



Heart disease is defined as any functional, structural, or electrical abnormality of the heart. It encompasses a wide range of abnormalities, including congenital anomalies, as well as anatomical and physiologic disorders of varying causes. Heart disease can be classified by various characteristics, including presence at birth (eg, congenital or acquired), cause (eg, infectious, degenerative, genetic, or heritable), duration (eg, chronic or acute), clinical status (eg, left heart failure, right heart failure, or biventricular failure), anatomic malformation (eg, ventricular septal defect), or electrical disturbance (eg, atrial fibrillation, ventricular premature complexes).
The diagnosis of heart disease typically involves evaluating the signalment, history, and physical-examination findings, as well as results of diagnostic tests such as radiography, electrocardiography, and echocardiography. Rarely, more specialized tests, such as cardiac catheterization, CT, MRI, or nuclear studies, are necessary.
History and Signalment
For animals with suspected heart disease, the signalment (age, breed, sex) helps formulate a differential diagnosis list. The signalment influences the relative importance of possible heart diseases (eg, endocarditis is rare in cats and small dogs but more common in cows and large dogs), as well as many specific abnormalities (eg, breed predispositions for certain congenital defects, dilated cardiomyopathy [DCM], myxomatous valve degeneration, etc).
Animals presenting with heart disease often have no clinical signs. Animals in heart failure may have:
tachypnea
dyspnea
abdominal distention (ascites)
subcutaneous edema
weakness
syncope (fainting)
cyanosis
exercise intolerance
weight loss
Some findings are more common in some species, such as peripheral or ventral (subcutaneous) edema in horses and cattle in right heart failure, as opposed to ascites in dogs in right heart failure. Cats rarely cough with heart failure and more commonly present with a history of tachypnea/dyspnea (which may be subtle and go unnoticed by the owner) and anorexia. In dogs, coughing can be due to pulmonary edema; however, coughing in dogs is much more commonly due to lung disease (eg, chronic bronchitis). Therefore, extreme care must be taken when evaluating dogs (especially older, small-breed dogs) with a cough and a heart murmur, because many are not in heart failure.
Physical Examination
A complete physical examination should be performed on any animal that is being evaluated for heart disease or that presents with clinical signs possibly attributable to heart disease. The cardiac physical examination should start with auscultation of the heart. Auscultation should be done in as quiet an environment as possible. In all cats, small dogs, and small mammals, a pediatric stethoscope should be used. In addition, only the diaphragm of the stethoscope needs to be used, because heart sounds, including gallop sounds, in animals of this size are not low enough in frequency to require the bell. In large dogs and large animals, the bell should also be used. In general, the left apex beat should first be located by palpation, then the head of the stethoscope placed over it (mitral area). The stethoscope head then should be inched forward and upward to the left base (pulmonic and aortic area). In any young animal, care should also be taken to place the stethoscope head farther forward (left axillary region) to listen for a continuous murmur (patent ductus arteriosus). Then the right apical region should be auscultated. In a young animal suspected of having congenital heart disease, the right base and along the neck should also be auscultated.
In addition to auscultation of the thorax, palpation of the ventral thorax should be performed to assess for the presence of a thrill (vibration created by turbulent blood flow that can be palpated with the fingertips) and alterations in intensity or location of the apex beat. Concurrent auscultation and palpation of the pulse should also be performed to identify pulse deficits (premature beats, atrial fibrillation) and to assess the strength and character of the systemic arterial pulse.
Pulmonary auscultation should be performed (see Respiratory Sounds). Mucous membrane color and refill time should be assessed, but often they are normal even in animals with severe heart failure. Cyanosis may be present if the animal is severely hypoxemic. Limbs should be examined for the presence of edema, and the abdomen should be assessed for the presence of ascites (through palpation and ballottement). With the animal in a standing or sitting position, the jugular veins should be examined for the presence of abnormal distention and pulsation. A normal jugular vein will be distended and may pulsate when an animal is laterally recumbent.
Heart Sounds in Animals
Heart sounds are generated by the rapid acceleration and deceleration of blood and secondary vibrations in the cardiohemic system. Four heart sounds can potentially be auscultated:
First heart sound (S1): closure of the atrioventricular (AV) valves (mitral and tricuspid valves) at the onset of systole
Second heart sound (S2: closure of the semilunar valves (aortic and pulmonic valves) at the end of systole
Third heart sound (S3): vibration of the ventricles during diastole, specifically during rapid ventricular filling (E wave on an echocardiogram)
Fourth heart sound (S4): vibration of the ventricles during late diastole, or atrial systole
In dogs, cats, and ferrets, S1 and S2 are the only heart sounds normally audible.
Three-Heart-Sound Rhythms (Gallop Heart Sounds and Systolic Clicks)
A gallop heart sound (rhythm) is the presence of S1 and S2 accompanied by an interceding sound or sounds in diastole (between S2 and S1) that is either an accentuated third heart sound (S3) or fourth heart sound (S4), or both. Gallop heart sounds are classified as protodiastolic (S3), presystolic (S4), or summation (fusion of S3 and S4). The most common gallop heart sound noted in dogs is a result of an accentuated S3 and typically occurs secondary to a normal quantity of blood "dumping" into a stiff left ventricle (as in DCM), or a massive amount of blood "dumping" into a normal left ventricle in early diastole (as in mitral regurgitation and patent ductus arteriosis). An S4 gallop heart sound is due to the action of atrial contraction pushing blood into a stiff left ventricle. In cats with cardiomyopathy, especially hypertrophic cardiomyopathy, the left ventricle is stiff, so both third and fourth heart sounds can be heard. However, because the heart rate commonly exceeds 160–180 bpm in cats in an examination room, it is usually impossible via auscultation to determine whether the gallop sound is due to an S3 or an S4 gallop; often, it is a summation of the two.
Gallop rhythms are not the only three-heart-sound rhythms that can be auscultated. Systolic clicks also occur in dogs and cats, and they are much more common than gallop rhythms in dogs. A systolic click is a short, sharp sound that occurs during mid to late systole. In dogs, systolic clicks occur mostly in middle-aged to older small breeds, and they are thought to be evidence of early myxomatous AV valve degeneration, causing mitral valve prolapse (as they are in humans). A systolic murmur may or may not also be present. Although systolic clicks are reasonably easy to distinguish from a gallop sound in dogs (they are usually relatively loud and high pitched, whereas a gallop sound is soft and low pitched), in cats they often sound identical to a gallop sound. Thoracic radiographs can be used to help distinguish between the two. In cats, gallop sounds are heard when severe heart disease is present. Systolic clicks are usually heard in cats that have an otherwise normal heart. So, if the heart is not enlarged, the sound is more likely a systolic click. Systolic clicks usually are single; however, they may be multiple, and they can vary in intensity (even completely disappearing), depending on cardiac loading conditions. Rarely, a three-heart-sound rhythm is a bigeminal rhythm (in which every other beat is premature).
Splitting of S or S
Split heart sounds are rare, subtle, and seldom clinically noteworthy in small animals. Splitting of S1 is due to discordant closure of the mitral and tricuspid valves, which can occur when there is asynchronous contraction of the ventricles, as in left or right bundle-branch block, cardiac pacing, and ectopic premature ventricular beats. S1 can also be split in healthy, large-breed dogs and in large animals.
Delayed closure of the pulmonic valve (in relation to the aortic valve) results in splitting of S2. Splitting of S2 can be a normal finding in horses during respiration. Abnormal splitting of S2 has been associated with pulmonary hypertension, as in pulmonary emphysema in horses and severe heartworm disease in dogs. Other possible causes include a large atrial septal defect, right bundle-branch block, or premature ventricular ectopic beats of left ventricular origin. Delayed closure of the aortic valve (paradoxical splitting of S2) might be heard with left bundle-branch block or premature ventricular ectopic beats of right ventricular origin. It has never been described in small animals. A split S2 is a subtle finding that usually must be heard several times along with a mentor before it can be appreciated.
Heart Murmurs in Animals
Heart murmurs are audible vibrations (sound) emanating from the heart or major blood vessels. The vast majority are due to turbulence created by high-velocity blood flow that produces a mixed-frequency murmur. Much less commonly, murmurs are due to vibrations of cardiac structures such as part of a valve leaflet or chordal structure that produces a single frequency (musical) murmur. Murmurs are typically defined relative to timing (systole, diastole, continuous); intensity (grades 1–6); and location (eg, left apex, left base). They can also be characterized by frequency (pitch); quality (eg, musical); and configuration (eg, crescendo-decrescendo).

Courtesy of Dr. Mark D. Kittleson.
A systolic murmur is typically described as either ejection (crescendo-decrescendo) or regurgitant (holosystolic, plateau). However, making this distinction is often difficult, even for an experienced examiner, especially when the heart rate is fast. Ejection-quality systolic murmurs typically demonstrate the greatest intensity during mid systole and appear diamond shaped on phonocardiography. Systolic murmurs are most commonly produced by stenotic lesions at the semilunar valves (eg, pulmonic stenosis or subaortic stenosis). A classic regurgitant systolic murmur demonstrates a constant intensity throughout systole and is commonly due to mitral or tricuspid regurgitation (eg, myxomatous degeneration of the mitral valve) or a ventricular septal defect. However, these murmurs may also change intensity during systole.
Diastolic murmurs are typically decrescendo (decreasing in intensity through diastole) and usually the result of aortic insufficiency (such as the insufficiency due to aortic valve infectious endocarditis in dogs or degenerative disease in horses). Diastolic murmurs may sound like a dive-bomber or grunting.
A continuous murmur is most commonly the result of patent ductus arteriosus and occurs throughout systole and diastole. A continuous murmur varies in intensity over time, typically being most intense at the end of ventricular ejection (the second heart sound) and then decreasing in intensity through diastole. The term "to-and-fro murmur" describes a murmur that occurs both in systole and in diastole (eg, in an animal with subaortic stenosis and aortic insufficiency).
In horses, early systolic and diastolic murmurs can be noted in the absence of heart disease or anemia. The point of maximal intensity is typically located over the left heart base. A short, high-pitched, squeaking, early diastolic cardiac murmur is sometimes heard in healthy, young horses. In cats, systolic heart murmurs are often heard without cardiac disease. Some of these systolic murmurs are due to an increase in right outflow tract flow velocity (dynamic right ventricular outflow tract obstruction). Innocent cardiac murmurs are also sometimes noted in immature cats and dogs (< 3 months old) and may be the result of a relative increase in stroke volume (stroke volume/aortic cross-sectional area).
Heart murmur intensity is classified as follows:
Grade 1: the lowest-intensity murmur that can be heard, typically detected only when auscultation is performed in a quiet room
Grade 2: a faint murmur but easily audible, and restricted to a localized area
Grade 3: a murmur immediately audible when auscultation begins in the correct location
Grade 4: a loud murmur immediately heard at the beginning of auscultation but not accompanied by a thrill
Grade 5: a very loud murmur with a palpable thrill
Grade 6: an extremely loud murmur with a thrill that can be heard when the stethoscope is removed from the chest wall
A soft systolic heart murmur (grades 1 and 2) usually either is not due to heart disease or is due to mild heart disease. An exception would be a large atrial septal defect. A very loud systolic heart murmur is commonly associated with severe heart disease (eg, severe subaortic stenosis in dogs almost always creates a loud systolic heart murmur), but that is not always the case. For example, a small ventricular septal defect usually produces a loud systolic heart murmur on the right side of the chest, and even some dogs with mild mitral regurgitation have a loud heart murmur. Grades 3 and 4 heart murmurs are generally not predictive of heart disease severity.
Grading murmur severity is subjective and the differences between grades 1 and 2, grades 3 and 4, and grades 5 and 6 are difficult to discern, vary from individual to individual, and provide no useful information. Consequently, it may be better to describe them as soft, moderately loud to loud, and palpable.
Arrhythmias in Animals
Arrhythmias (also called dysrhythmias or ectopic rhythms) are abnormalities of the rate, regularity, or site of cardiac impulse formation and are noted during auscultation. The presence of a cardiac arrhythmia does not necessarily indicate the presence of heart disease; some arrhythmias are normal, such as sinus arrhythmia in a dog and second-degree AV block in a horse; many cardiac arrhythmias are not clinically important and require no specific treatment. Some arrhythmias, however, may cause severe clinical signs, such as syncope, or lead to sudden death. Numerous systemic disorders may be associated with abnormal cardiac rhythms. Common auscultatory findings in animals with an arrhythmia are a rate that is too slow (bradycardia), a rate that is too fast (tachycardia), premature beats (a beat is heard too early), an irregular rhythm, and pauses in the rhythm. Whenever an abnormal rhythm is heard, an electrocardiogram (ECG) should be performed.
Pulses in Animals
The arterial pulse is the rhythmic expansion of an artery by blood flow/pressure that can be digitally palpated (or visualized) during physical examination. Physiologically, the pulse pressure (the pulse one feels) is the systolic pressure minus the diastolic pressure. The best place to feel the arterial pulse depends on the species;.in dogs and cats the arterial pulse is typically palpated at the femoral artery, whereas in horses, the facial artery is usually used. To feel the maximum pulse, examiners should first occlude the artery with their fingers and then gradually decrease the digital pressure until the maximum pulse is felt.
A weak pulse (a decrease in pulse pressure) is usually due to a decrease in systolic pressure and can be noted with decreased stroke volume in animals in heart failure, hypovolemic shock, or cardiac tamponade, as well as those with severe subaortic stenosis. However, a weak pulse can also be felt in a healthy animal if the artery is not palpated appropriately or in an obese or heavily muscled animal. A bounding pulse (an increase in pulse pressure) is usually caused primarily by a decreased diastolic pressure and can be noted with aortic insufficiency and patent ductus arteriosus. However, the pulse in a thin, athletic dog may also feel stronger than expected. The pulse felt with mitral regurgitation is often normal but at times may be termed "brisk."
A pulse deficit is an absent pulse despite auscultation of a heartbeat and is thus detected during simultaneous auscultation and pulse palpation. Pulse deficits are often due to a premature beat that occurs so early that the ventricles are unable to fill sufficiently, resulting in a decreased stroke volume that produces either a weak pulse or no pulse. Atrial fibrillation also produces pulse deficits, as well as alternating pulse strength.
Dogs with severe subaortic stenosis may have a pulse pressure that slowly increases during ventricular systole and reaches a peak pressure late in systole called pulsus parvus et tardus. Pulsus paradoxus is a decrease in pulse pressure during inspiration and an increase in pulse pressure during expiration. Pulsus paradoxus occurs normally in animals, but it is too subtle to observe on physical examination. Animals with cardiac tamponade (severe pericardial effusion), however, demonstrate an exaggeration of this finding, so it becomes detectable. Pulsus alternans is an alternating strong and weak pulse while the animal is in sinus rhythm; it can be noted (albeit rarely) in animals with severe (usually terminal) myocardial failure or tachyarrhythmias. Pulsus bigeminus is an alternating strong and weak pulse due to an arrhythmia such as ventricular bigeminy. The weaker pulse (during the ventricular premature contraction) typically follows a shorter time interval than the stronger pulse.
Jugular venous pulsation can be noted in normal animals but typically does not extend beyond the thoracic inlet.
Respiratory Sounds in Animals
Pulmonary edema may develop as a result of congestive heart failure (CHF). Animals with pulmonary edema will be hyperpneic (have an increased respiratory rate [tachypnea] and depth of respiration) and may be dyspneic. The increased depth of respiration may increase bronchovesicular sounds. Fine and, less commonly, coarse crackles might be auscultated in animals with pulmonary edema; however, fine crackles are usually heard only at the end of a deep inspiration. Coarse crackles in dogs are most commonly heard with chronic bronchitis. Pulmonary edema is often silent (no auscultatory abnormality). Respiratory sounds may be absent in animals with pleural effusion, especially ventrally.
Ascites in Animals
Abdominal distention may occur as a result of gas, soft tissue, or fluid accumulation. Animals with right heart failure (eg, due to severe heartworm disease, severe tricuspid valve dysplasia, cardiac tamponade) can develop ascites. Because there are many causes of ascites, it is important to evaluate the jugular veins in every case in which ascites is present. If right heart failure is the cause of the ascites, the jugular veins may be distended (but often they are not distended in dogs and cats) by the increase in right atrial pressure. If the jugular veins are not distended in a dog or cat with ascites, a hepatojugular reflux test should be performed. To do this, one person examines the jugular veins with the animal standing or sitting, while another person places firm and steady pressure on the abdomen. In a dog or cat in right heart failure, the jugular veins should distend well up the neck with this maneuver. If ascites is present without jugular venous distention and with a negative hepatojugular reflux test, then extracardiac causes of the ascites should be considered.
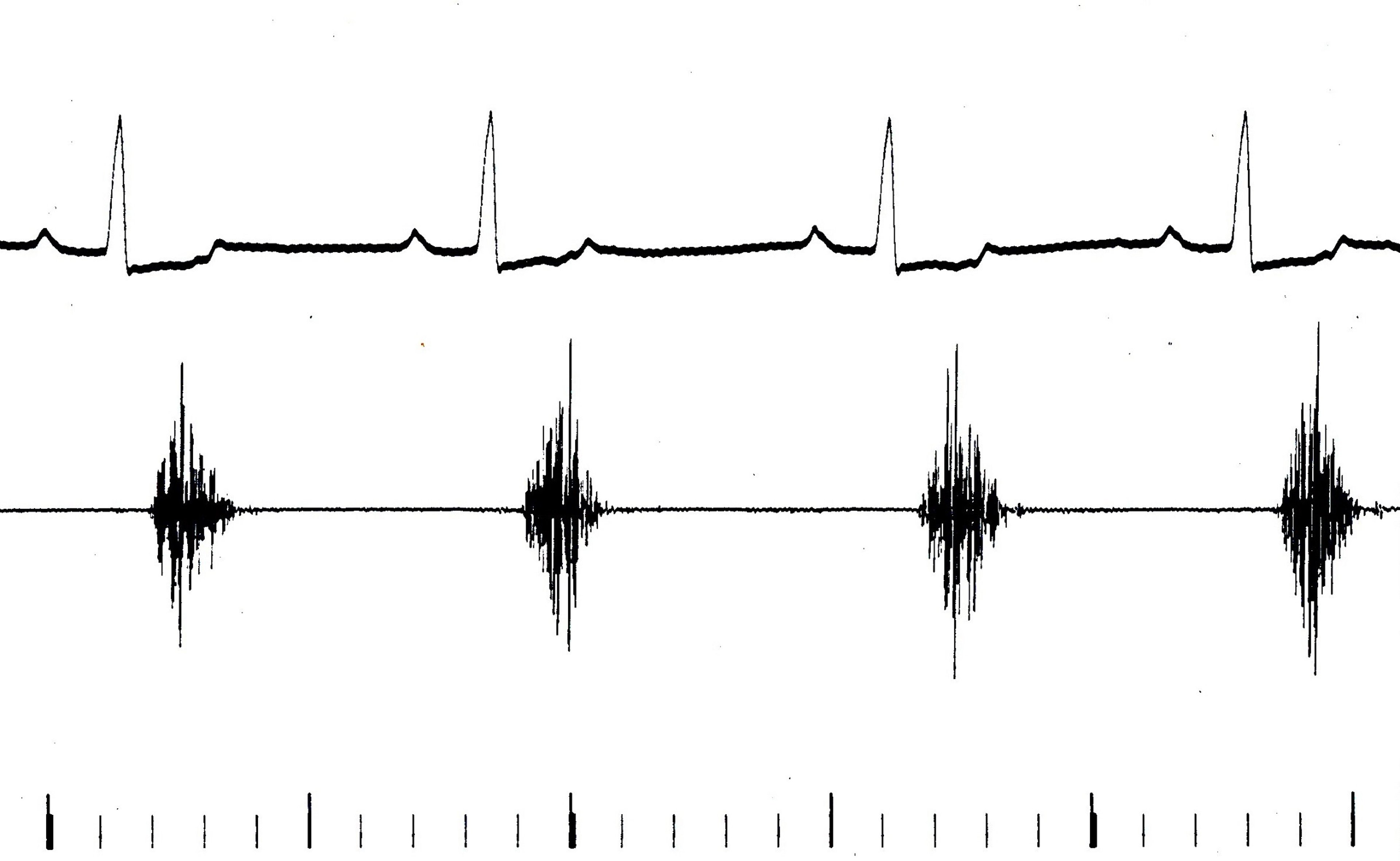
Synchronous Diaphragmatic Flutter in Animals
The diaphragm may contract synchronously with the heart to produce loud thumping noises on auscultation and usually visible contraction in the flank area. The syndrome results from stimulation of the phrenic nerve by atrial depolarization and occurs primarily when there is a marked electrolyte or acid-base imbalance, particularly with hypocalcemia. Synchronous diaphragmatic flutter is most common in horses and dogs. In dogs it occurs most commonly in association with hypocalcemia and electrolyte disturbances induced by GI disease, although idiopathic cases also occur. Similarly, in horses it occurs with hypocalcemia, and in endurance horses it accompanies dehydration and electrolyte depletion.
Radiography


Courtesy of Dr. Mark D. Kittleson.


Courtesy of Dr. Mark D. Kittleson.


Courtesy of Dr. Mark D. Kittleson.


Courtesy of Dr. Mark D. Kittleson.

Courtesy of Dr. Mark D. Kittleson.


Courtesy of Dr. Mark D. Kittleson.
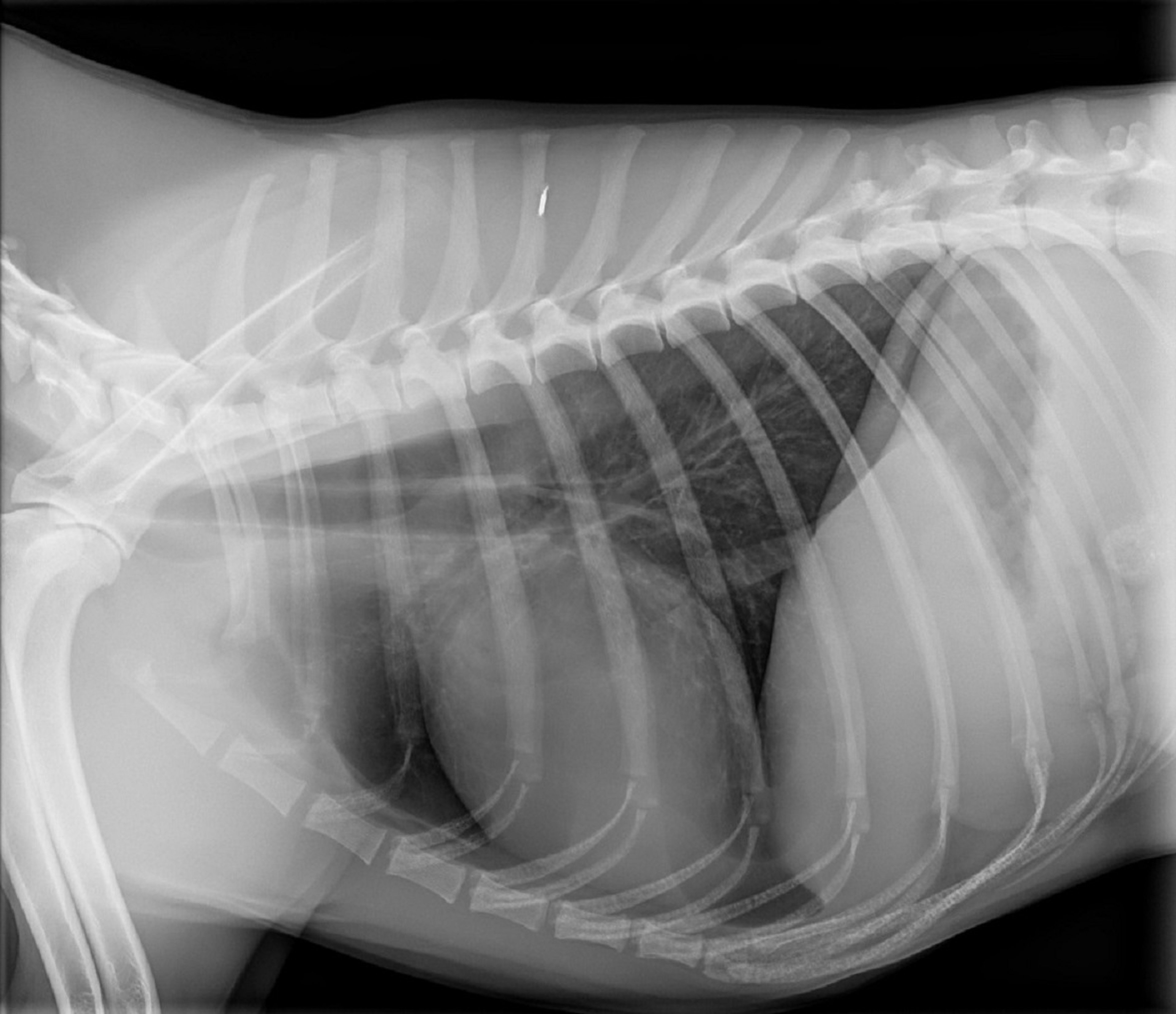
Thoracic radiographs frequently provide valuable information in the assessment of animals that have or are suspected of having heart disease. However, thoracic radiography is rarely performed in horses or cows to evaluate heart disease because of the animal's large size and body conformation, which decreases the quality of the images. In dogs, which have numerous different body types, chest conformation must always be assessed before attempting to evaluate cardiac size.
On the lateral view, dogs can be normal, shallow-chested, or deep-chested. On the dorsoventral (DV) and ventrodorsal (VD) views, they can be normal, narrow-chested, or barrel-chested.
Many small-breed dogs are shallow-chested. A shallow chest makes the cardiac silhouette appear enlarged on the lateral view and often necessitates reliance on the DV view to obtain an accurate assessment of size and shape. In deep-chested breeds, even severe cardiomegaly can look normal on the lateral view, and because the heart sits more upright in the chest, a deep chest (eg, in Doberman Pinschers with DCM) can also mask the presence of cardiomegaly on the DV view. Obesity also interferes with accurate radiographic evaluation of cardiac size because of the presence of intrapericardial fat or because the diaphragm is pushed forward, decreasing the size of the thoracic space and pushing the heart into the cranial and narrower aspect of the thoracic cavity.
Because of 1) the marked variation in chest conformation, 2) the changes observed between inspiration and expiration, and 3) the changes evident between systole and diastole, only relatively dramatic changes in overall cardiac size can be identified in most dogs. Consequently, conditions such as mild generalized cardiomegaly cannot be identified on thoracic radiographs. The one chamber where mild, moderate, and severe enlargement can be relatively accurately identified is the left atrium. Enlargement of specific cardiac chambers and great vessels makes the presence of heart disease more likely and may also provide clues as to the specific disease present.

Courtesy of Dr. Mark D. Kittleson.
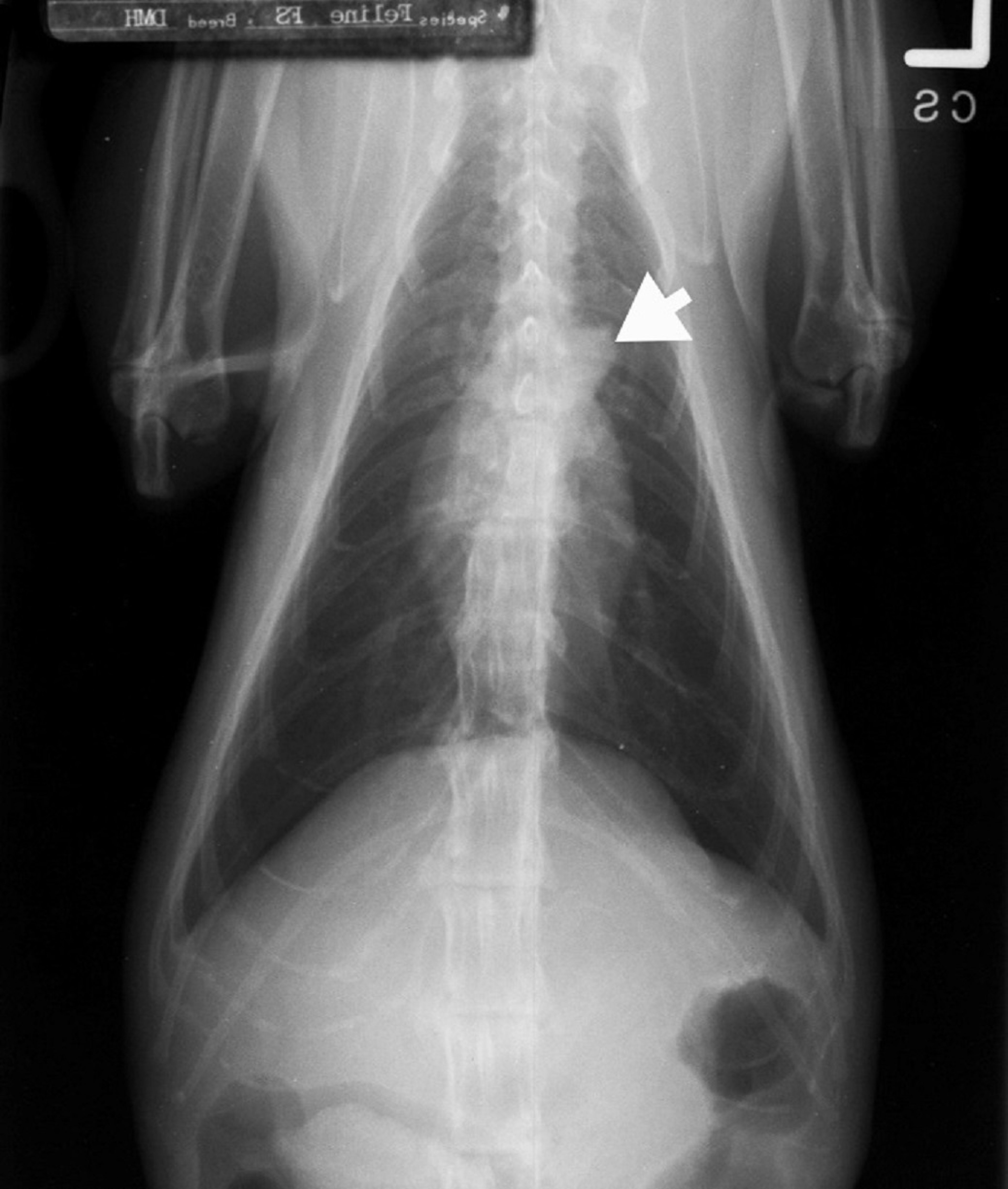
The size and shape of the heart tend to be more uniform in cats than in dogs. Normal old cats commonly have a "knob" in their proximal descending aorta that shows up on VD and DV radiographs.
Cardiogenic pulmonary edema is a common finding in animals with CHF and may be associated with pulmonary venous congestion. However, the identification of pulmonary edema is often difficult and may not be possible in some dogs and even some cats. Cardiogenic pulmonary edema in dogs is typically found in the caudodorsal aspects of the lungs. In many cases, this region has an interstitial density that is enhanced by age and by expiration, giving a false impression that pulmonary edema is present or masking the presence of pulmonary edema. Digital radiography units, especially if not set up perfectly (to match analog units), have made the diagnosis even harder in some cases.
In animals with chronic left heart failure, the left atrium is usually severely and always at least moderately enlarged. In acute left heart failure (eg, rupture of the chordae tendineae), the left atrium may not be enlarged. Pleural effusion can usually be readily identified radiographically. In dogs, pleural effusion occurs with right or biventricular heart failure. In cats and many other species (eg, humans, sheep), it occurs most commonly with left heart failure. Resolution of these abnormalities on subsequent thoracic radiographs can be considered one indication that treatment has been effective. The presence of pulmonary edema or pleural effusion does not definitively confirm a cardiogenic origin or exclude another origin.

Courtesy of Dr. Mark D. Kittleson.
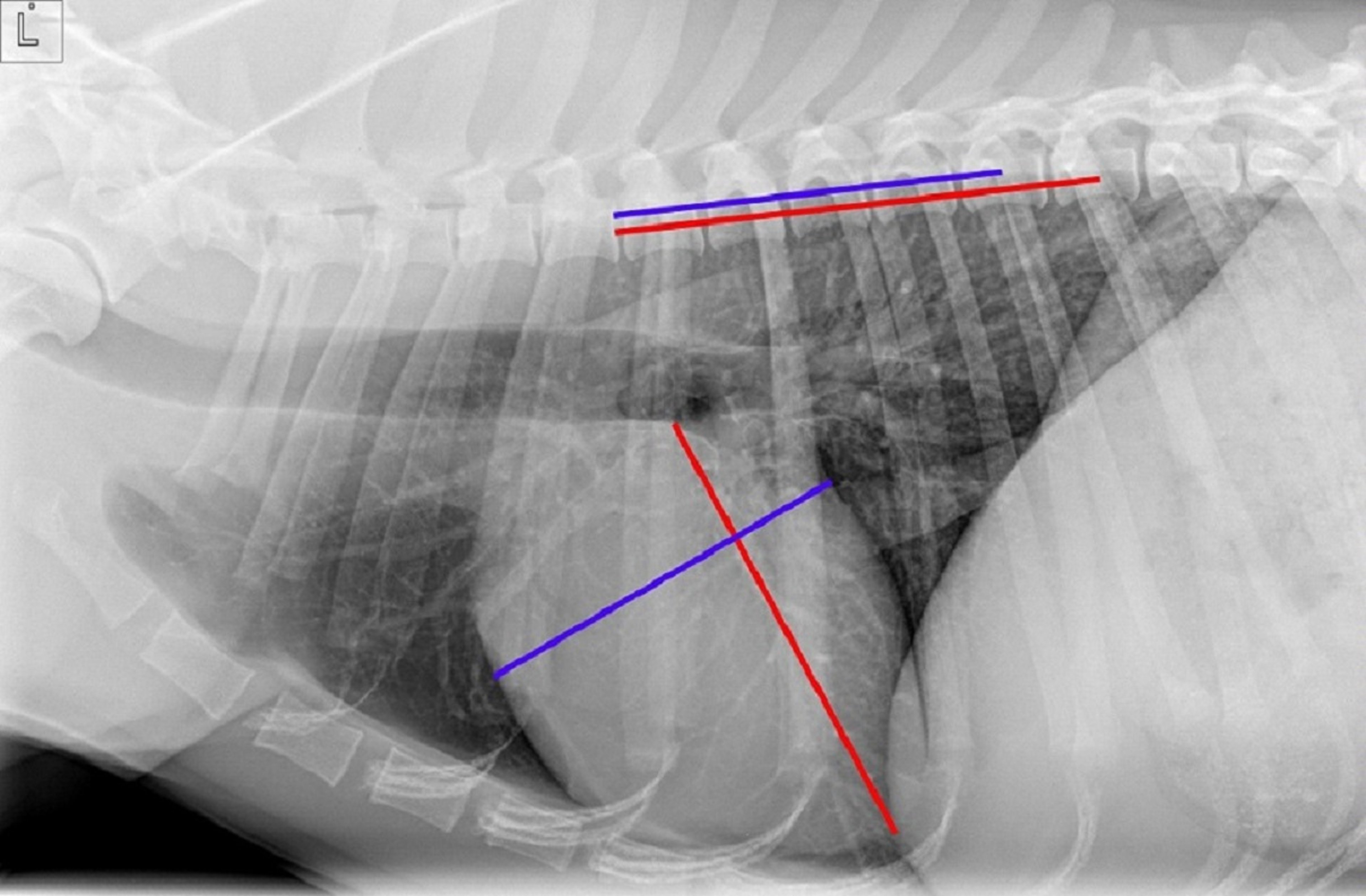
Overall cardiac size can be assessed using the vertebral heart scale or score (VHS). The lateral projection is usually used for this assessment. Manual or electronic calipers are used to measure the width of the cardiac silhouette (the maximal cranial-to-caudal diameter) and the length of the cardiac silhouette from the carina to the apex of the silhouette (dorsal to ventral). These measurements are superimposed on the thoracic vertebrae starting at the cranial edge of T4. To normalize the measurements for the size of the animal, the length and width are added together and expressed in terms of thoracic vertebral bodies. The vertebral heart score is highly variable between breeds, which limits its diagnostic utility. Furthermore, in cases where enlargement of one chamber predominates (eg, mitral regurgitation), it is more important to try to accurately assess the size of that chamber (the left atrium in the case of mitral regurgitation) than it is to determine the overall size of the cardiac silhouette.
Assessment of left atrial size is one of the most common reasons for taking thoracic radiographs. Usually this is a subjective assessment. In dogs with chronic mitral regurgitation due to myxomatous valve degeneration, the severity of the mitral regurgitation is based on left atrial size, which is generally categorized as mild, moderate, or severe enlargement. In general, only dogs with moderate to severe left atrial enlargement can be in chronic left heart failure (pulmonary edema). Assessing left atrial size is also important for determining whether a dog might benefit from the administration of pimobendan before the onset of heart failure. In general, a dog should have at least moderate left atrial enlargement before being started on pimobendan.
Electrocardiography
Electrocardiography is the recording of cardiac electrical activity from the body surface (which yields surface ECGs). It should be used primarily to identify cardiac arrhythmias. It can also identify conduction disturbances that do not alter rhythm, and it has been used to identify chamber enlargement in dogs and cats. However, the inaccuracy of electrocardiography in identifying chamber enlargement and the advent of diagnostic ultrasonography have diminished this role. In contrast to small animals, in which the Purkinje fibers penetrate only about one-third of the way into the myocardium, Purkinje fibers in horses and cattle penetrate throughout the myocardium, resulting in "burst" depolarization of the ventricles and decreased waveform production and complexes on the surface ECG. Consequently, there is no relationship between complex height on a surface ECG and chamber enlargement in horses and cattle. The most common ECG lead used in large animals is a base-apex lead that produces large deflections and is used for rhythm analysis. ECGs should be used only to characterize an arrhythmia in an animal with an auscultatory arrhythmia and to monitor rhythm during anesthesia; they should never be used as screening tools in animals as they are in human medicine (primarily for changes secondary to coronary artery disease).
Echocardiography
Echocardiography, the use of diagnostic medical ultrasonography to evaluate the heart and proximal great vessels, complements other diagnostic procedures by quantifying chamber dimensions, wall thicknesses, and the dynamic events of the cardiac cycle. It also enables visualization of the anatomy and motion of valves and visualization of congenital abnormalities ranging from a defect in the interventricular septum to a stenotic pulmonary valve. Blood flow velocity is also commonly measured, and turbulent blood flow is identified using Doppler echocardiography. Pressure gradients, blood flow volumes, and several indices of cardiac function can be calculated. Echocardiography can also identify changes in myocardial tissue texture indicative of ischemia and fibrosis and delineate masses, valvular vegetations, pericardial effusion, and many other features previously verifiable only with cardiac catheterization or at necropsy.
There are four main types of echocardiography:
Two-dimensional echocardiography provides a wedge-shaped, two-dimensional image of the heart in real time. Several standard long-axis and short-axis views obtained from standard imaging windows on the thorax have been developed for dogs, cats, horses, and cows.
M-mode echocardiography is produced by a one-dimensional ultrasonographic beam that penetrates the heart, providing an “ice-pick view” over time. The tissue interfaces that are encountered by the beam are then plotted on a screen. This mode of echocardiographic evaluation typically has been used to measure chamber dimensions, wall thickness, valve motion, and great vessel dimensions; as the frame rate of two-dimensional echocardiography has improved, however, M-mode echocardiography has lost some of its usefulness.
Doppler echocardiography measures velocity of blood flow by using the principle that an ultrasonographic beam changes frequency after contacting a moving structure (eg, RBCs, cardiac wall). Doppler echocardiography is further divided into color flow, continuous wave and tissue Doppler echocardiography.
Color flow Doppler echocardiography is a form of pulsed Doppler echocardiography prone to aliasing when high-velocity flow is encountered, enabling the detection of high-velocity (and therefore turbulent) flow in the heart and great vessels.
Continuous wave Doppler echocardiography is used to quantify high-velocity flow, and thus to calculate pressure gradients, most commonly across the regions of valves, using the modified Bernoulli equation (4 × velocity2).
Tissue Doppler echocardiography is used to measure the lower-velocity motion of cardiac structures, most commonly ventricular walls, in an attempt to quantify regional myocardial function.
Three-dimensional echocardiography is the newest modality for ultrasound imaging of the heart. By utilizing 3 dimensions, volume calculations are more accurate and lesions can be assessed more comprehensively since they can be viewed from multiple different perspectives.
Cardiac Catheterization
Cardiac catheterization is the placement of catheters into cardiac chambers and surrounding great vessels to measure pressure, inject contrast agents, and place devices (ie, "interventional cardiology"). Indications for cardiac catheterization include diagnostic evaluation (eg, when other diagnostic tests are insufficient to identify specific cardiac abnormalities or are unable to identify the severity of a lesion), presurgical evaluation (eg, to help diagnose constrictive pericarditis before surgery), therapeutic intervention, and clinical research. Diagnostic and presurgical cardiac catheterization, however, have largely been replaced by echocardiography. Currently, most cardiac catheterizations are interventional procedures to address cardiac defects (eg, closure of a patent ductus arteriosus).



