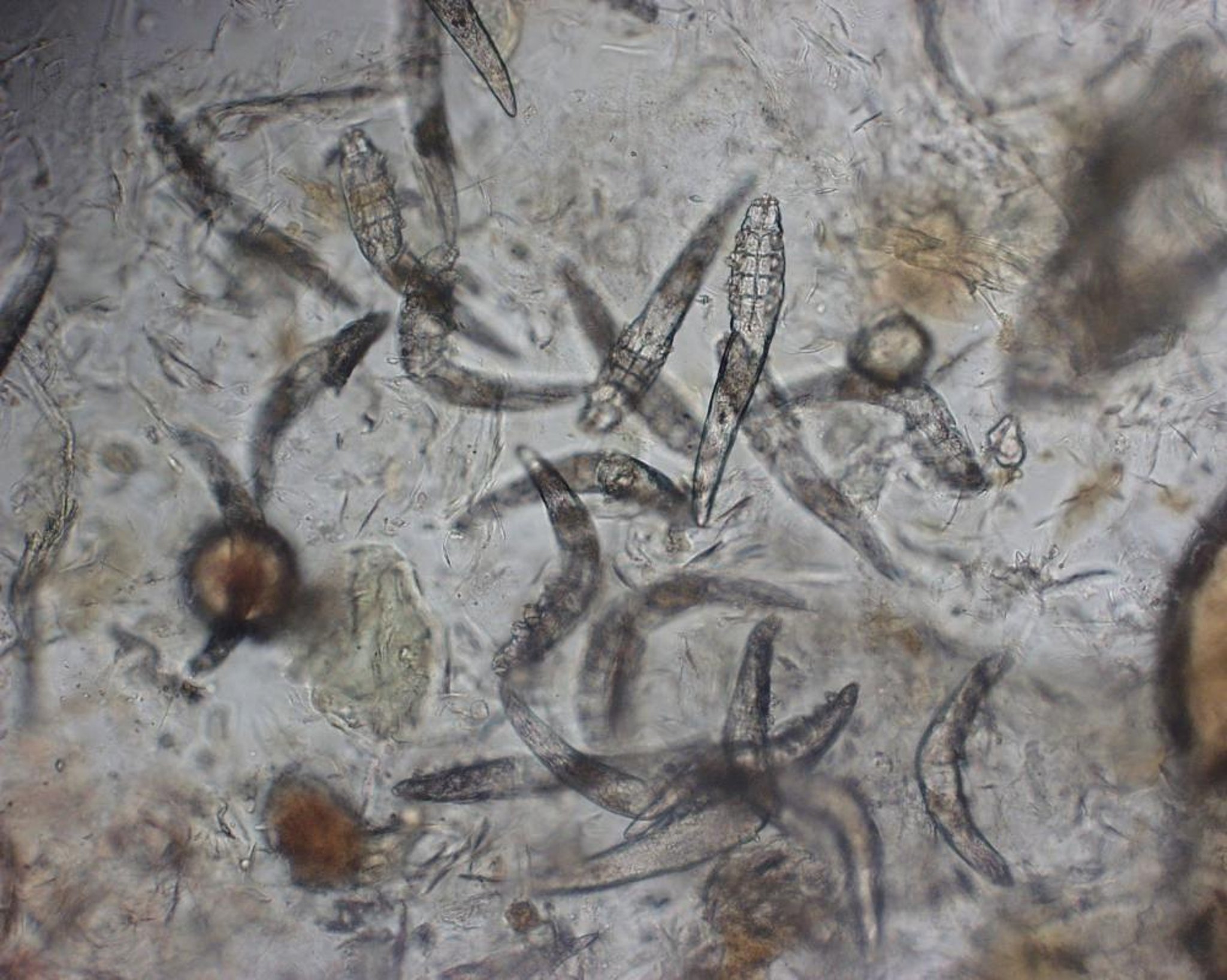
In temperate areas from summer to fall, dogs and cats can acquire the larvae as parasites when lying on the ground or walking outside. In warmer regions, infestation occurs throughout the year. The larvae (0.25 mm long) attach to the host, feed for a few days, and leave when engorged. At that time, they are easily identified as ovoid, 0.7 mm long, orange to red, immobile dots, usually found clustering on the head, ears, feet, or ventrum. Pathogenicity is through traumatic and proteolytic activities. Hypersensitivity reactions are suspected in some animals, because pruritus may vary from none to severe. Lesions include erythema, papules, excoriations, hair loss, and crusts. When present, intense pruritus can persist for hours to several days, even after the larvae have left the animal.
Diagnosis of trombiculosis is based on history and clinical signs. The infestation is a seasonal threat to free-ranging dogs and cats. Differential diagnoses include other pruritic dermatoses. Diagnosis is confirmed by careful examination of the affected areas. Microscopic examination of samples obtained from skin scrapings may help to identify the larvae, which have an oval-shaped body densely covered with setae, six long legs, and curved pedipalps terminating in claws.
Management is difficult. The most useful approach, if feasible, consists of keeping pets away from areas known to harbor large numbers of mites, to prevent reinfestation during periods of risk. The application of pyrethroids (dogs only) with repellent-like activity to prevent infestation has yielded variable results. Fipronil and permethrin (dogs only) can be used, both for prevention and treatment of infested animals. Symptomatic treatment may be required in cases of severe pruritus.
Straelensiosis in Dogs
Canine straelensiosis is a rare, noncontagious, sporadic, but potentially emerging parasitic dermatitis caused by the temporary encystment in the epidermis of the parasitic larval stage of Straelensia cynotis. This mite belongs to a family close to the family Trombiculidae. The life cycle is largely unknown, and the disease has been reported only in France, Portugal, Spain, and Italy. Transmission occurs mainly in rural and small-sized hunting dogs, probably through contact with contaminated soil, litter, and other terrestrial habitat of foxes. No contagion has been reported to congeners and humans. S cynotis has distinct differences from other trombidioid mites, especially in clinical presentation, histopathologic features, and response to treatment.
Straelensiosis is sudden in onset and may be accompanied by systemic clinical signs such as anorexia and prostration. Lesions are painful, variably pruritic, and either generalized or multifocal, most often affecting the dorsal regions of the head and trunk. The characteristic erythematous papules and nodules resemble small craters. Scaling, pustules, and crusts can be seen.
Differential diagnoses include bacterial folliculitis, sarcoptic mange, and gunshot. Microscopic examination of samples obtained from deep skin scrapings may help identify the larvae (0.7 mm long, 0.45 mm wide), each in a thick-walled cyst. The larvae, which resemble Neotrombicula, are more easily visualized by histopathology examination.
Prognosis is favorable; a self-cure generally occurs after several months if reinfestation is prevented. However, management of clinical signs is difficult. Ivermectin is usually effective.
Lynxacariasis in Cats
Feline lynxacariasis is a quite common but, to date, geographically restricted (Australia, Brazil, Hawaii, Florida, North Carolina, Texas) parasitic dermatitis caused by the fur mite Lynxacarus radovskyi, which belongs to the family Listrophoridae. The life cycle remains poorly described, and this species has not been reported from hosts other than cats. Infestation typically occurs by direct contact; however, fomites may be important for transmission. Clinical signs include a salt-and-pepper appearance of the hair coat, variable pruritus, and alopecia. Diagnosis is based on visualization of mites (0.5 mm long) using a magnifying glass or on isolation of any parasitic stage in skin scrapings or acetate tape preparations. Treatment with acaricidal sprays, weekly lime sulfur dips, and ivermectin (300 mcg/kg, SC) are effective. The only reported case of contagion to humans involved a transient rash in an owner with a heavily infested cat.






