



Traumatic reticuloperitonitis of cattle occurs when animals ingest nails, pieces of wire, and other nonmetallic materials that injure the reticular wall. Sharp objects can puncture the reticulum, allowing ingesta and bacteria to leak into the peritoneal cavity, resulting in peritonitis and often leading to adhesions in the abdomen. Clinical signs include rumenoreticular atony, decreased milk production, and signs of abdominal pain. Treatment can be medical (rumen magnet and antimicrobial therapy) or surgical (foreign body removal via rumenotomy).
Traumatic reticuloperitonitis of cattle is localized inflammation in the wall of the reticulum, usually due to perforation by a sharp object (eg, nail or wire) ingested by the animal. The most common clinical findings include decreased feed intake, decreased rumen motility, mild fever, poorly digested feces, and signs of pain. Foreign body tests (eg, back grip, percussion of the reticulum with a mallet, or pole test) to elicit a grunt are an important step in clinical examination. Ultrasonographic evaluation is essential to identify inflammatory lesions of the reticulum, and radiography enables visualization of foreign bodies. Traumatic reticuloperitonitis is treated with a rumen magnet and antimicrobial therapy, and laparorumenotomy is an option when there is no response to medical treatment. Disease is much less common in other ruminants such as goats and sheep, which tend to be discriminating eaters.
Etiology of Traumatic Reticuloperitonitis in Ruminants


All of the metallic objects pictured in this photograph are foreign bodies that were extracted from the reticulum of a cow with traumatic reticuloperitonitis.
Courtesy of Dr. Ueli Braun.
Ingested wires can come from cut tires used to weigh down tarps covering silage, and other metallic fragments may come from components of mixer wagons. Production systems often use wire fencing. Aluminum and other nonmagnetic foreign bodies are uncommon.
Swallowed metallic objects, such as nails or pieces of wire, fall directly into the reticulum and can penetrate or perforate its wall and cause traumatic reticuloperitonitis. Contractions of the reticulum promote penetration of the wall by the foreign object.


This photograph shows localized peritonitis in the carcass of a cow with traumatic reticuloperitonitis.
Courtesy of Dr. Ueli Braun.
Perforation of the wall of the reticulum allows leakage of ingesta and bacteria, which contaminates the peritoneal cavity. The resulting peritonitis is generally localized and frequently results in adhesions. Less commonly, more severe diffuse peritonitis, pleuritis, pericarditis, hepatic, or splenic abscess develops.
Clinical Findings of Traumatic Reticuloperitonitis in Ruminants


Photograph of a Holstein Friesian cow with an arched back, a clinical sign associated with traumatic reticuloperitonitis.
Courtesy of Dr. Ueli Braun.
Clinical signs indicating initial penetration of the reticulum in traumatic reticuloperitonitis include the sudden onset of ruminoreticular atony, moderate ruminal tympany, and a sharp decrease in milk production. Rectal temperature is mildly to severely increased. Heart rate is normal or slightly increased, and respiration is usually shallow and rapid. Clinical signs include an arched back, erect hairs at the withers, anxious expression, reluctance to move, and an uneasy, careful gait. Forced sudden movements, as well as defecating, urinating, lying down, and getting up, may be accompanied by bruxism and groaning. Grunting can often be induced for diagnostic purposes by offering feed, by leading the animal downhill, or by conducting one of the foreign body tests (eg, back grip, percussion of the reticulum with a mallet, or pole test).
Chronic cases are characterized by illness or poor-doing for weeks or months, sometimes interrupted by periods of apparent improvement or by recurring episodes of illness marked by decreased feed intake, poor rumination, decreased rumen motility, mild recurring ruminal tympany, obstipation or diarrhea, poorly digested feces, weight loss, and low milk production.
As the acute inflammation subsides, signs of cranial abdominal pain become less apparent, and the rectal temperature usually returns to normal.
Complications of traumatic reticuloperitonitis include traumatic pericarditis, hepatic inflammation or abscesses, splenic inflammation or abscesses, pleuropneumonia, vagal indigestion syndrome, and generalized peritonitis.
Diagnosis of Traumatic Reticuloperitonitis in Ruminants
Clinical examination
Testing for presence of a reticular foreign body (eg, back grip, pain percussion, or pole test)
Laboratory testing (eg, serum-to-peritoneal fluid glucose concentration difference or peritoneal fluid D-dimer concentration)
Ultrasonographic evaluation of the ventral abdomen to identify localized peritonitis adjacent to the reticulum
Radiography to visualize metallic foreign bodies in the reticulum


The veterinarian in this photograph is using a rubber hammer to elicit a pain response by means of percussion in the region of the reticulum in a Holstein Friesian cow suspected of having traumatic reticuloperitonitis.
Courtesy of Dr. Ueli Braun.
Cattle suspected of traumatic reticuloperitonitis should be tested for signs of pain, including grunting and bruxism. Foreign body tests to elicit a grunt are an important part of clinical examination; however, the same response may be elicited in other painful abdominal and thoracic conditions as well. Cattle with acute traumatic reticuloperitonitis generally grunt in pain more readily than do those with chronic traumatic reticuloperitonitis. The back grip, percussive pain, and pole tests are the most important tests in diagnosing traumatic reticuloperitonitis. Based on a retrospective study of 508 cattle, foreign body tests (pole test, back grip, percussion) have only fair diagnostic reliability and may result in false negatives.
Although not always necessary, laboratory tests may be helpful in diagnosing traumatic reticuloperitonitis. A differential WBC count more accurately indicates traumatic reticuloperitonitis than does a total WBC count. During the first 3 days of acute localized peritonitis, a characteristic clinicopathologic finding is an increased neutrophil count. After the third day, the findings are normalized in uncomplicated cases. Hyperfibrinogenemia and hyperproteinemia are more reliable than WBC counts at indicating traumatic reticuloperitonitis. Increased fibrinogen concentration may be evident as early as 2–3 days after traumatic reticuloperitonitis onset. In chronic cases, an increase in gamma-globulin concentration accounts for the increase in total protein concentration.
The gamma-globulin and fibrinogen concentrations can be determined simply and quickly by the glutaraldehyde coagulation test, in which they are positively correlated with the time to gel formation. The diagnostic sensitivity of the test is 97.8% for a coagulation time of 3 minutes, and 87.9% for 6 minutes.
Results of rumen fluid analysis are not diagnostic for traumatic reticuloperitonitis. Peritoneal fluid analysis can help determine whether peritonitis is present. Ideally, ultrasonography-guided abdominocentesis using a spinal needle with stylet yields samples that can be assessed for amount, color, transparency, odor, and consistency as well as for the presence of other material. The specific gravity and total solids concentration in a sample can be evaluated by refractometry. Exudates that indicate traumatic reticuloperitonitis are generally cloudy and watery to viscous fluids that may have a foul odor because of bacteria and may clot quickly after being collected. Flecks of fibrin are often present, the specific gravity is >1.015, and the total solids concentration is >30 g/L. When assessing aspirated peritoneal fluid in cases of traumatic reticuloperitonitis, standard definitions differentiating abdominal transudates from abdominal exudates do not always apply because healthy and sick animals may show similar concentrations of protein and fibrinogen in the peritoneal fluid.
The concentrations of other substances (eg, glucose and D-dimer) can be measured in the peritoneal fluid and serum, and their values from the two sources compared to clarify the diagnosis. In healthy cattle, concentrations of glucose in blood and peritoneal fluid are usually similar. A comparatively lower concentration of glucose in the peritoneal fluid indicates the presence of bacteria, which metabolize glucose. Serum-to-peritoneal fluid glucose concentration difference is therefore considered a very specific criterion for the diagnosis of septic peritonitis. Peritoneal fluid D-dimer concentration is considered the best criterion for the diagnosis of peritonitis because both the sensitivity and the specificity are high.

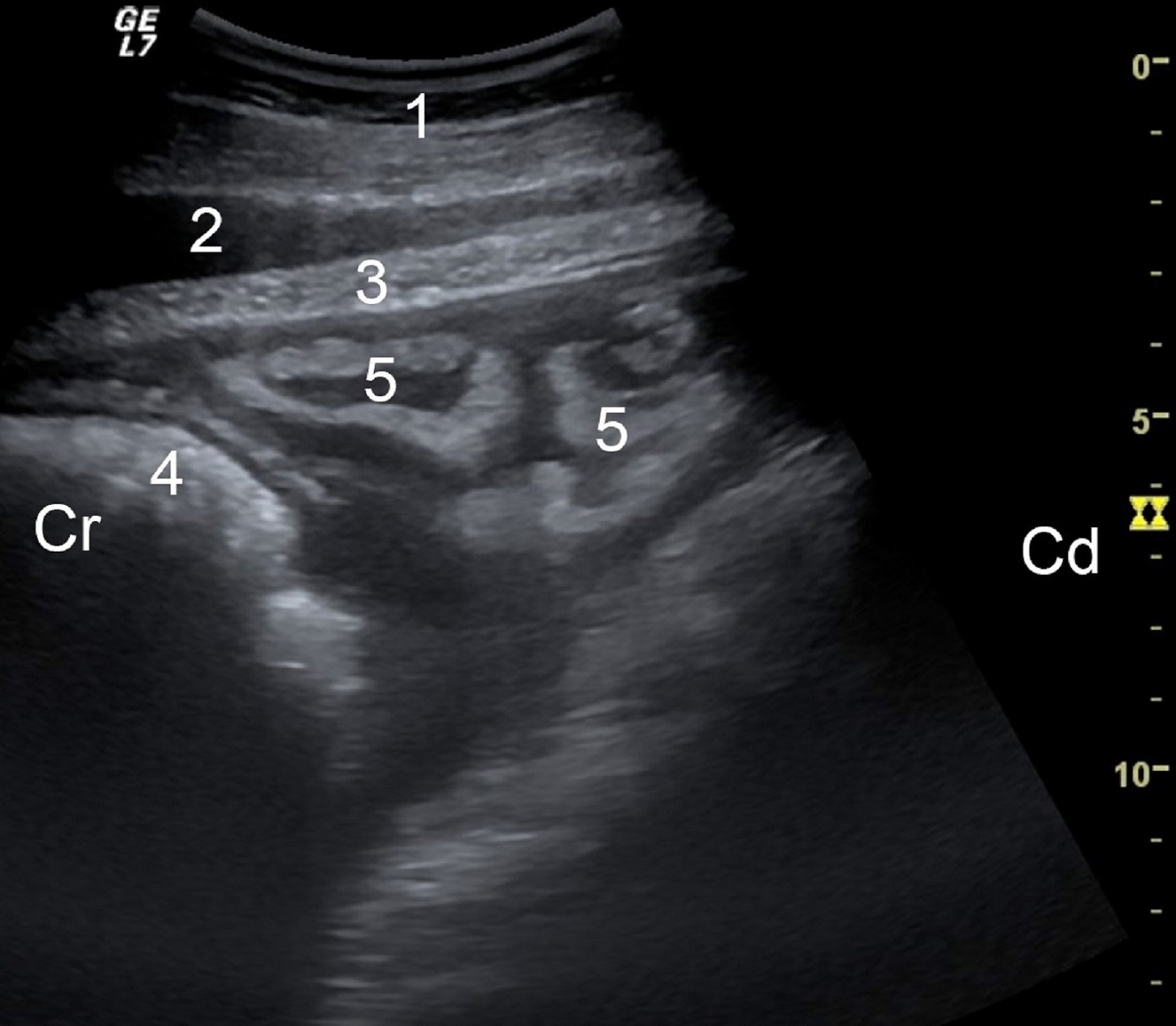
Ultrasonogram showing fibrin accumulation in the area of the reticulum imaged from the sternal region of a cow with traumatic reticuloperitonitis. 1, abdominal wall; 2, musculophrenic vein; 3, diaphragm; 4, reticulum; 5, echogenic fibrin with fluid inclusions; Cr, cranial; Cd, caudal.
Courtesy of Dr. Ueli Braun.

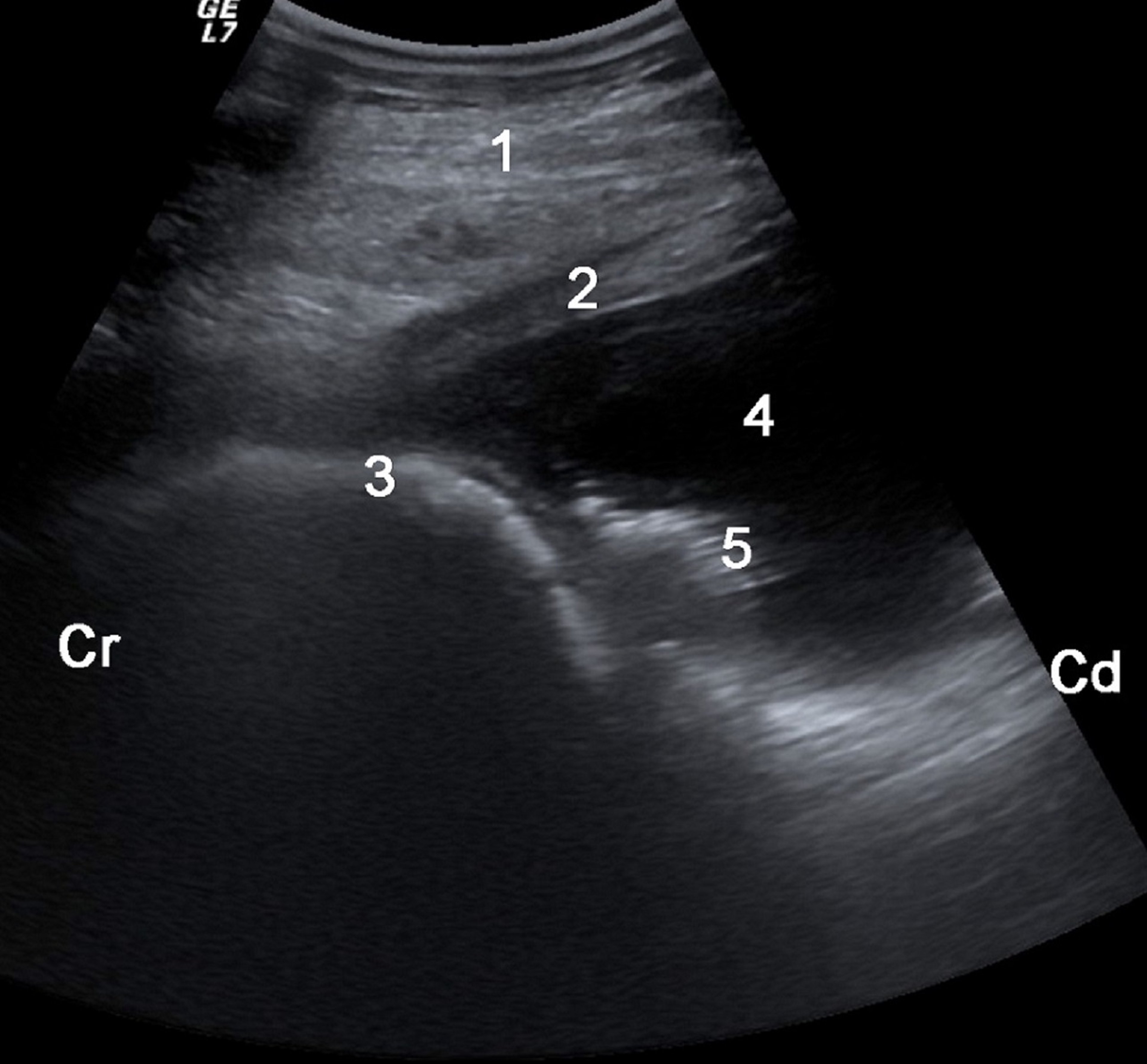
Ultrasonogram showing fluid accumulation in an area of the reticulum imaged from the sternal part of the ventral abdominal wall of a cow with traumatic reticuloperitonitis. 1, abdominal wall; 2, diaphragm; 3, reticulum; 4, fluid; 5, echogenic fibrin; Cr, cranial; Cd, caudal.
Courtesy of Dr. Ueli Braun.

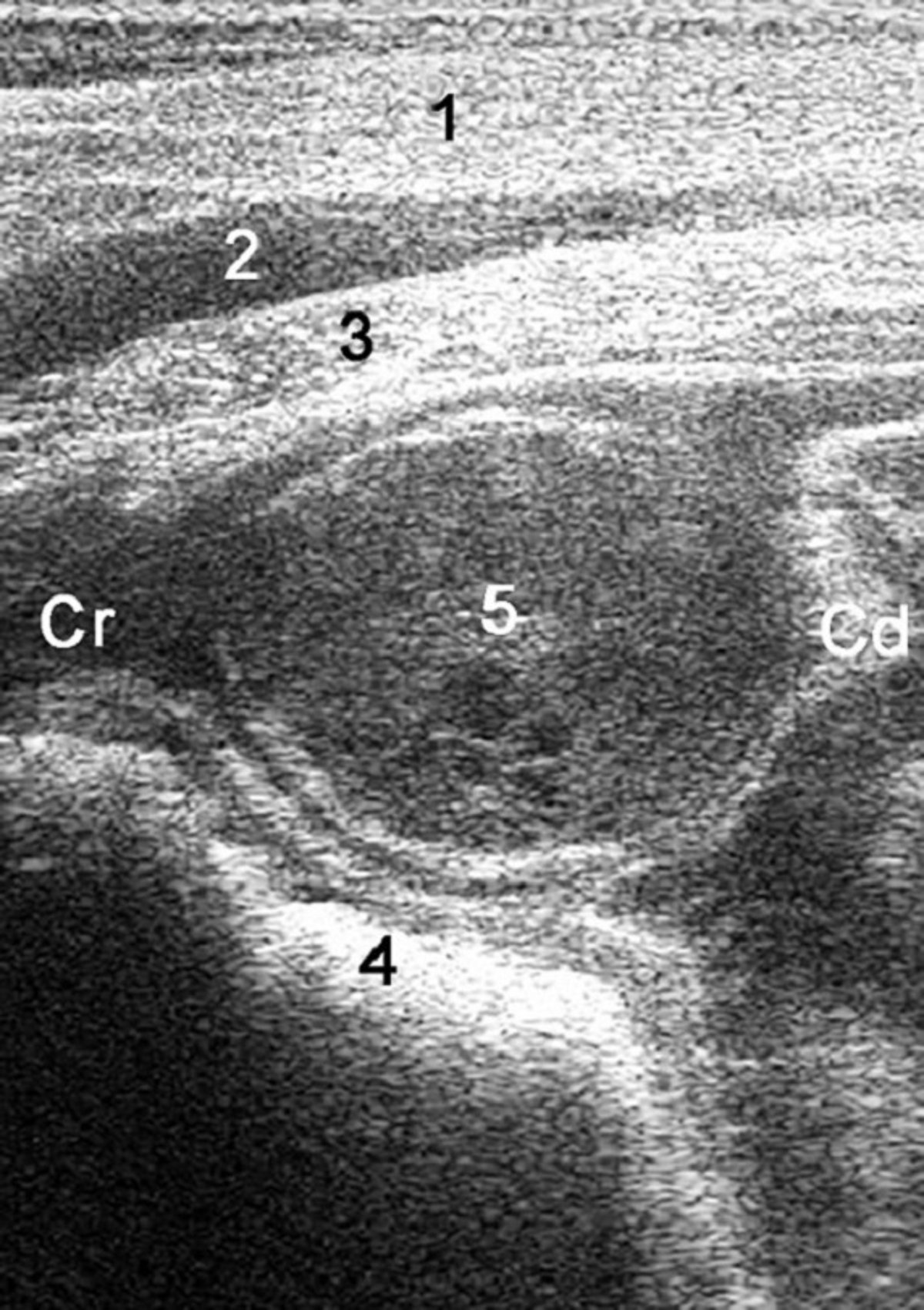
Ultrasonogram showing a reticular abscess in the paramedian sternal region of a cow with traumatic reticuloperitonitis. 1, abdominal wall; 2, musculophrenic vein; 3, diaphragm; 4, reticulum; 5, abscess; Cr, cranial; Cd, caudal.
Courtesy of Dr. Ueli Braun.
Ultrasonographic examination of the ventral abdomen using a 3.5- to 5.0-MHz linear or convex transducer is the most accurate way to diagnose localized peritonitis near the reticulum and characterize reticular contraction frequency. The transducer is applied to the ventral aspect of the thorax on both sides of the sternum and to the lateral aspects of the thorax up to the level of the elbow. If abnormalities are detected, the area being examined is expanded to determine the extent of the lesions. Inflammatory changes appear as echogenic deposits, with or without hypoechoic or anechoic fluid pockets, and structures of various shapes and echogenicities with central echogenic fluid collections. Inflammatory lesions may involve the adjacent organs (typically spleen, liver, and rumen).
Cattle with traumatic reticuloperitonitis frequently have peritoneal effusion in which the accumulation of fluid lacks an echogenic border and is limited to the reticular region. The fluid appears anechoic to hypoechoic depending on the amount of fibrin and cellular material it contains. Fluid surrounding the lesions may contain strands of fibrin that stand out on an ultrasonogram. Reticular abscesses that have an echogenic capsule and a cavity with content that ranges from hypoechoic to moderately echogenic and that is either homogeneous or heterogeneous are present in about 20% of cattle with traumatic reticuloperitonitis. Rarely, ultrasonography may show magnets in the reticulum or foreign bodies either inside or outside of the reticulum.
Most cattle with traumatic reticuloperitonitis have a change in the frequency of reticular contractions.

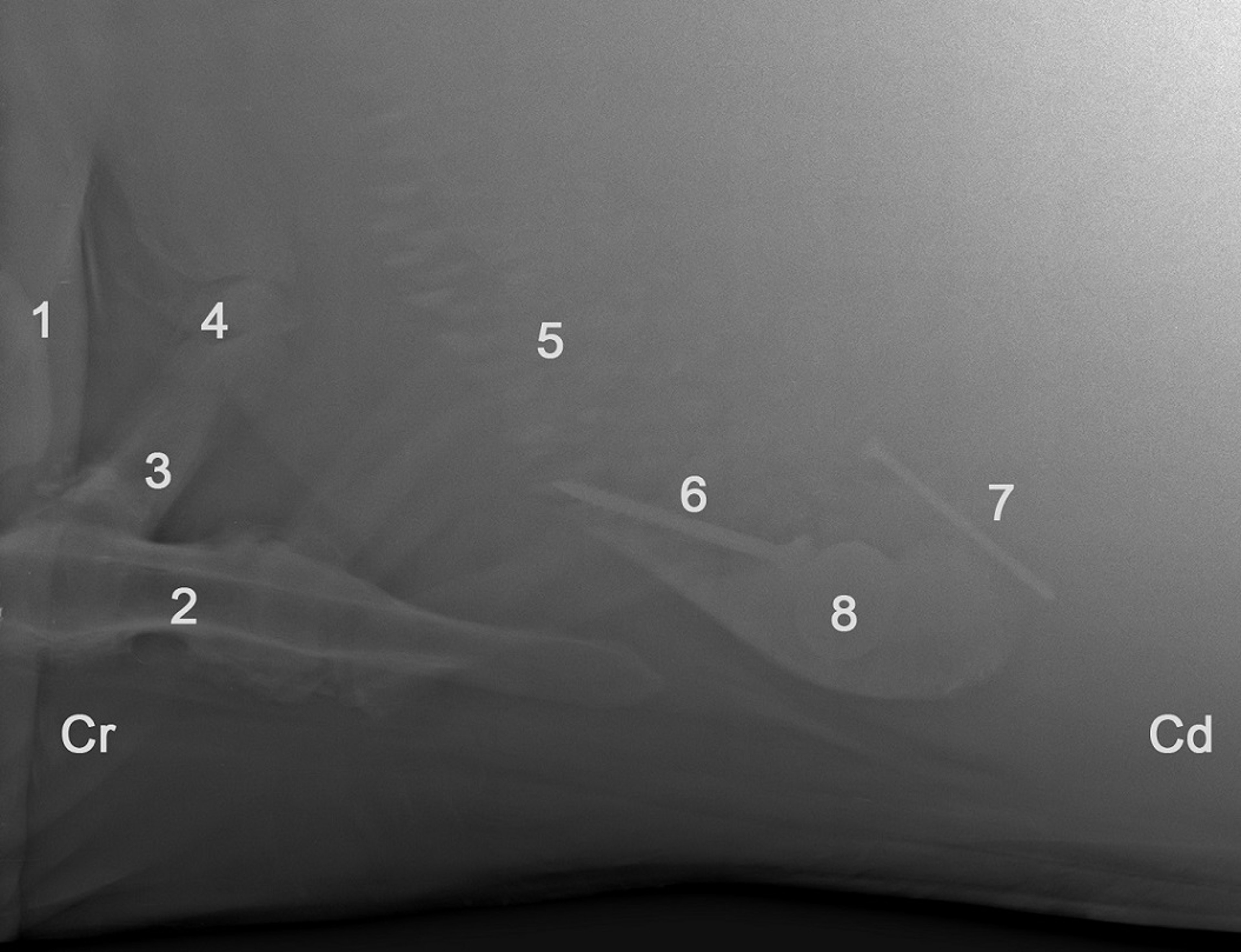
Lateral radiographic view of the reticulum, showing two penetrating reticular foreign bodies in a cow with traumatic reticuloperitonitis. A screw has penetrated the cranial reticular wall, and a nail has penetrated the caudal reticular wall. A magnet is also present in the reticulum and is in contact with the screw. 1, elbow; 2, sternum; 3, rib; 4, diaphragm; 5, reticulum; 6, screw; 7, nail; 8, magnet in reticulum; Cr, cranial; Cd, caudal.
Courtesy of Dr. Ueli Braun.
Radiography is the usual initial modality of choice to visualize metallic foreign bodies in the reticulum. To be considered clinically relevant, linear foreign bodies must be ≥1 cm long. Even more important than the presence of a foreign body is its position. Foreign bodies most likely to have penetrated the reticulum are those that do not contact the reticulum's ventral aspect or those that are situated at an angle >30° to the reticulum's ventral aspect. Any foreign body that is outside of the reticulum's outer contour to some extent has punctured the reticular wall. Foreign bodies that lie flat on the reticulum's ventral aspect or whose positions vary on serial radiographs are considered nonpenetrating, but they still pose a risk for traumatic reticuloperitonitis. Foreign bodies on the ventral aspect of the reticulum but not attached to a magnet in the reticulum may be nonmagnetic.
Treatment of Traumatic Reticuloperitonitis in Ruminants
Oral administration of a rumen magnet and antimicrobial therapy over several days (medical treatment)
Rumenotomy if medical (conservative) treatment fails
Initial treatment of cattle suspected of having traumatic reticuloperitonitis consists of oral administration of a rumen magnet (if the animal does not already have one; give only one magnet per animal) and antimicrobial therapy (most commonly penicillin or broad-spectrum antimicrobials such as ampicillin, ceftiofur, and tetracyclines). Anti-inflammatory drugs, including flunixin meglumine, ketoprofen, and meloxicam, are administered to manage pain. By capturing ferromagnetic foreign bodies in the reticulum and rumen, magnets prevent trauma. How well the rumen magnet works depends mainly on where the foreign body is situated in the reticulum; a magnet can pick up foreign bodies that on the ventral aspect of the reticulum or that are upright more easily than those that either are not in contact with the ventral aspect of the reticulum or are penetrating the reticulum.
Treatment is considered successful when the rectal temperature normalizes and eating and rumination improve within 3–5 days. Radiographic evidence that a foreign body is completely attached to a magnet also confirms the success of treatment. If conservative treatment fails, the animal may need to be treated surgically or euthanized. The decision of which course to follow should be made only after radiographic evaluation confirms that the foreign body is not attached to the magnet.
Two main surgical techniques are used for rumenotomy. In laparorumenotomy, the rumen is permanently sutured to the peritoneum and transverse fascia so that the entire procedure—including access to the rumen and healing of the incision—can take place outside of the peritoneum. In temporary extra-abdominal fixation, the surgeon repositions the sutured rumen to its normal position in the abdomen. Laparotomy is carried out in the left flank, the rumen is partially emptied so that the reticular lumen can be palpated, and foreign bodies are removed.
Abscesses that are firmly and broadly attached to the reticulum can be incised and the content drained into the reticulum. For abscesses attached to the thoracic or abdominal wall, transcutaneous drainage guided by ultrasonography is the treatment of choice.
Prevention of Traumatic Reticuloperitonitis in Ruminants
Measures to prevent traumatic reticuloperitonitis include avoiding the use of baling wire, passing feed over magnets to remove metallic objects, keeping cattle away from sites of new construction, and completely removing old buildings and fences. In addition, magnets may be administered by mouth. There is good evidence that giving magnets to all cattle at ~1 year of age minimizes the incidence of traumatic reticuloperitonitis.
Key Points
Cattle will ingest sharp objects that can puncture the reticulum and cause peritonitis
Clinical signs are of sudden onset and include sharply decreased feed intake and milk production; the classic sign of traumatic reticuloperitonitis is an arched back
Foreign body tests (eg, back grip, percussive pain, and pole tests) are key in diagnosing traumatic reticuloperitonitis
Treatment can be medical (rumen magnet and antimicrobial therapy) or surgical (foreign body removal via rumenotomy)
For More Information
Braun U, Gerspach C, Ohlerth S, et al. Review: aetiology, diagnosis, treatment and outcome of traumatic reticuloperitonitis. Vet J 2020;255:105424.
Braun U, Warislohner S, Torgerson P, et al. Clinical and laboratory findings in 503 cattle with traumatic reticuloperitonitis. BMC Vet Res 14, 66 (2018). https://doi.org/10.1186/s12917-018-1394-3





