

Malabsorption is a failure of digestion and is caused by exocrine pancreatic insufficiency (EPI) or small intestinal disease. Diarrhea and weight loss, despite an increased appetite, are the hallmarks of malabsorption. Measuring serum trypsin-like immunoreactivity will test for EPI, and then, if ruled out, small intestinal disease can be investigated by imaging, measuring serum folate and cobalamin concentrations, and ultimately by intestinal biopsy. However, empirical diet trials are indicated before small intestinal biopsy if the patient is still eating. Enzyme replacement is the basis of treatment of EPI, and small intestinal diseases failing to respond to diet may be treated with antimicrobials or immunosuppressives.
Malabsorption is the defective uptake of a dietary constituent resulting from interference with its digestion or absorption, due to either exocrine pancreatic insufficiency (EPI) or small intestinal disease.
The primary functions of the exocrine pancreas and the small intestine are the digestion and absorption of nutrients. These occur in sequential phases: intraluminal digestion, mucosal digestion and absorption, and delivery of nutrients to the body. Pancreatic insufficiency and a number of chronic small intestinal diseases cause malabsorption by interfering with one or several of these processes.
Malabsorptive syndromes have been studied in most detail in dogs; however, basic diagnostic and therapeutic principles are relevant to other species. Malabsorption typically results in diarrhea, altered appetite, and weight loss, but a number of animals (especially cats) may not have overt diarrhea because of the reserve capacity of the colon to conserve water.
Physiology of Malabsorption Syndromes in Small Animals
Normal digestive processes convert polymeric dietary nutrients (proteins, polysaccharides, and fats) into forms (mainly monomers) that can cross the luminal surface (brush border) of intestinal absorptive epithelial cells (ie, enterocytes). Most digestive enzymes are secreted by the pancreas; therefore, by causing maldigestion, EPI is a major cause of malabsorption. Brush border enzymes digest oligopeptides and disaccharides into smaller units to facilitate their absorption. These enzymes work either at the surface of the enterocyte in association with transport proteins for their specific products or in the intestinal lumen, where they are released after cleavage by pancreatic peptidases or enzymes freed from exfoliated senescent enterocytes.
The main digestible carbohydrates in the diet are starch, glycogen, sucrose, and lactose. Their digestion proceeds as follows:
Starch and glycogen are hydrolyzed by pancreatic amylase to the oligosaccharides maltose, maltotriose, and alpha-limit dextrins.
Oligosaccharides and dietary disaccharides (sucrose, lactose) are further hydrolyzed to monosaccharides by enzymes located on the brush border of enterocytes.
The final products of hydrolysis (glucose, galactose, and fructose) are actively transported into the enterocyte by sodium-linked carrier-mediated processes, driven by a sodium-potassium ATPase export pump.
Within enterocytes, glutamine, not the glycolytic pathway, is used as an energy source: Glucose is passed by facilitated diffusion via a transport protein on the basolateral enterocyte membrane down a concentration gradient into the extracellular space, and then by diffusion into the portal venous circulation.
Protein digestion and absorption follow a similar pattern:
Proteolytic enzymes from the stomach (pepsin) and pancreas (trypsin, chymotrypsin, elastase) degrade protein into a mixture of short-chain oligopeptides, dipeptides, and amino acids.
Oligopeptides are further hydrolyzed by brush-border peptidases.
Dipeptides and amino acids cross the brush-border membrane on specific carrier proteins.
The products of fat digestion and fat-soluble molecules (eg, vitamins A, D, E, and K) do not need specific carriers to cross the phospholipid barrier of the enterocyte brush border. However, intraluminal degradation of triglycerides is essential:
Fat in the duodenum stimulates release of cholecystokinin, which, in turn, stimulates secretion of pancreatic lipase and emptying of bile from the gallbladder.
After solubilization by bile salt micelles, triglycerides are digested by pancreatic lipase to monoglycerides and free fatty acids.
At the enterocyte luminal membrane, monoglycerides and free fatty acids disaggregate from the micelle and are passively absorbed into the cell.
Released bile salts remain within the lumen and are ultimately reabsorbed in the ileum and undergo enterohepatic recycling.
Once inside the cell, monoglycerides and free fatty acids are re-esterified to triglycerides and incorporated into chylomicrons, which subsequently enter the central lacteal of the villus, being delivered to the venous circulation via the thoracic duct.
Medium-chain triglycerides (C8–C10) may be absorbed directly into the portal blood, providing an alternative route for fat uptake in case of lymphatic obstruction; some medium-chain triglycerides normally enter the circulation via the thoracic duct, so consequently, they are no longer recommended in management of lymphangiectasia.
Etiology and Pathophysiology of Malabsorption Syndromes in Small Animals
Malabsorption is a consequence of interference with mechanisms responsible for either the degradation or absorption of dietary constituents (see the table ).
Mechanisms of Malabsorption
Location | Disease | Mechanism |
|---|---|---|
Luminal | Exocrine pancreatic insufficiency | Lack of pancreatic enzymes (maldigestion) |
Luminal | Small-intestinal dysbiosis
| Bacterial activity: bile salt deconjugation, fatty acid hydroxylation, competition for cobalamin and nutrients |
Mucosal | Infectious enteropathies
Chronic inflammatory enteropathy
Neoplastic infiltration | Mucosal damage: inflammation, brush border defects, disturbed enterocyte function, reduction of surface area |
Mucosal | Villous atrophy | Reduction in surface area, immature enterocytes due to increased cell turnover with reduced brush border enzyme expression |
Mucosal | Inherited and acquired brush border enzyme deficiencies | Lactase deficiency, diffuse small-intestinal disease |
Postmucosal | Lymphangiectasia | Lymphatic obstruction impairs delivery of chylomicrons |
Postmucosal | Vasculitis, portal hypertension | Impaired delivery |
Diseases that disrupt the synthesis or secretion of digestive pancreatic enzymes cause maldigestion with subsequent malabsorption, so that the end result is the same.
An important syndrome is EPI, which occurs if there is a loss of approximately 85–90% of exocrine pancreatic mass. EPI is characterized by severe maldigestion-malabsorption of starch, protein, and, most notably, fat. Fat malabsorption may also be present with a deficiency of intraluminal bile salts due to cholestatic liver disease or extrahepatic biliary obstruction.
In dogs, EPI is most commonly due to acinar atrophy. End-stage chronic pancreatitis is less common and occurs in older animals; pancreatic hypoplasia is a rare congenital cause. Canine EPI is often complicated by secondary small intestinal dysbiosis (disturbance of the normal GI microbiota), which further disrupts nutrient digestion and absorption. EPI is relatively uncommon in cats and is most frequently due to chronic pancreatitis.
Intraluminal effects of bacteria can have important consequences, and small intestinal dysbiosis is a common consequence of EPI and small intestinal disease. It can also be caused by dietary changes and antimicrobial use. Bacterial deconjugation of bile salts interferes with micelle formation, which results in malabsorption of lipid. Deconjugated bile salts and bacterial hydroxylation of fatty acids exacerbate diarrhea by stimulating colonic secretion.
Small intestinal disease can cause malabsorption by decreasing the number or function of individual enterocytes. Diffuse diseases of the small intestinal mucosa can result in decreased activity of brush-border enzymes, decreased carrier-protein activity, decreased mucosal absorptive surface area, and interference with final transport of nutrients into the circulation.
Weight loss may be compounded by decreased nutrient intake due to inappetence in severe inflammatory or neoplastic diseases.
In addition, with malabsorption of nutrients, strong intraluminal osmotic effects diminish intestinal and colonic absorption of water and electrolytes, resulting in diarrhea. This response may be exacerbated if mucosal damage is accompanied by intestinal inflammation, which can cause increased intestinal secretion and exudation of fluid.
Histological changes in chronic inflammatory enteropathies (eg, villous atrophy and infiltration with inflammatory cells) indicate intestinal disease but do not identify the underlying cause. For example, lymphocytic-plasmacytic enteritis may be a common response pattern of the intestinal mucosa to different provocative agents, particularly microbial or dietary antigens. In many cases, the underlying cause cannot be identified except by the response to empirical treatment trials. Thus, potential causes of mucosal inflammation in chronic enteropathies include idiopathic inflammatory bowel disease (IBD), enteric pathogens (eg, Giardia, Histoplasma, Pythium), dietary sensitivity, and intestinal neoplasia (eg, lymphosarcoma).
Acquired brush-border defects may be present in generalized small intestinal diseases. However, the main inherited brush-border enzyme deficiency reported, when no histological abnormalities are present, is a relative lactase deficiency in cats. Their lactase activity declines after weaning, and they may become lactose intolerant. In both dogs and cats, lactose intolerance may also develop secondarily to nonspecific damage to the brush border, which is why feeding dairy products to animals with diarrhea should be avoided.
Postmucosal obstruction may be observed with lymphatic obstruction (especially lymphangiectasia) and vascular compromise (portal hypertension, vasculitis). Intestinal lymphangiectasia causes intestinal protein loss as well as severe fat malabsorption, as ruptured lacteals leak lipoproteins and chylomicrons.
Usually in malabsorption, a number of nutrients are affected, and consequently diarrhea occurs; malabsorption of a single ingredient without any GI signs is rare (eg, inherited selective cobalamin malabsorption [Imerslund-Gräsbeck syndrome] in Giant Schnauzers, Australian Shepherds, Beagles, and Border Collies). The large absorptive capacity of the colon may prevent overt diarrhea in some animals (especially cats), despite pronounced malabsorption and weight loss.
Pearls & Pitfalls
|
Clinical Findings of Malabsorption Syndromes in Small Animals
Clinical signs of malabsorption are mainly the result of lack of nutrient uptake and losses in the feces. The primary cause, duration, and severity of mucosal damage determine the severity of clinical signs, which typically include chronic diarrhea, weight loss, and altered appetite (anorexia or polyphagia). However, the absence of diarrhea does not exclude the possibility of severe GI disease.
Weight loss may be substantial despite a ravenous appetite, sometimes characterized by coprophagia and pica. Typically, animals with malabsorption are systemically well and hungry, unless there is severe inflammation or neoplasia or hypoproteinemia.
Nonspecific clinical signs may include dehydration, anemia of chronic disease or small intestinal blood loss, and ascites or edema in cases of hypoproteinemia.
Thickened bowel loops or enlarged mesenteric lymph nodes may be palpable, especially in cats.
Diagnosis of Malabsorption Syndromes in Small Animals
Rule out other causes of clinical signs
Perform adjunctive tests, intestinal biopsy, and empirical treatment trials
Chronic diarrhea and weight loss are nonspecific clinical signs common to a variety of systemic and metabolic diseases, as well as malabsorption, although systemic diseases typically cause anorexia. A thorough diagnostic approach in dogs and cats with clinical signs suggestive of malabsorption is therefore needed to help exclude association with possible underlying systemic or metabolic disease. A precise diagnosis is also important for selecting treatment and assessing prognosis.
The diagnosis of small intestinal disease is difficult because of limitations of routine screening procedures, the need for biopsy in many cases, and frequently the absence of pathognomonic histological changes.
History in Malabsorption Syndrome
Dietary history is particularly important, because it may suggest specific dietary intolerance, indiscretion, or sensitivity. Small- and large intestinal diarrhea may be distinguished by a number of features (see the table Differentiation of Small Intestinal from Large Intestinal Diarrhea).
Distinguishing small- from large intestinal diarrhea is helpful in identifying differential diagnoses and deciding where to take biopsies. Suspected large intestinal disease in dogs may be evaluated by colonoscopic biopsy. However, diffuse disease is more common, and if clinical signs of large intestinal disease are accompanied by weight loss, large volumes of feces, or hypocobalaminemia, then there is almost certainly concurrent small intestinal disease.
Physical Examination in Malabsorption Syndrome
A thorough physical examination should be performed. Abdominal palpation is essential to identify abnormalities, and rectal examination is required even when no large intestinal disease is suspected, both to provide a fecal sample and also to identify previously unreported GI bleeding.
In middle-aged to older cats, the thyroid should be palpated carefully (and serum T4 assayed), because clinical signs of hyperthyroidism can closely mimic those of primary intestinal malabsorption.
Minimum Database in Malabsorption Syndrome
Initial evaluation should include a minimum database (CBC, biochemical profile, urinalysis, fecal examination) to rule out non-GI disease.
Endocrine disorders, including hypoadrenocorticism (in the dog) and hyperthyroidism (in the cat), should be ruled out.
Hematologic findings in small intestinal disease sometimes include the following:
anemia from chronic blood loss (microcytic, hypochromic) or from chronic inflammation (normocytic, normochromic)
neutrophilia and/or monocytosis associated with intestinal inflammation, infectious enteropathies, or neoplasia
eosinophilia associated with parasitism and eosinophilic enteritis
lymphopenia associated with intestinal lymphangiectasia and with a stress leukogram in dogs
Lymphocytosis (or even a normal lymphocyte count) in a sick dog raises the suspicion of hypoadrenocorticism.
Pearls & Pitfalls
|
Biochemical tests and urinalysis help to exclude systemic diseases that cause chronic diarrhea, most notably hypoadrenocorticism, protein-losing nephropathies, chronic kidney disease, and liver disease:
Hypoproteinemia is frequently secondary to protein-losing enteropathy (PLE) and occurs more commonly in dogs than cats. In most cases of PLE, serum albumin and globulin concentrations are both low, but low albumin concentration alone does not exclude it; IBD and neoplasia are occasionally associated with hyperglobulinemia as well as hypoalbuminemia.
Activity of hepatocellular enzymes (ALT, AST) may be increased as a consequence of increased intestinal permeability, allowing more antigens to reach the liver; in such cases, a bile acid stimulation test as well as ultrasonography should be performed to exclude primary liver disease. However, cats may have concurrent IBD and cholangitis (triaditis).
Activity of cholestatic enzymes (ALP, GGT) tends to be increased in biliary and pancreatic disease.
Urinalysis is important to exclude renal causes of hypoalbuminemia and/or renal disease. However, sometimes both exist together (eg, the familial PLE and protein-losing nephropathy of Soft Coated Wheaten Terriers).
Hypocholesterolemia may develop with fat malabsorption and is most notable in lymphangiectasia.
Fecal analysis may reveal fat, undigested muscle fibers, or starch. They are indirect evidence for malabsorption but are nonspecific findings. Fecal analysis is primarily indicated for the identification of infectious agents:
Feces should be examined for endoparasitic ova and oocysts (especially hookworms and Giardia in dogs and Tritrichomonas and Giardia in cats). Giardia oocysts can be detected using serial zinc sulfate fecal flotations or a commercially available SNAP assay or ELISA; the latter is easier to perform, and its sensitivity is better than fecal flotation performed by inexperienced personnel. Tritrichomonas typically causes colitis in cats rather than malabsorption and is best diagnosed by PCR assay. Cytological evaluation of rectal scrapings may reveal Histoplasma organisms. Cryptosporidium is a rare cause of malabsorption and is best identified in feces by immunofluorescence.
Potentially pathogenic bacteria (including Salmonella and Campylobacter) can be isolated by stool culture. However, isolation of pathogenic bacteria is not conclusive proof of causation, because such organisms can be found in the stool of clinically normal animals. Speciation of Campylobacter isolates by PCR assay allows the pathogenic C jejuni to be distinguished from the more common and probable commensal C upsaliensis. Some Escherichia coli are potential pathogens; however, molecular techniques to identify genes encoding pathogenicity determinants are required for diagnosis.
Specific Rule-Outs in Malabsorption Syndrome
Once obvious dietary, systemic, parasitic, and infectious causes of chronic small intestinal diarrhea have been eliminated, the next step is differentiation of specific non–small intestinal causes of malabsorption:
In dogs, EPI should be ruled out before investigating small intestinal causes of malabsorption. The diagnosis of EPI is relatively straightforward, whereas that of small intestinal disease is more complex. The serum trypsin-like immunoreactivity (TLI) assay is a highly sensitive and specific test and should be used for the diagnosis of EPI. This assay measures trypsinogen, some of which normally leaks from the pancreas into the blood, thereby providing an indirect assessment of functional pancreatic tissue. In EPI, functional exocrine tissue is severely depleted, and serum TLI concentrations are extremely low, clearly distinguishing EPI from other causes of malabsorption. This test requires a serum sample obtained after 12 hours of food withholding. Species-specific canine and feline TLI tests are available.
Hypoadrenocorticism and atypical hypoadrenocorticism in dogs can be ruled out by finding a basal cortisol > 55 nmol/L, or by an ACTH stimulation test.
Hyperthyroidism in cats should be excluded by measuring serum total T4 concentrations.
Serological tests for feline leukemia and feline immunodeficiency viruses should also be performed in cats, not only because both can be associated with secondary, chronic diarrhea but also because they are important prognostic factors.
Imaging in Malabsorption Syndrome
Radiography and ultrasonography should be considered complementary.
When indicated by clinical signs or abnormal abdominal palpation, plain radiography is used to identify surgical conditions and to provide clues as to the nature of any small intestinal disease. Abdominal radiography can identify foreign bodies, intestinal obstructions, and masses but is most useful when vomiting is present or palpable abnormalities are detected.
CT provides greater detail of all abdominal structures but is often not available.
Ultrasonography is an important part of the investigation of most small intestinal diseases. Changes consistent with pancreatitis may be observed ultrasonographically; however, failure to find a pancreas is an unreliable way to diagnose EPI. Ultrasonography can measure intestinal wall thickness, layering, and luminal diameter and detect other intestinal lesions (eg, masses, intussusception), mesenteric lymphadenopathy (in neoplasia and inflammatory enteropathies), and abnormalities in other organs. A thickened small intestinal wall with loss of layering is concerning for neoplasia. Mucosal striations have been associated with lymphatic dilatation.
Serum Folate and Cobalamin in Malabsorption Syndrome
The assay of serum folate and cobalamin (vitamin B12) concentrations can be a helpful initial test in the assessment of small intestinal disease. Folate is absorbed primarily by the proximal small intestine (jejunum), whereas cobalamin is absorbed by the distal small intestine (ileum). As a result, serum folate concentrations can be decreased in proximal small intestinal diseases, serum cobalamin concentrations can be decreased in distal small intestinal diseases, and both can be decreased in diffuse enteropathies.
Additionally, dysbiosis can result in concurrent hypocobalaminemia and hyperfolatemia due to utilization of cobalamin and production of folate by intestinal bacteria. Other factors (eg, the severity, extent, and duration of a mucosal abnormality; dietary intake; and vitamin supplementation) also influence these concentrations.
Hypocobalaminemia is particularly associated with IBD and alimentary lymphoma and results in metabolic changes, including methylmalonic acidemia, that can lead to anorexia. Subnormal cobalamin concentrations are an indication for supplementation.
Markers of Protein-Losing Enteropathies and Small Intestinal Inflammation in Malabsorption Syndrome
IV administration of51Cr-labeled albumin (or 51CrCl3 to label endogenous albumin) has been used historically to document PLE in dogs. Measurement of 3-day fecal excretion of this radioactive marker provides an estimation of labeled albumin and hence protein loss into the intestinal lumen. However, its use is very limited because of the need for a radioactive marker.
An alternative approach is the measurement of alpha-1 proteinase inhibitor in the feces. This plasma protein is lost into the intestinal lumen together with albumin, but unlike albumin, it is an antiproteinase and is excreted in the feces essentially intact. Species-specific assays have been developed; however, only a canine assay is available and only in the US. Three fresh fecal samples passed by spontaneous evacuation are required; any GI bleeding invalidates the result.
Intestinal inflammation may be identified indirectly by increases in serum C-reactive protein. A more specific test that measures fecal calprotectin is not readily available.
In many situations these tests are not performed, and PLE is suspected based on the presence of panhypoproteinemia in an animal with suspected GI disease, when other causes of hypoalbuminemia (such as protein-losing nephropathy or liver dysfunction) have been ruled out.
Empirical Treatment Trials in Malabsorption Syndrome
Intestinal biopsy often identifies chronic inflammatory enteropathies but rarely the cause of the inflammation. Although it may be idiopathic (ie, IBD) and require immunosuppression, parasitic infections, diet-responsive enteropathies, and antibiotic-responsive diarrhea may show similar histological changes. Therefore, sequential empirical antiparasitic trials (ie, a 3-day course of fenbendazole at 50 mg/kg, PO, every 24 hours) and diet trials are indicated before biopsy if there are no criteria of concern.
To avoid inappropriate use of antimicrobials and the development of resistance, empirical antimicrobial trials before biopsy are reserved for those patients in whom antibiotic-responsive diarrhea (ARD) is suspected (eg, young German Shepherd Dogs). Additionally, other methods of modulating the microbiota (eg, through diet, probiotics, and potentially fecal microbiota transplantation [FMT]) may be considered instead of antimicrobials. Anorexia, abnormal abdominal palpation and/or imaging, severe hypoproteinemia, and GI bleeding are all indications to proceed to biopsy.
For an exclusion diet trial, hydrolyzed diets or novel protein diets are often preferred to easily digestible diets; remission is achieved more frequently, and time to relapse is longer. However, hydrolyzed diets may be less palatable, not balanced for growth in young animals, and not in a palatable formulation (many are dried kibble). Curiously, follow-up studies after successful clinical resolution with a hydrolyzed diet do not show resolution of histological changes.
Intestinal Biopsy in Malabsorption Syndrome
Definitive diagnosis of some chronic small intestinal diseases (such as IBD) ultimately includes histological examination of intestinal biopsies taken by endoscopy or at laparotomy. However, if there is clinical remission with a prior empirical treatment trial, biopsy is not justified.
Histological examination of intestinal biopsy specimens can identify morphological changes of intestinal inflammation (including lymphocytic-plasmacytic enteritis and eosinophilic enteritis), intestinal lymphangiectasia, villous atrophy, and intestinal neoplasia. The description of morphological abnormalities can provide a baseline to evaluate response to treatment if sequential biopsies are possible, although resolution of changes does not always follow clinical remission. Morphological abnormalities may also provide prognostic information, because more severe enteropathies tend to be more difficult to manage.
Endoscopy is minimally invasive and allows visualization of the mucosa and targeted biopsy sampling (see images of small intestines, and with ). However, endoscopic mucosal biopsies cannot give an adequate representation of deeper disease and are limited to the parts of the small intestine (duodenum, ileum) that can be visualized via gastroscopy and colonoscopy. Endoscopic biopsy is preferred initially because the risk of intestinal surgical wound dehiscence can exceed 10% in debilitated, malnourished, or hypoproteinemic patients.


Endoscopic image of normal small intestine showing individual villi.
Courtesy of Dr. Edward J. Hall.

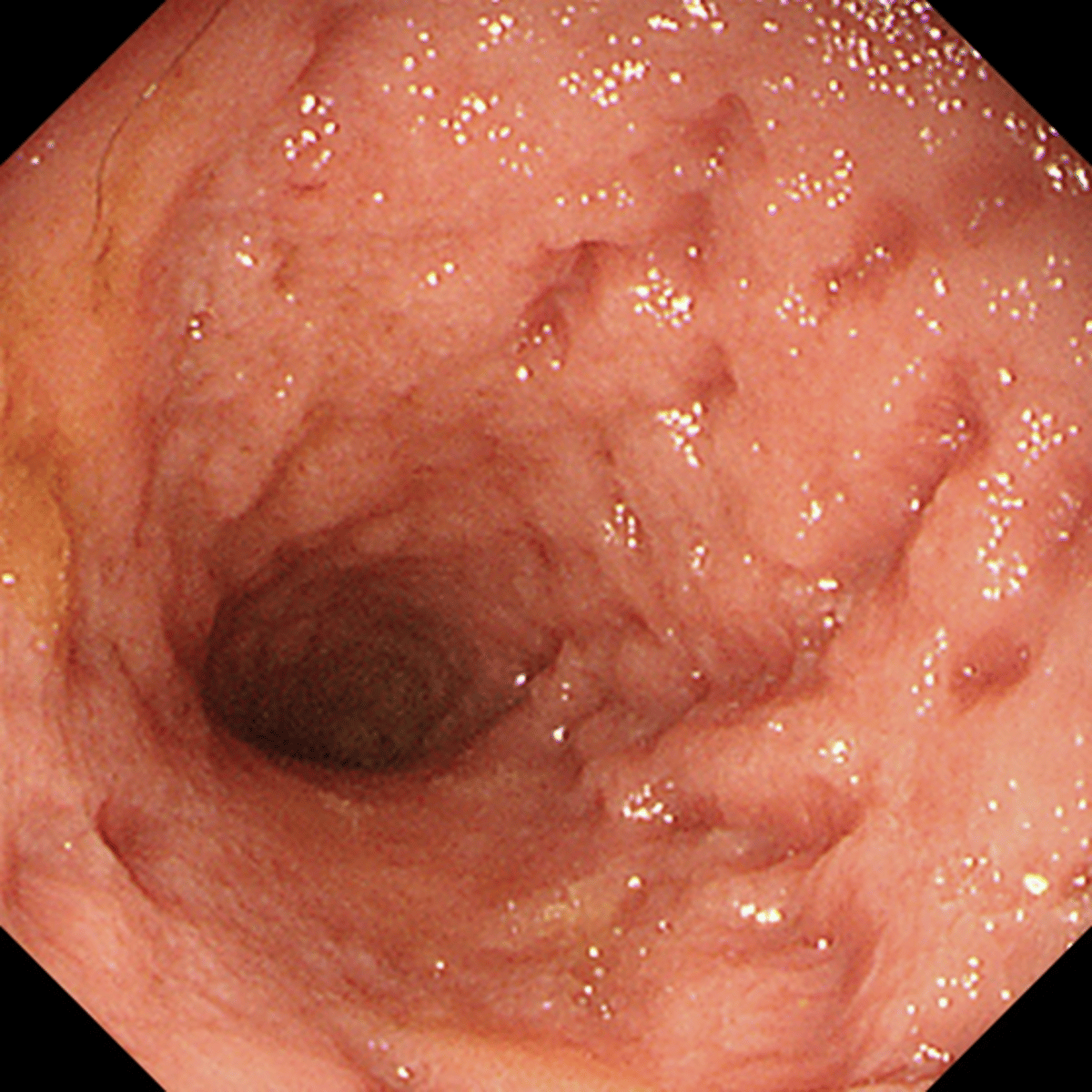
Endoscopic image of lymphoplasmacytic enteritis in a dog with malabsorption.
Courtesy of Dr. Edward J. Hall.
Surgery is the preferred option when there is a concern about deeper or extraintestinal disease or a focal lesion has been identified. Due to the risks associated with enterotomies, empirical treatment trials are usually performed first unless a surgical condition (eg, a focal lesion, partial obstruction) has been identified by palpation or imaging. If a laparotomy is performed and a gross focal lesion is not present, multiple elliptical, longitudinal biopsy samples should be collected from the duodenum, jejunum, and ileum; mesenteric lymph nodes should be biopsied and other organs examined.
However, certain malabsorptive disorders may display minimal or no obvious abnormalities, despite considerable interference with intestinal function. Nevertheless, histological descriptions alone provide little information, such as possible etiology or underlying mechanisms of damage that would assist with effective management and determination of prognosis. Furthermore, inconsistency in histological descriptions between pathologists is a recognized problem in achieving a definitive diagnosis. However, the World Small Animal Veterinary Association GI Standardization Group has published a descriptive template as a basis for concordance (1).
Treatment of Malabsorption Syndromes in Small Animals
Treat primary disorders (eg, EPI if present)
Add diet changes if needed and address complications
Treatment of malabsorption involves treatment of the primary cause (if identified) in conjunction with dietary therapy, modification of the microbiome (prebiotics, probiotics, and dietary manipulation) and management of any complications (eg, cobalamin supplementation for hypocobalaminemia).
Dietary Modification in Malabsorption Syndrome
Supportive Care in Malabsorption Syndrome
Probiotics and prebiotics. Prebiotics are digestible fibers that encourage the growth of a healthy microbiome. Probiotics are live organisms that confer a health benefit to the host when administered in adequate amounts. Evidence for the efficacy of probiotics in chronic enteropathies is largely lacking; however, hypothetically they help restore a normal microbiome and decrease intestinal inflammation.
Cobalamin and folate supplementation. See treatment and control of chronic enteropathy.
Antidiarrheals. Oral kaolin- and pectin-based suspensions can help solidify diarrhea but only treat clinical signs. Similarly, opioids (eg, loperamide) only provide temporary relief of clinical signs by modifying motility and decreasing small intestinal secretion. Note that loperamine should not be used in dogs with known ABCB1-delta genetic polymorphisms (Collies, Shetland Sheepdogs, Australian Shepherds).
Specific Treatments in Malabsorption Syndrome
Effective treatment of EPI and small intestinal disease depends on the nature of the disorder; however, therapy may be empirical when a specific diagnosis hasn't been made.
Exocrine pancreatic insufficiency: Management of EPI in dogs is relatively straightforward and includes dietary modification and replacement of pancreatic enzymes with exogenous enzymes.
Feeding a low-fiber diet that contains moderate levels of fat or highly digestible fat, very digestible carbohydrate, and high-quality protein is often recommended. Yet in many dogs and most cats, a standard, good-quality commercial diet is adequate. Diets that are highly digestible and low-residue are often used.
Treatment of EPI in dogs will require lifelong supplementation of each meal with pancreatic extract. Powdered extracts (1 tsp/10 kg) are preferable to tablets, capsules, and most enteric-coated preparations and should be mixed in food, not administered directly to the oral cavity, because these supplements will cause mucosal erosion. Fresh or fresh-frozen pancreas can be used as an alternative (100 g/meal for an adult German Shepherd Dog). However, raw products may be contaminated with bacterial pathogens and other infectious agents.
Pearls & Pitfalls
|
Treatment of EPI in cats is similar to that in dogs, but cyanocobalamin supplementation is almost invariably required.
The response to pancreatic enzyme replacement therapy may be poor, and adjunctive treatments may be necessary:
Secondary dysbiosis may be suspected. Concurrent treatment to address dysbiosis, including probiotics and/or FMT, could be considered
Acid suppressants (eg, H2-receptor blockers, such as cimetidine or ranitidine; proton pump inhibitors, such as omeprazole) may be given 20 minutes before a meal to inhibit acid secretion and minimize acid degradation of enzymes in the pancreatic extract; however, these products are expensive, and their value is questionable.
Serum cobalamin concentrations are commonly decreased in dogs and cats with EPI. Cobalamin supplementation (SC or PO) can be administered.
IBD: See treatment and control of chronic enteropathy.
Lymphangiectasia: See treatment and control of chronic enteropathy.
Infectious causes: Giardiasis can be treated with metronidazole or fenbendazole, and histoplasmosis treated with appropriate antifungal treatment (such as itraconazole with or without amphotericin B).
Intestinal neoplasia: Treatment of alimentary lymphoma involves an appropriate chemotherapy regimen; however, response is very poor in dogs and poor in cats with lymphoblastic forms. In cats, treatment of small cell villous lymphoma with oral prednisone and chlorambucil has been associated with prolonged remission.
Solid tumors of the small intestine (eg, adenocarcinoma) more typically produce clinical signs of intestinal obstruction and bleeding with diarrhea rather than malabsorption. They are managed primarily by surgical resection.
Prognosis for Malabsorption Syndromes in Small Animals
The prognosis in cases of malabsorption is good if there is a simple solution (eg, in a retrospective study, 60% of cases of EPI responded well to enzyme replacement therapy and 17% had a partial response) (2, 3). A poorer prognosis has been associated with severe intestinal inflammation, neoplastic disease, severe weight loss, hypoalbuminemia and ascites (PLE), anorexia, elevated pancreatic lipase concentration, and hypocobalaminemia. More than 50% of dogs with PLE are reported to be deceased within 12 months of diagnosis (4, 5, 6).
Key Points
Malabsorption is caused by exocrine pancreatic or small intestinal disease and results in diarrhea and weight loss even if polyphagia occurs.
History, physical examination, and a minimum laboratory database help rule out non-GI causes of diarrhea.
Pancreatic insufficiency, hypoadrenocorticism in dogs, and hyperthyroidism in cats should be ruled out before investigating small intestinal disease directly.
Serum folate and cobalamin deficiencies are markers of small intestinal disease and indications for vitamin supplementation.
A hydrolyzed diet trial is recommended before intestinal biopsy if the patient is eating and not unwell.
For More Information
Global nutrition guidelines. World Small Animal Veterinary Association.
Comparative Gastroenterology Society. Texas A&M Veterinary Medicine & Biomedical Sciences.
Also see pet owner content regarding malabsorption in dogs, cats, and horses.
References
Washabau RJ, Day MJ, Willard MD, et al. Endoscopic, biopsy, and histopathologic guidelines for the evaluation of gastrointestinal inflammation in companion animals. J Vet Intern Med. 2010;24(1):10-26. doi:10.1111/j.1939-1676.2009.0443.x
Cridge H, Williams DA, Barko PC. Exocrine pancreatic insufficiency in dogs and cats. J Am Vet Med Assoc. 2023;262(2):246-255. doi:10.2460/javma.23.09.0505
Batchelor DJ, Noble PJ, Taylor RH, Cripps PJ, German AJ. Prognostic factors in canine exocrine pancreatic insufficiency: prolonged survival is likely if clinical remission is achieved. J Vet Intern Med. 2007;21(1):54–60. doi:10.1892/0891-6640(2007)21[54:pficep]2.0.co;2
Allenspach K, Iennarella-Servantez C. Canine protein losing enteropathies and systemic complications. Vet Clin North Am Small Anim Pract. 2021;51(1):111-122. doi:10.1016/j.cvsm.2020.09.010
Craven MD, Washabau RJ. Comparative pathophysiology and management of protein-losing enteropathy. J Vet Intern Med. 2019;33(2):383-402. doi:10.1111/jvim.15406
Allenspach K, Rizzo J, Jergens AE, Chang YM. Hypovitaminosis D is associated with negative outcome in dogs with protein losing enteropathy: a retrospective study of 43 cases. BMC Vet Res. 2017;13(1):96. doi:10.1186/s12917-017-1022-7





