



ECG Waveform Abnormalities in Dogs and Cats
Chamber enlargement can be indicated by waveform abnormalities in dogs and cats; however, these abnormalities are commonly absent when there is chamber enlargement and are sometimes present when the heart is normal. In lead II in dogs and cats, wide or notched P waves suggest left atrial enlargement, whereas tall P waves suggest right atrial enlargement. Tall R waves in leads that have the positive electrode on the left and/or caudal aspect of the body (leads I, II, aVF, CV6LL, and CV6LU) are evidence of left ventricular enlargement. Wide QRS complexes can occur in animals with either right or left ventricular enlargement; however, they can also be due to conduction disturbances. Electrocardiography is very insensitive at identifying mild to moderate changes in chamber size and unacceptably insensitive for detecting severe enlargement. Although false-positive findings are less frequent than false-negative findings, they do occur. Consequently, the level of accuracy is unacceptable, and ECGs should therefore not be used to infer chamber enlargement.
Sinus Rhythm and Sinus Node Abnormalities in Animals
The sinus node initiates depolarization of the rest of the heart in a healthy animal, sets the normal rate and rhythm, and is called the normal pacemaker of the heart. It functions as the pacemaker because it is automatic (depolarizes on its own) and does so at a rate faster than the other automatic sites in the heart (AV node and Purkinje fibers). Normal sinus rhythm is regular and originates at the sinus node, indicated on the ECG by a P wave that precedes each normal QRS complex. The rate at which the sinus node fires varies tremendously from species to species and situation to situation. A healthy dog can have a heart rate in the teens when asleep and ≥250 bpm during maximal exercise. A healthy but stressed cat can have a heart rate of 240 bpm at rest in an examination room.
Sinus bradycardia is a regular sinus rhythm that is slower than expected for a given species and for the situation the animal is in. Sinus bradycardia may be noted in animals overdosed with anesthetic drugs or agents that can result in increased vagal tone (primary or secondary) or decreased sympathetic tone (eg, xylazine, beta-blocker), as well as in hypothermic animals, hypothyroid animals, animals with sick sinus syndrome (see below), or animals with increased vagal tone secondary to systemic disease (such as respiratory, neurologic, ocular, GI, or urinary tract disease). Treatment for sinus bradycardia is typically not needed unless clinical signs associated with the bradycardia, such as exercise intolerance, weakness, or collapse, are noted. In dogs and cats, administration of atropine (up to 0.04 mg/kg, IV, IM, or SC) may be considered for treatment of bradycardia. The initiating cause should also be corrected.
Sinus tachycardia is the finding of a regular sinus rhythm at a rate faster than normal but generally appropriate for the situation the animal is in (eg, stress, exercise, heart failure). If the rate is inappropriately high (eg, 200 bpm in an otherwise healthy dog at rest at home), another form of tachycardia (eg, atrial or ventricular) should be considered. Causes include stress (resulting in high sympathetic drive), exercise, hyperthyroidism, fever, pain, hypovolemia, cardiac tamponade, heart failure, and administration of agents that can increase the rate of sinus node discharge (eg, catecholamines). Treatment is targeted at resolving the underlying cause. Administration of a beta-blocker (eg, atenolol) might be considered.
Sinus arrhythmia results from irregular discharge of the sinus node most commonly associated with the respiratory cycle. The site of impulse formation remains the sinus node; however, the frequency of the discharge varies. Sinus arrhythmia is a normal finding in dogs; it is abnormal in cats in the hospital setting, although it appears to be more common in cats in their home environment. Respiratory sinus arrhythmia is characterized by an increase in heart rate with inspiration and a decrease with expiration. In dogs, sinus arrhythmia can also occur without being in sync with respiration, and is instead associated with variation in the intensity of vagal tone. It is abolished by decreased vagal tone resulting from excitement, exercise, or administration of vagolytic drugs such as atropine. Sinus arrhythmia may be associated with a wandering pacemaker, which is characterized on the ECG by taller P waves during higher rates and smaller P waves during lower rates.
Sinoatrial (SA) block occurs when the impulse from the SA node fails to be conducted through the surrounding tissue to the atria and ventricles. Thus, no P waves or QRS complexes are noted on the ECG, and the P-P interval surrounding the break in sinus rhythm is an exact multiple of the normal P-P interval. Sinoatrial block is often difficult to diagnose in dogs because sinus arrhythmia is common, resulting in a variable normal P-P interval.

Courtesy of Dr. Mark D. Kittleson.
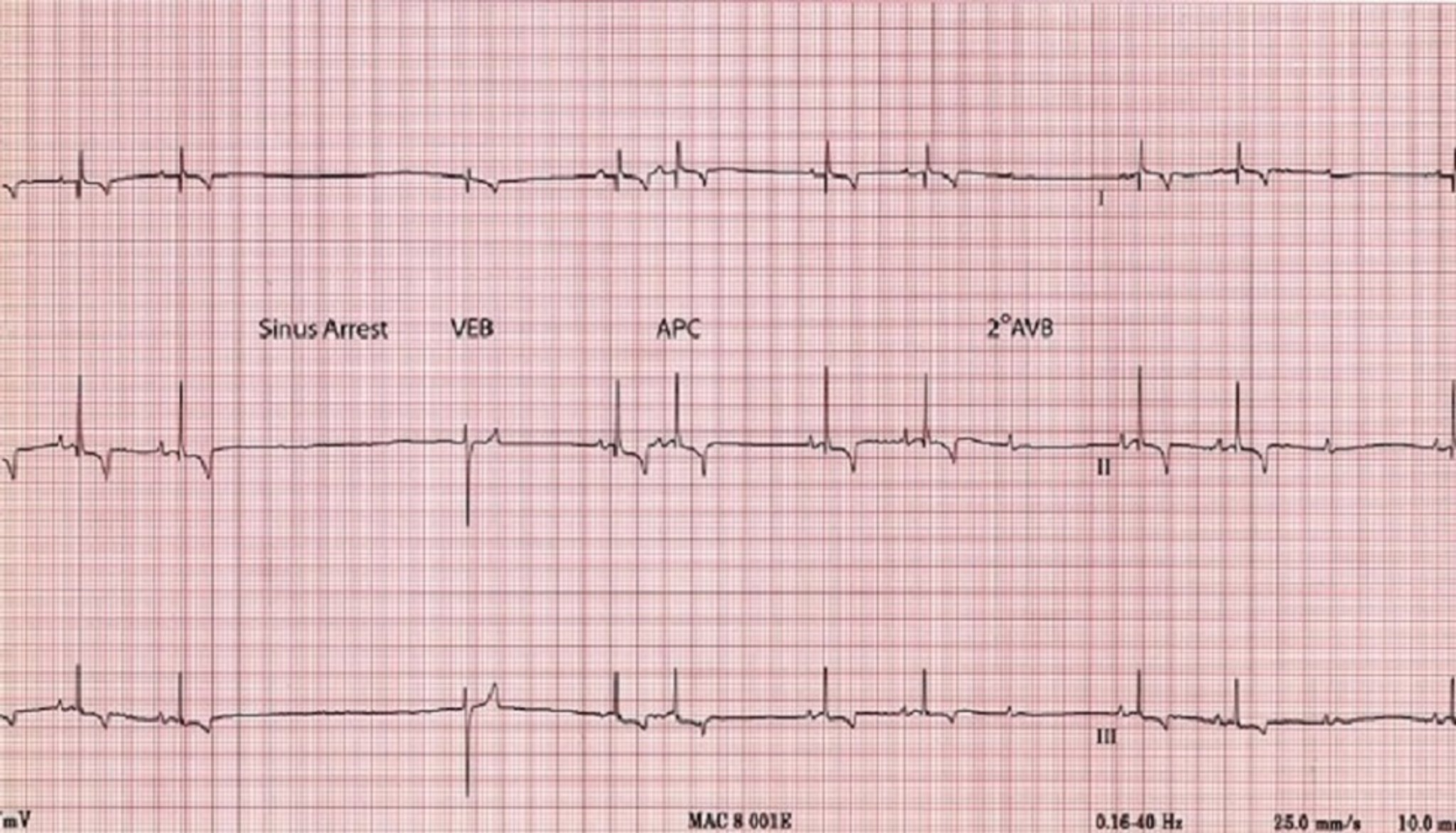
Sinus arrest (sinoatrial arrest, sinus pause) is the absence of P waves on the ECG for a short period (typically accepted as a pause exceeding twice the normal P-P interval). Sinus arrest results from excessive vagal tone, inherent sinus node disease, or both. Sinus arrest is usually due to some form of sick sinus syndrome (see below); however, it can sometimes occur with an exaggerated sinus arrhythmia.
Atrial standstill is characterized as the complete absence of P waves on the ECG and occurs when the atria are unable to be depolarized by the SA node discharge. Atrial standstill occurs either because the atrial myocardium is functionally unable to be depolarized (usually because of hyperkalemia), or because it has been destroyed by a cardiomyopathy or myocarditis (persistent atrial standstill). In hyperkalemia, the sinus node continues to depolarize, and the electrical tracts from the sinus node to the AV node (internodal tracts) continue to function, so the sinus node controls the rate (albeit at a lower rate). With persistent atrial standstill, the sinus node is destroyed, so the animal usually has an AV nodal (junctional) escape rhythm with a heart rate in the range of 40–65 bpm (dog).
Sick sinus syndrome is a constellation of abnormalities, including ECG changes (sinus arrest, junctional or ventricular escape complexes, and possibly supraventricular tachycardia) and possible weakness or syncope from the bradycardia (usual) or tachycardia (rare). With these clinical signs, the principal problem either lies within the SA node or perinodal tissue, or is due to increased vagal tone, or both. In some instances, other portions of the specialized conduction tissue of the myocardium, including the AV node, can also be affected. Therefore, evidence for AV block (see Atrioventricular Conduction Disturbances) may also be present. This condition is most commonly noted in geriatric dogs, particularly in Miniature Schnauzers and Cocker Spaniels. Administration of parasympatholytics (eg, propantheline bromide, 0.25–0.5 mg/kg, PO, every 8–12 hours) or sympathomimetics (eg, extended-release theophylline, 10 mg/kg/day, PO; terbutaline, 0.2 mg/kg, PO, every 8–12 hours ) to increase heart rate can be tried.(1) These are often effective; however, they may be effective for only a short time. Adverse effects can occur but are usually tolerable. Some dogs require pacemaker implantation.
References
Rishniw M, Thomas W. Bradyarrhythmias. In: Bonagura J, Kirk R, eds. Kirk’s current veterinary therapy: small animal practice. 13[ed.] ed. Philadelphia London: W.B. Saunders; 2000:719-725.
Atrioventricular Conduction Disturbances in Animals

Courtesy of Dr. Mark D. Kittleson.

Courtesy of Dr. Mark D. Kittleson.
The term atrioventricular (AV) block refers to an alteration of impulse conduction through the AV node from the atria to the ventricles. AV blocks are categorized as first-degree, second-degree, or third-degree blocks.
In first-degree AV block (prolonged conduction), the conduction time is increased and is recognized on an ECG as an increased P-R interval, with no attendant clinical signs
In second-degree AV block (intermittent conduction), occasional impulses fail to be conducted through the AV node, bundle of His, or both bundle branches; this type of block is most often characterized by occasional P waves that are not followed by QRS complexes. During the block, S1, S2, and arterial pulse are absent. S4 may be audible in dogs with second-degree AV block, but it is much less common to hear S4 in dogs. There are several different forms of second-degree AV block:
In Mobitz type I second-degree AV block, or Wenckebach phenomenon, the P-R intervals preceding the dropped beat progressively lengthen, or the P-R interval immediately after the block is shorter. This form of AV block is usually due to high vagal tone and is the most common type of second-degree AV block occurring in puppies. No treatment is indicated.
In Mobitz type II second-degree AV block, the P-R intervals do not change. Again, no treatment is indicated; however, closer surveillance may be warranted to see whether the block progresses to a more severe form.
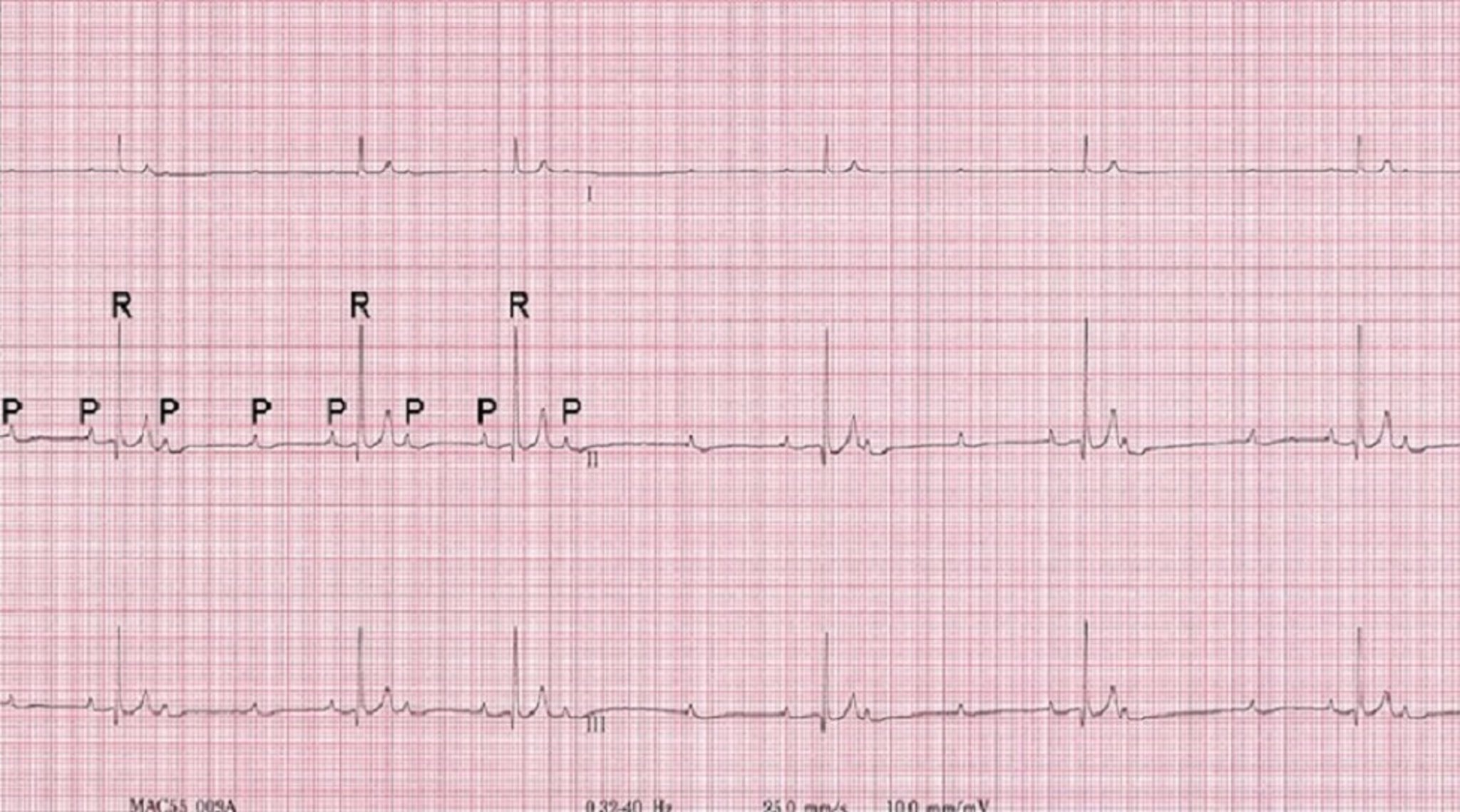
High-grade second-degree AV block occurs with every other beat in a ratio of 2:1 (two P waves for every QRS complex) or more (3:1, 4:1, etc). This type of AV block is distinguished from third-degree AV block (see below) by the presence of an association between the QRS complexes and the P wave preceding each one (same P-R interval for each). Dogs with high-grade second-degree AV block can have clinical signs that match those of dogs with third-degree AV block (eg, syncope), and they are also at increased risk of sudden death.
In third-degree AV block (complete heart block), none of the impulses are conducted from the atria to the ventricles. The atrial rhythm (P waves) occurs more rapidly and independently from the ventricular rhythm (QRS complexes)—a form of AV dissociation. The ventricular rhythm originates from subsidiary pacemakers (AV node in the case of nodal escape beats, ventricular Purkinje fibers in the case of ventricular escape beats). The heart and pulse rates are usually regular but slow and generally unresponsive to factors or agents that usually increase heart rate (eg, exercise, excitement, atropine). The difference in timing between atrial and ventricular contractions results in variation in ventricular filling and consequent variation in the intensity of S1 (bruit de canon) and possibly arterial pulse pressure. Periodically, the atria contract when the ventricle is in systole, resulting in a pulsation in the jugular vein (cannon A wave).
The importance of the type of AV block varies by species. Both first- and second-degree AV block may be present without outward evidence of cardiac disease. First-degree AV block may result from excessive vagal tone and usually is not important in dogs unless other evidence of heart disease or pathologic cause of increased vagal tone (eg, CNS or pulmonary disease) or AV nodal disease is present. In all species, second-degree AV block may indicate heart disease. Mobitz type II second-degree, high-grade second-degree, and third-degree (complete) AV blocks are always abnormal in all species.


Courtesy of Dr. Mark D. Kittleson.
Second- and third-degree AV blocks may be due to fibrosis, neoplasia, or injury to the AV node, or, rarely, to increased vagal tone or electrolyte abnormalities. The ideal treatment would be to correct the underlying cause, but this is not usually possible. High-grade second-degree AV block and third-degree AV block can cause exercise intolerance or, more commonly, weakness, collapse, and syncope. Oral treatment with positive chronotropic drugs, such as extended-release theophylline (10 mg/kg, PO, every 12 hours), terbutaline (0.2 mg/kg, PO, every 8–12 hours),(1) or propantheline bromide (0.25–0.5 mg/kg, PO, every 8–12 hours) may occasionally be useful in animals with second-degree AV block; however, more aggressive treatment (pacemaker implantation) is usually indicated in symptomatic (eg, syncopal) animals.
Third-degree heart block is usually associated with irreversible lesions; the only effective treatment in dogs is pacemaker implantation. Because they are at risk of sudden death, dogs with third-degree AV block should have a pacemaker implanted regardless of clinical signs. In cats, third-degree AV block often produces no clinical signs, and thus requires no treatment. However, problems can arise if such a block is not identified before anesthesia, and some cats will faint and thus require pacemaker implantation. Pacemakers have been implanted successfully in species other than dogs and cats, but only rarely.
References
Rishniw M, Thomas W. Bradyarrhythmias. In: Bonagura J, Kirk R, eds. Kirk’s current veterinary therapy: small animal practice. 13[ed.] ed. Philadelphia London: W.B. Saunders; 2000:719-725.
Common Tachyarrhythmias in Animals
Tachyarrhythmias can be categorized as supraventricular or ventricular on the basis of where they originate.Supraventricular premature complexes are premature complexes (as observed on an ECG) that originate from ectopic (nonautomatic) sites above the ventricles (eg, atrial myocardium or AV node). They may also be called atrial or nodal premature complexes/depolarizations/contractions/beats. Possible sites for ectopic depolarizations include the SA node (rare), atrial myocardium (very common), and AV node, or AV junction. On ECGs, supraventricular premature complexes are identified by a QRS complex that usually appears relatively normal but occurs earlier than the next expected normal QRS complex. Variable P wave morphologies may be noted before or after the supraventricular premature complex or may be hidden in the preceding sinus complex or within the premature complex. Supraventricular premature complexes are most commonly a result of atrial enlargement or disease, stress, or other causes of increased sympathetic tone.

Courtesy of Dr. Mark D. Kittleson.
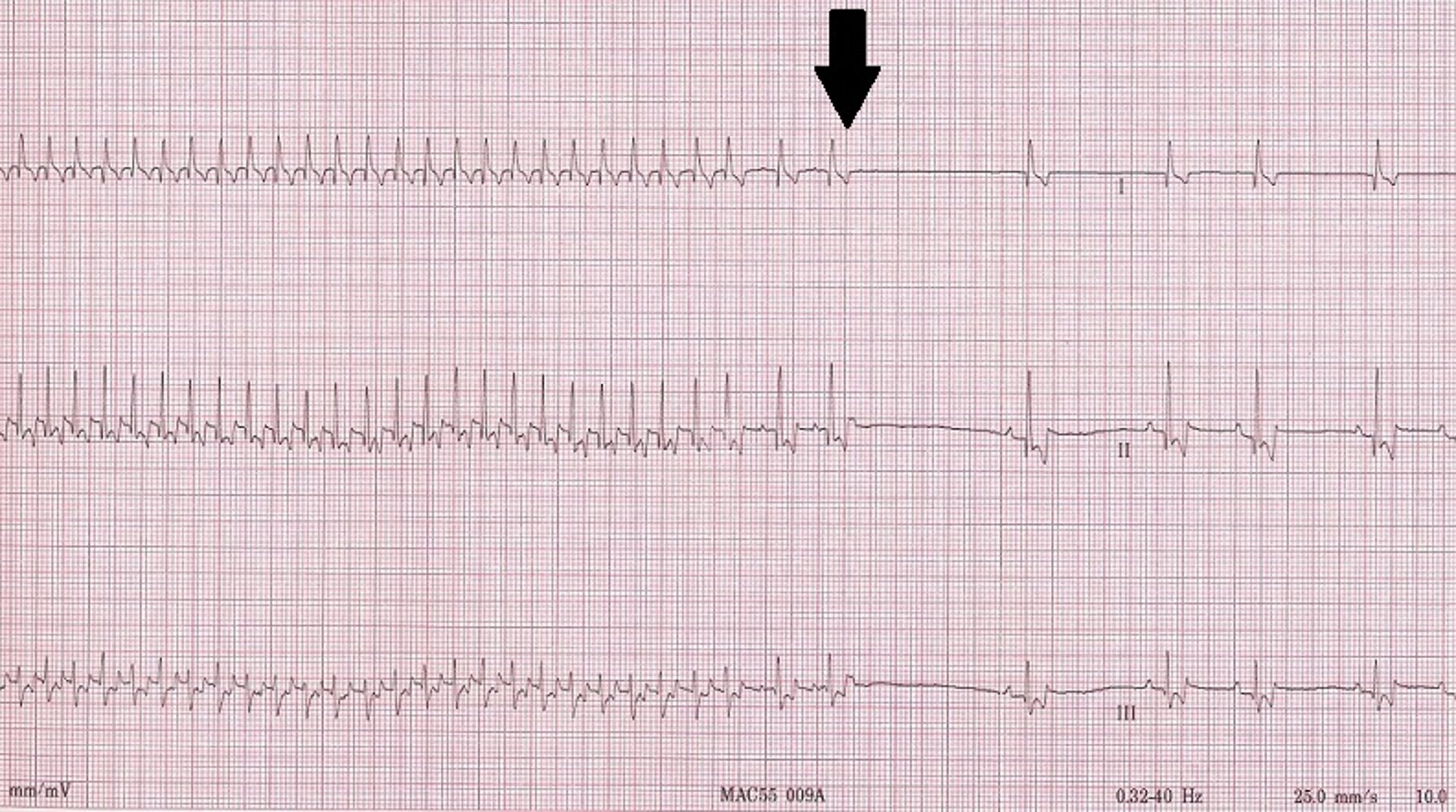
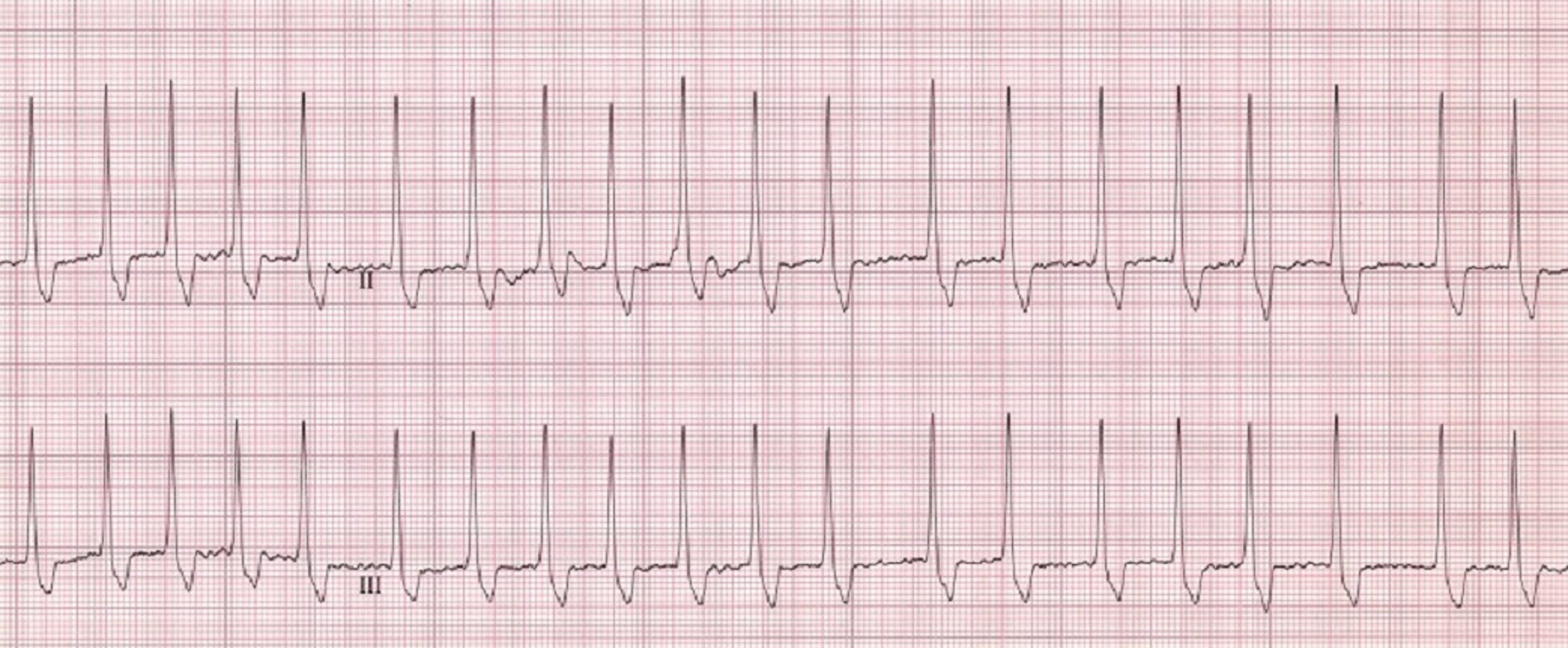
Supraventricular tachycardia (SVT) is the consecutive occurrence of a series of supraventricular premature complexes. SVT may be short (nonsustained) or occur for prolonged periods (called "sustained" when lasting > 30 seconds). SVT most commonly ranges in rate from 200 to 350 bpm in dogs. At rates closer to 200 bpm, it may be indistinguishable from sinus tachycardia on a surface ECG. Vagal maneuvers (applying ocular pressure, carotid sinus massage), precordial blow (chest thump), and intravenous administration of drugs (eg, diltiazem) often "break" an SVT into sinus rhythm and either do not change or more gradually slow a sinus tachycardia. Diltiazem (dogs, 0.5–2 mg/kg, PO, every 8 hours; cats, 1.5–3 mg/kg or 7.5–15 mg/cat, PO, every 8 hours) is the most common drug used in longterm treatment of SVT; however, it can also be used intravenously to break the SVT into sinus rhythm (0.1–0.25 mg/kg, IV bolus over 5 minutes, followed 15 minutes later by up to 0.35 mg/kg over 5 minutes or constant rate infusion at dose rate of 0.05–0.15 mg/kg per hour). Digoxin and beta-blockers are also used.
An accessory pathway (bypass tract) is a congenital abnormality that forms an electrical connection between an atrium and a ventricle outside the normal connection (AV node/bundle of His). Accessory pathways have been recognized in dogs and cats and may result in SVT (eg, orthodromic AV reciprocating tachycardia). Treatment may include radiofrequency catheter (heat) ablation of the bypass tract or, more commonly, administration of oral medications such as procainamide, sotalol, or diltiazem.

Courtesy of Dr. Mark D. Kittleson.

Courtesy of Dr. Mark D. Kittleson.
Atrial flutter is a rare arrhythmia that often progresses to atrial fibrillation. It is most commonly due to a reentrant loop within the atria and is typically characterized on the ECG by a “saw-toothed” baseline with relatively normal QRS complexes that can appear in a regular or irregular rhythm. The atrial rate of discharge is very rapid (> 400 bpm). Only intermittent atrial impulses are conducted through the AV node, because of its normal long refractory period, so the ventricular rate is slower than the atrial rate.
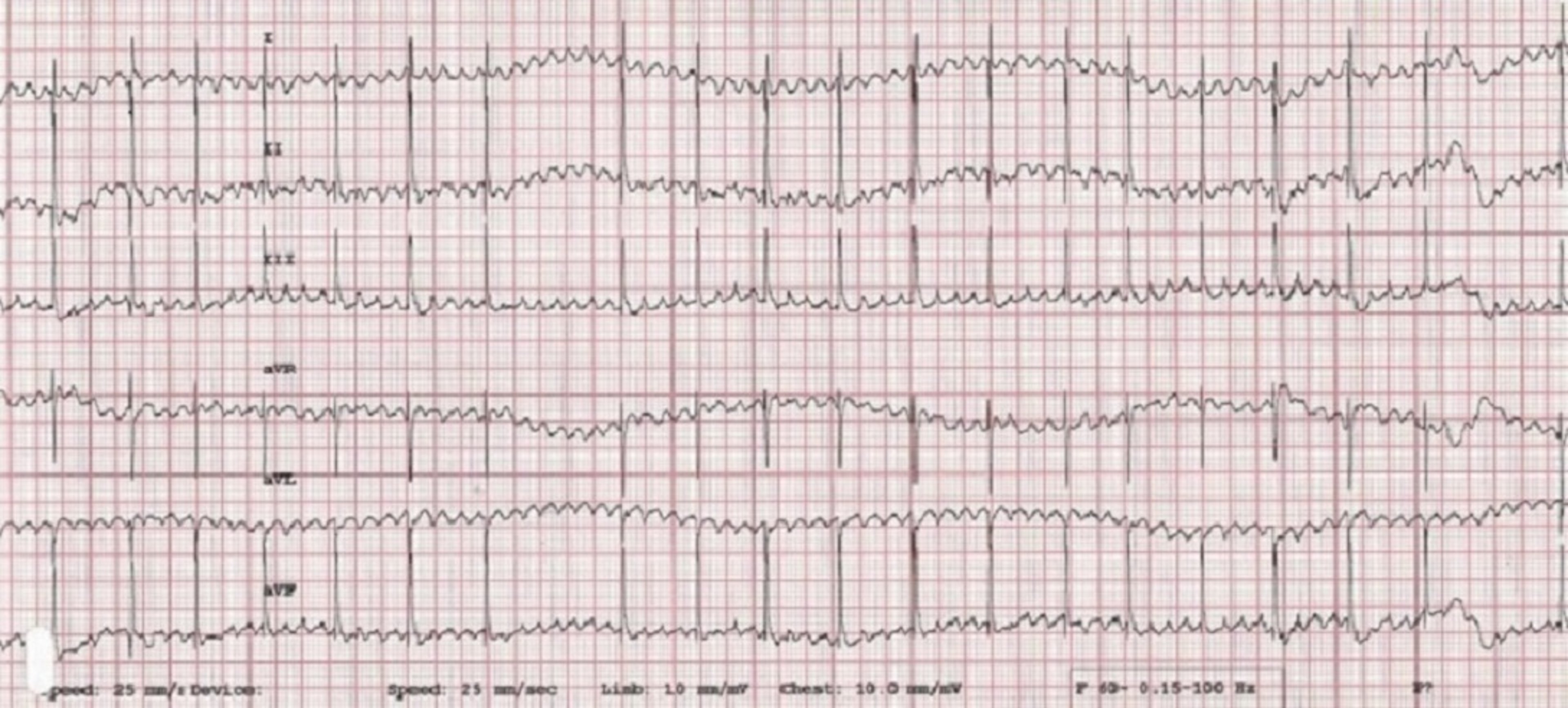
In dogs and cats, atrial fibrillation is an even more rapid atrial rhythm (> 600–700 atrial depolarizations/minute) that results in a slower (in the range of 80–300 bpm in dogs) and always irregular ventricular rhythm. As in atrial flutter, the AV node is bombarded by frequent atrial depolarizations. The AV node acts as a filter, allowing only some of the depolarizations to reach the ventricles, but always in an irregular fashion. In dogs and cats, atrial fibrillation is characterized on the ECG by normal-appearing QRS complexes with an irregular ventricular rhythm that is usually fast (> 160 bpm). After those characteristics are identified, the next thing to look for is the absence of P waves and an undulating baseline that can appear almost flat (fine) or very rough (coarse). The irregular rhythm results in variation in the diastolic filling period of the ventricles and thus variability in stroke volume and variability in pulse character, including pulse deficits. The irregular rhythm also causes variation in the intensity of the heart sounds, especially the second heart sound, creating a heart sound that resembles "tennis shoes in a dryer" on auscultation in dogs.
In dogs, atrial fibrillation is most commonly associated with underlying cardiac disease. The notable exception occurs in some giant dog breeds, such as Irish Wolfhounds, Scottish Deerhounds, Great Danes, and others, in which the rhythm can develop with an otherwise normal heart (so-called lone or primary atrial fibrillation). All cats in atrial fibrillation have severe underlying heart disease.
The goal of treatment of atrial fibrillation in most dogs and all cats is to control the ventricular rate—ie, the frequency with which QRS complexes are generated from the fibrillatory depolarization waves. Rate control is usually accomplished by administration of either diltiazem (Dogs: diltiazem immediate release [0.5–2.0 mg/kg, PO, every 8 hours] or diltiazem extended release (XR) [3–5 mg/kg, PO, every 12 hours,]; Cats: diltiazem immediate release [3.75–7.5 mg/cat, PO, every 8 hours], or diltiazem controlled delivery (CD) [30–45 mg/cat, PO, every 24 hours], or diltiazem extended release (XR) [30–60 mg/cat, PO, every 12 hours]) or a combination of digoxin (0.003 mg/kg, PO, every 12 hours) and diltiazem. The combination is often more effective than diltiazem alone. A beta-blocker, such as atenolol, may also be used, but never in combination with diltiazem. These drugs prolong the refractory period of the AV node and slow AV nodal conduction, resulting in fewer atrial depolarizations crossing the AV node to the ventricles. Amiodarone has also been used to control the ventricular response rate; however, its adverse effects (hepatic and thyroid toxicoses) limit its use to second-line treatment in animals refractory to the digoxin and diltiazem/atenolol protocol.
In rare instances, electrical cardioversion (defibrillation of the heart that is synced to the ECG to prevent causing ventricular fibrillation) is used to convert atrial fibrillation to sinus rhythm. This method is most sensible in a dog with primary atrial fibrillation; however, it has also been done in dogs with atrial fibrillation secondary to severe cardiac disease. In those instances, sinus rhythm commonly reverts back to atrial fibrillation within weeks to months, necessitating reconversion or rate control. Cardioversion is frequently combined with amiodarone administration in an attempt to prolong the time until reversion to atrial fibrillation.


Courtesy of Dr. Mark D. Kittleson.

Courtesy of Dr. Mark D. Kittleson.

Courtesy of Dr. Mark D. Kittleson.
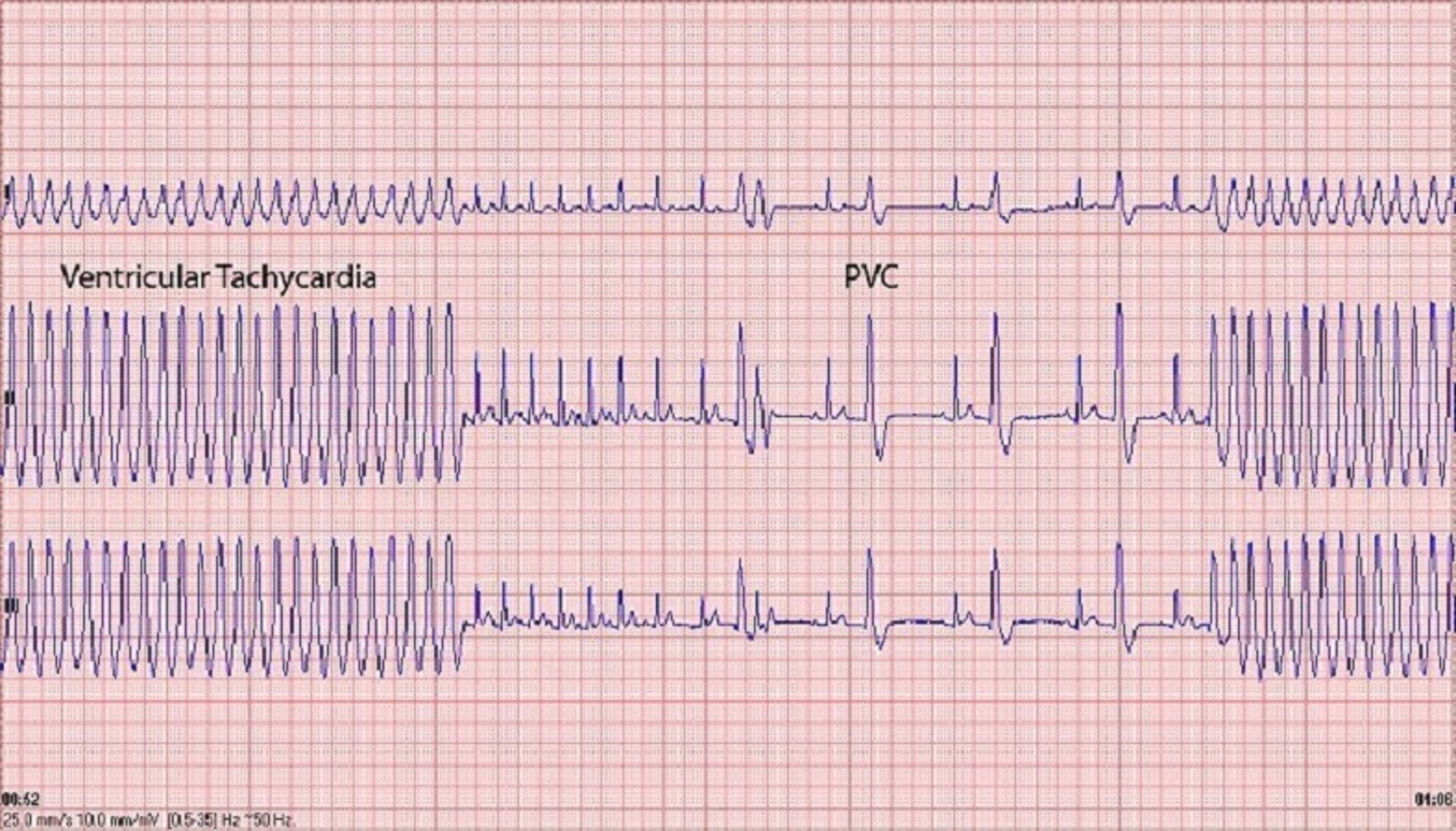
Ventricular premature complexes (VPCs) arise from a site within the ventricular myocardium or specialized intraventricular conduction system. On ECGs, the QRS complex usually appears wide and is followed by a large T wave that is opposite in polarity to the QRS complex. The result is a complex that is large and bizarre when compared with normally sinus-driven QRS complexes, occurs earlier than the next expected sinus-driven QRS complex (ie, it is premature), and does not have an associated preceding P wave, although unassociated P waves going at a lower rate (AV dissociation) may be observed. Most commonly, these complexes do not arise from primary cardiac disease, but instead result from systemic disturbances related to anesthesia, age, electrolyte abnormalities, acute toxicoses, neoplasia (eg, splenic hemangiosarcoma in dogs), gastric distention (eg, gastric dilation and volvulus syndrome in dogs), or trauma. They may also be associated with ventricular myocardial diseases such as dilated cardiomyopathy (DCM), arrhythmogenic right ventricular cardiomyopathy (ARVC; Boxer cardiomyopathy), and myocarditis.
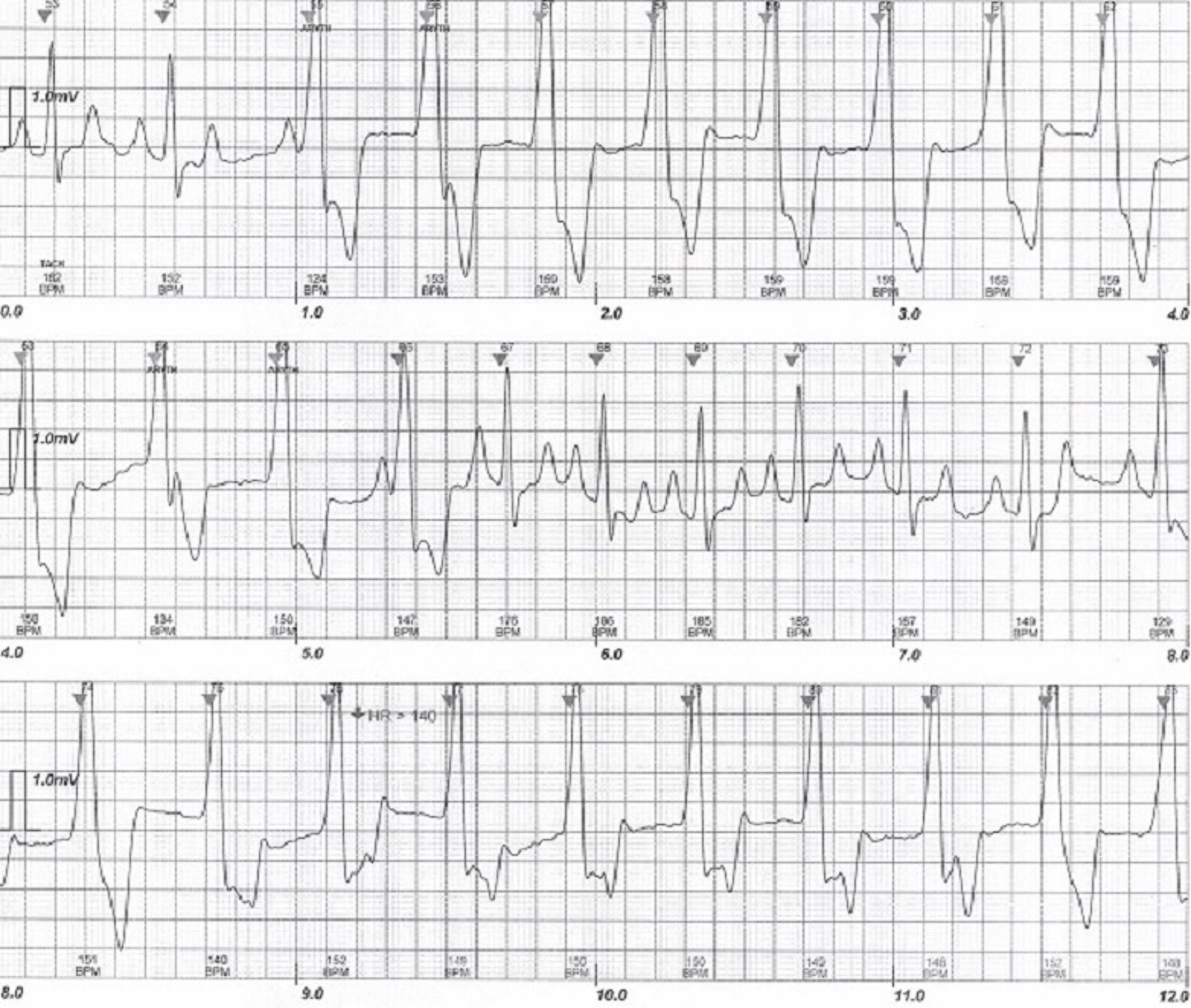
Ventricular tachycardia is the occurrence of three or more sequential ventricular premature complexes. Again, these can be nonsustained or sustained (> 30 seconds). They can also be divided into slower, benign ventricular tachycardias and faster, malignant ones. A slower, benign ventricular tachycardia is called an accelerated idioventricular rhythm (AIVR). AIVRs occur commonly in dogs in the intensive care unit secondary to systemic (often intra-abdominal) disease or trauma. AIVRs are characterized on ECGs by the presence of a ventricular tachycardia that is relatively slow (usually < 200 bpm). Sinus rhythm may be interspersed with the AIVR, with one rhythm taking control of the rhythm whenever it is slightly faster than the other.
Fusion beats(hybrids of sinus beats and premature ventricular contraction [PVC]) can also occur. This arrhythmia does not result in sudden death and usually dissipates on its own within 48–72 hours. Therefore, it requires treatment (eg, lidocaine) only if it is causing hemodynamic instability.

Courtesy of Dr. Mark D. Kittleson.
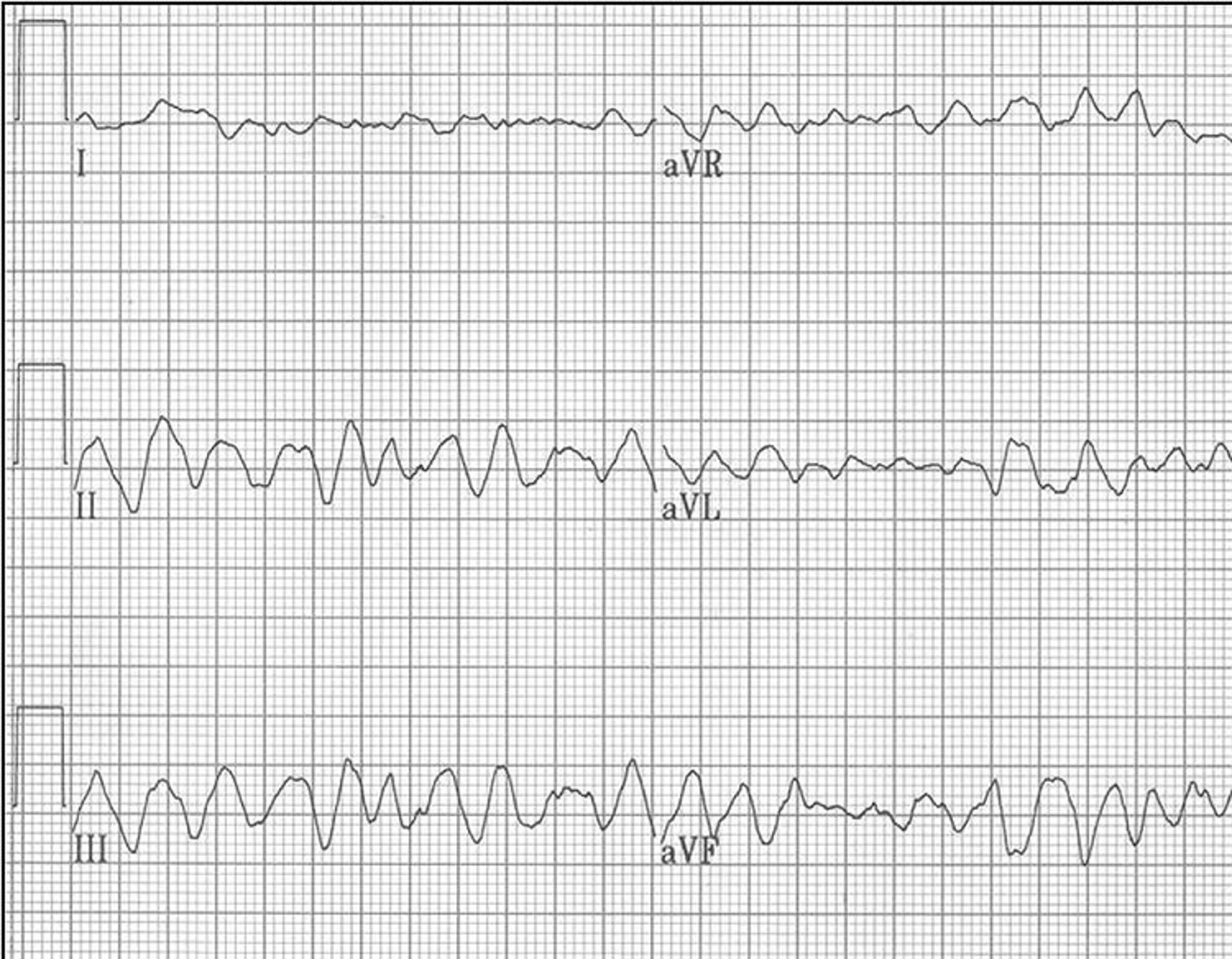
Malignant ventricular tachycardia is most commonly the result of severe underlying cardiac disease, usually either a cardiomyopathy (eg, DCM or arrhythmogenic right ventricular cardiomyopathy) or severe semilunar valve stenosis (eg, subaortic stenosis, pulmonic stenosis). Malignant ventricular tachycardia predisposes the animal to sudden death because the tachycardia can deteriorate into ventricular fibrillation. Frequently, this arrhythmia is not identified, so the first clinical sign observed is sudden death. Some dogs (especially Boxers and Doberman Pinschers) will experience syncope as the result of a very fast ventricular tachycardia (often > 400 bpm) that spontaneously reverts back to sinus rhythm within seconds of its onset (ventricular tachycardia by definition must last > 6 seconds and usually lasts no more than 1 minute).
Administration of sotalol or a combination of atenolol and mexiletine effectively controls the arrhythmia in Boxers and usually stops the syncope and presumably prevents sudden death. Beta-blockers are frequently administered to dogs with severe subaortic stenosis and to some with severe pulmonic stenosis in an attempt to prevent sudden death, but proof of efficacy is lacking. Ventricular tachycardia must be distinguished from ventricular escape rhythm, as observed with third-degree AV block, and from idioventricular rhythm, a terminal ventricular escape rhythm. A ventricular escape rhythm is a slow rhythm (20–40 bpm) that occurs because higher pacemakers (SA and AV nodes) have failed. Suppression of a ventricular escape rhythm by administration of a drug (eg, lidocaine) results in cessation of all cardiac electrical activity (ie, death).
Ventricular fibrillation is a result of microreentrant circuits within the ventricular myocardium, resulting in the absence of effective ventricular contractions; thus, it is a terminal rhythm (ie, cardiac arrest). The only effective treatment is electrical defibrillation.
Antiarrhythmics for Animals
A detailed discussion of antiarrhythmic treatment is covered elsewhere (see Antiarrhythmics in the chapter "Systemic Pharmacotherapeutics of the Cardiovascular System"). Most antiarrhythmic drugs are administered to suppress ectopic premature depolarizations (eg, atrial and ventricular premature complexes, atrial and ventricular tachycardia) or to slow the ventricular rate in animals with atrial flutter or fibrillation. Many antiarrhythmics are being supplanted by automatic implantable defibrillators in human medicine, so the manufacture of these drugs is waning. Some antiarrhythmics have negative inotropic effects, with the potential to worsen active CHF; this is most likely to occur with the use of beta-blockers in the treatment of supraventricular tachyarrhythmias and with sotalol.
Atrial fibrillation is one of the most commonly treated tachyarrhythmias; it is imperative to decrease the ventricular rate to ≤160 bpm if it is higher than that in the clinic. In experimental situations, pacing the heart of a dog at a rate ≥180 bpm results in myocardial failure severe enough to cause CHF within weeks. Consequently, leaving the rate this high will cause further cardiac disease and decompensation. The target heart rate is controversial, but an average (mean) heart rate of < 125 bpm on a Holter monitor (which provides a 24-hour ambulatory ECG) is a good target. Administration of diltiazem (Dogs: diltiazem immediate release [0.5–2.0 mg/kg, PO, every 8 hours] or diltiazem extended release (XR) [3–5 mg/kg, PO, every 12 hours,]; Cats: diltiazem immediate release [3.75–7.5 mg/cat, PO, every 8 hours], or diltiazem controlled delivery (CD) [30–45 mg/cat, PO, every 24 hours], or diltiazem extended release (XR) [30–60 mg/cat, PO, every 12 hours]) or a combination of diltiazem and digoxin (0.003 mg/kg, PO, every 12 hours) is generally the preferred method to control the ventricular rate in dogs with atrial fibrillation. A low dosage of a beta-blocker, such as atenolol (dogs: 0.2–1 mg/kg, PO, every 12–24 hours; cats: 2–3 mg/kg or 5–12.5 mg/cat, PO, every 12–24 hours), may also be used instead of diltiazem; however, the use of beta-blockers is uncommon. (Also see Antiarrhythmics).
Ventricular tachycardia can degenerate into ventricular fibrillation and cause sudden death. Dogs with fast ventricular tachycardia (> 250 bpm) or with ventricular tachycardia accompanied by severe underlying cardiac disease are the most vulnerable to dying suddenly from ventricular tachycardia. In Boxers with ARVC, administration of sotalol (0.5–3 mg/kg, PO, every 12 hours; most commonly 80 mg/dog, PO, every 12 hours) or of a combination of mexiletine (5–8 mg/kg, PO, every 8 hours) and either atenolol (0.5–1 mg/kg, PO, every 12 hours) or sotalol can effectively decrease or, more commonly, stop episodes of syncope due to ventricular tachycardia and decreases the incidence of sudden death. In addition, Doberman Pinschers with DCM commonly die suddenly as a result of ventricular tachycardia. Caution is warranted when treating patients with DCM with sotalol, as the negative inotropic effects of this drug can either push a dog into heart failure or make existing heart failure worse. Consequently, in these cases, the dosage must start low and be titrated upward carefully, with pimobendan administered concurrently. Amiodarone (loading dose: 8–10 mg/kg, PO, every 12 hours for 7–10 days; maintenance dose: 4–6 mg/kg, PO, every 24 hours) is another treatment option for preventing sudden death, but it has frequent adverse effects. Doberman Pinschers appear to be particularly susceptible to the hepatotoxic effects of amiodarone.
Animals with chronic bradyarrhythmias, as occur with AV block (high-grade second-degree block or third-degree block) or sick sinus syndrome, most commonly present with weakness, episodic weakness/collapse, and syncope. Pacemaker implantation is the treatment of choice. If pacemaker implantation is not a viable option, anticholinergics, phosphodiesterase (PDE) inhibitors, or sympathomimetics may be administered.
Propantheline is a mild anticholinergic dosed as follows: for dogs, 0.25–1 mg/kg, PO, every 8–12 hours; for cats, 0.8–1.6 mg/kg or 7.5 mg/cat, PO, every 8–12 hours for maximum 3 days. The parenteral formulation of atropine may be administered orally, but it must be diluted 10:1 with corn syrup at a dosage of 0.04 mg/kg, PO, every 6–8 hours. Adverse effects include mydriasis, dry mucous membranes, tachycardia, and GI stasis.
Theophylline is a nonselective PDE inhibitor with modest positive chronotropic effects. Extended-release tablets or capsules can be given at 10 mg/kg, PO, every 12 hours; consider monitoring. If no adverse effects are evident and the desired clinical effect is not achieved, the dosage in dogs can be increased to 15 mg/kg, PO, every 12 hours, while monitoring for adverse effects; and in cats, to 20 mg/kg, PO, every 24–48 hours. Adverse effects may include restlessness, excitability, tachycardia, or GI upset.
Terbutaline is a beta-agonist that has more potent positive chronotropic effects; however, its adverse effects are similar to those observed with theophylline. It is dosed to effect at 1.25–5 mg/dog (not per kg), PO, every 8 hours; and 0.625 mg/cat, PO, every 12 hours.
Oral treatment of clinically important bradyarrhythmias that are due to high-grade second-degree or third-degree AV block is often unsuccessful, although overall clinical signs may improve in some animals. Sick sinus syndrome is more often amenable to medical treatment.




