

Uroperitoneum is leakage of urine into the peritoneal space and is caused most often by rupture of the urinary bladder or urachus. Clinical signs, including lethargy, tachycardia, frequent attempts to urinate, and abdominal distention, appear shortly after birth. Diagnosis is based on history, clinical findings, laboratory tests, and ultrasonography. Surgical correction is typically successful in uncomplicated cases.
Uroperitoneum is defined as urine leakage into the peritoneal space. In foals, this most commonly results from tearing of the bladder or urachus during parturition, prolonged recumbency while being treated for a neonatal illness, or, less commonly, from rupture of the urachus secondary to umbilical abscessation. Ureteral tears are an uncommon cause of uroperitoneum.
In general, a higher incidence of bladder rupture is observed in males than in females, possibly because the narrower pelvis and the longer, narrower urethra of colts is a predisposing factor.
Traumatic bladder rupture is thought to be caused by uterine contractions on the foal's full bladder as the foal passes through the birth canal. Although most ruptured bladders at birth are thought to be traumatic, the presence of smooth edges and absence of hemorrhage around the tear in some foals might suggest a congenital origin (developmental defect of the bladder wall). Most bladder tears are located on the dorsum of the bladder.
In the case of a postnatal ruptured urachus, infection in the umbilical stump can weaken the urachal wall and result in leakage of urine into the abdomen or subcutaneously near the umbilicus.
Prematurity, neonatal encephalopathy, prolonged recumbency, cystitis, ascending infection, abdominal trauma, and sepsis can predispose foals to postnatal bladder rupture.
Clinical Findings of Uroperitoneum in Foals
Foals with uroperitoneum generally appear normal at birth but progressively become lethargic, tachycardic, and tachypneic throughout the 24–72 hours after the rupture. As the condition progresses, the abdomen becomes noticeably distended, and ballottement can produce a fluid wave. Most foals show pollakiuria and stranguria, with small amounts of urine being produced. This stranguria is often misinterpreted as straining to defecate (see image).


A 2-day-old Thoroughbred colt with a ruptured bladder and stranguria. The rear legs are extended behind the body, which is typical of stranguria, whereas in foals with meconium impaction and tenesmus, the rear legs are commonly placed underneath the body.
Courtesy of Dr. Thomas Divers.
Diagnosis of Uroperitoneum in Foals
History
Clinical findings
Laboratory tests and ultrasonography
Ultrasonographic abdominal examination and blood and peritoneal fluid analysis are crucial to confirming a diagnosis of uroperitoneum (see ). The combination of serum hyperkalemia with hyponatremia and hypochloremia is observed in most cases because of the high concentration of potassium and low concentrations of sodium and chloride in the urine, which rapidly equilibrate across the peritoneum into the plasma and other extracellular fluid sites.

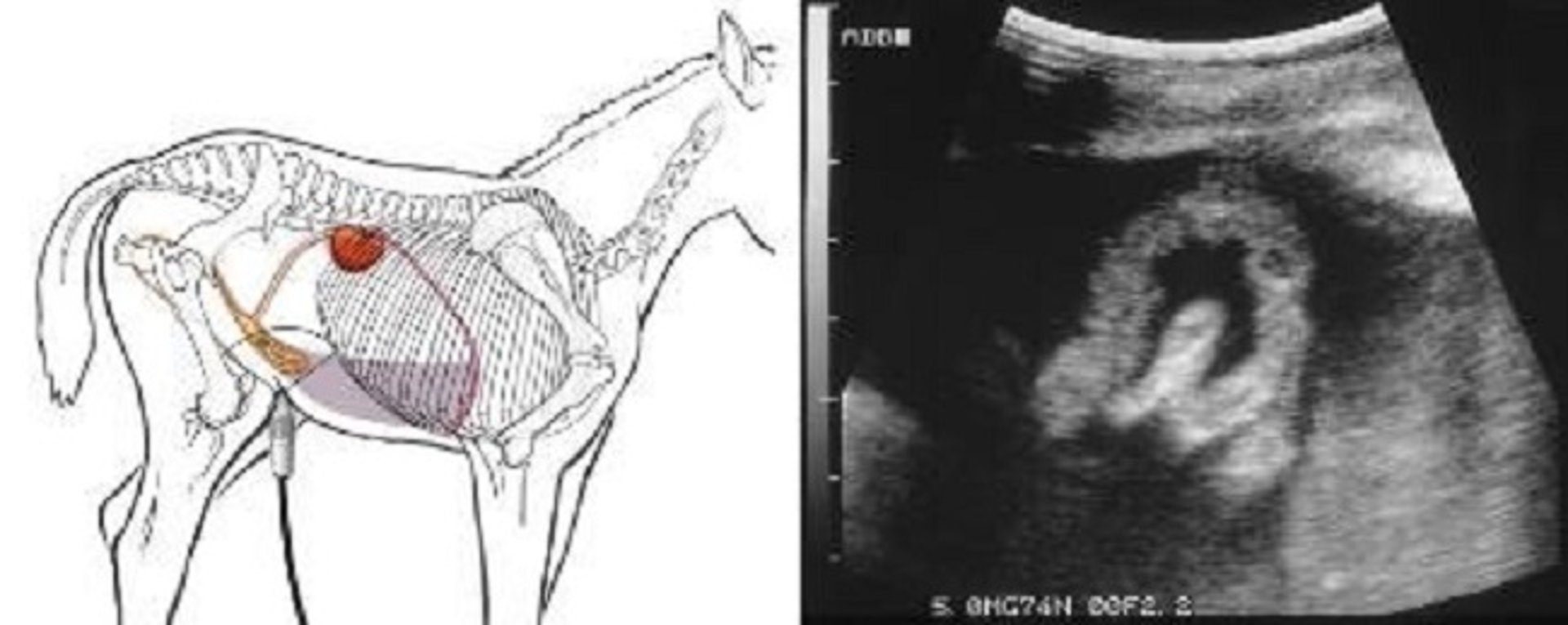
A drawing depicting an ultrasonographic examination of a foal with uroperitoneum along with an ultrasonogram of a ruptured bladder and uroperitoneum in a foal. The bladder is partially inverted due to the surrounding urine (black area) in the peritoneal space.
Courtesy of Dr. Thomas Divers.
Electrocardiography can show broad QRS complexes and very tall T waves due to hyperkalemia. The increased serum potassium concentration predisposes the foal to bradycardia and cardiac arrhythmias (atrioventricular block, atrial standstill, and cardiac arrest) if not corrected.
Azotemia (elevated serum BUN and creatinine concentrations) occurs in most cases. Blood gas analysis can also be normal or reveal metabolic acidosis. Abdominal fluid is pale yellow and copious and can easily be detected as hypoechoic-appearing fluid on ultrasonographic evaluation. The creatinine concentration in the peritoneal fluid is at least double that in the serum. This test is the most accurate in diagnosing the problem.
If laboratory testing is not available, 10 mL of 1% methylene blue can be injected into the bladder via a urinary catheter. If the bladder is patent to the peritoneal space, dye should be evident in the peritoneal fluid within 15 minutes. This test is rarely necessary to make the diagnosis and therefore rarely performed.
The clinical signs of progressive depression and stranguria can confuse the diagnosis with meconium impaction. Other differential diagnoses for uroperitoneum are listed in the table . Detrusor sphincter dyssynergia generally resolves within 2–4 days if a catheter is placed in the bladder to prevent rupture. This may be a form of neonatal encephalopathy.
Differential Diagnoses for Clinical Signs Associated With Uroperitoneum in Foals
Clinical Signs | Potential Diagnoses |
|---|---|
Progressive depression | Uroperitoneum, meconium impaction |
Progressive stranguria | Uroperitoneum, meconium impaction, detrusor sphincter dyssynergia |
Lethargy, tachycardia, tachypnea | Uroperitoneum, septicemia, hypoxic ischemic encephalopathy/neonatal encephalopathy, colic |
Hyponatremia, hypochloremia, azotemia | Uroperitoneum, acute renal failure, ureteral defects causing urine leakage, ureteral dilation caused by ureterovesical dysfunction |
In the case of a urachal rupture, abdominal ultrasonography can be helpful to establish an etiological diagnosis. Ultrasonography of the umbilical remnants may suggest the presence of infection or abscessation. A large amount of fluid in the abdomen is also observed if the urachal defect is within the abdomen. Subcutaneous urachal ruptures can also occur, causing an accumulation of urine in that area and marked stranguria.
Rarely, neonatal foals may become azotemic because of rupture of one or both ureters. With rupture of a ureter, accumulation of urine in the retroperitoneal area can be observed via ultrasonography until the retroperitoneal membrane ruptures, at which time the abdominal ultrasonographic findings and laboratory findings are identical to those with ruptured bladder.
Treatment of Uroperitoneum in Foals
Surgery
Surgery is necessary to correct the uroperitoneal defect and, in uncomplicated cases, is very successful. The foal should be stabilized with IV fluids and by having the urine drained from the peritoneal space when needed to correct electrolyte abnormalities, fluid deficits, and pressure on the diaphragm before surgery. In the author's clinical experience, potassium > 6 mEq/L should be lowered preoperatively by either 500 mL of isotonic sodium bicarbonate plus 10% dextrose given over 30–40 minutes, or sodium bicarbonate administration alone. All of these treatments help drive potassium into cells. If the potassium concentration is > 8 mEq/L or if the above treatments are unsuccessful, administration of regular insulin at 0.1–0.2 U/kg/h, IV, in 5% dextrose and saline solution (0.9% NaCl) and/or peritoneal fluid drainage should be considered.
The bladder should be repaired using absorbable sutures. If the tear is in the urachus, it is surgically removed. If the umbilical structures are enlarged (indicating infection), they should be removed at the time of surgery and cultured. After surgical correction of the ruptured bladder or urachal tear, an indwelling urinary catheter may be placed for 48 hours to decrease bladder distention and leakage of urine at the repair site; however, this is rarely done on a first repair. If the urachus is ruptured between the body wall and skin, causing subcutaneous accumulation of urine, placement of an indwelling urinary catheter can result in resolution of the problem without surgery.
If a bladder rupture is recognized early in an otherwise healthy foal and the foal is stabilized appropriately before surgery, the prognosis for recovery is excellent, with success rates as high as 95%. In septic or premature foals, in which complications such as peritonitis, incisional complications, adhesions, and anesthetic death are encountered more frequently, the prognosis is fair. All recumbent foals should be considered at high risk of bladder rupture and might require prophylactic indwelling catheterization.
Key Points
Ruptured bladder or urachus leading to uroperitoneum is common in neonatal foals.
The earlier that surgical correction can be performed, the less severe are plasma electrolyte abnormalities and volume of urine accumulating in the peritoneal space.
Sick neonatal foals that are persistently recumbent are also at risk of developing a ruptured bladder, and an indwelling urinary catheter might be needed to prevent this complication.
For More Information
Fubini SL, Delco M. Surgery of the equine urinary tract. Vet Clin North Am Equine Pract. 2022;38(1):141-153.
Schott HC, Waldridge B, Bayly WM. Disorders of the urinary system In: Reed SM, Bayly WM, Sellon DC, eds. Equine Internal Medicine. 4th ed. Elsevier; 2016:895-898,.
Also see pet owner content regarding uroperitoneum in foals.





