

The first step in wound management should be an assessment of the overall stability of the animal. Obvious open wounds can distract attention from more subtle but potentially life-threatening problems (eg, shock).
Pearls & Pitfalls
|
After initial assessment, the patient should be stabilized.
First aid for the wound should be performed as soon as safely possible. Active bleeding can be controlled with direct pressure. A pneumatic cuff or pressure wrap, instead of a tourniquet, should be used in cases of severe arterial bleeding; the cuff should be inflated until hemorrhage is controlled. Use of a cuff or pressure wrap helps avoid neurovascular complications that can be associated with narrow tourniquets.
Treatment for any local wound should be guided by the fundamentals of debridement, infection or inflammation control, and moisture balance. The wound must be protected from further contamination or trauma by covering it with a sterile, lint-free dressing. The delay between examination and definitive debridement should be minimized to decrease bacterial contamination.
If the wound is infected, a sample should be collected for bacteriologic culture and antimicrobial susceptibility testing. Antimicrobial treatment should be instituted in all cases of dirty, infected, or puncture wounds. A broad-spectrum bactericidal antimicrobial (eg, a first-generation cephalosporin) is generally recommended pending culture results.
Analgesia is indicated for pain relief.
Wound Lavage in Small Animals
Wound lavage serves two purposes.
Irrigation of the wound washes away both visible and microscopic debris. This decreases the bacterial load in the tissue, which helps decrease wound complications.
The lavage also allows better examination of underlying tissues.
Assuming the solution is nontoxic, the most important factor in wound lavage is use of large volumes to facilitate removal of debris.
Wound lavage is most effective when delivered under appropriate pressure. Low-pressure systems, such as a bulb syringe, are adequate in clean wounds. Higher pressures are used in dirty or contaminated wounds. A recommended lavage system delivering 48–55 kPa (7–8 psi) of pressure can be fashioned with a 35-mL syringe and a 19-gauge needle. Excessive pressure can cause adverse effects by driving debris deeper into the healthy tissue.
The use of antimicrobials in the lavage fluid is controversial.
The ideal lavage fluid should be antiseptic and nontoxic to the healing tissues. Saline (0.9% NaCl) solution is the least toxic to healing tissue, although it is not antiseptic. Surgical scrub agents should not be used because the detergent components are damaging to tissue. Dilute antiseptics can be used safely.
Chlorhexidine diacetate (0.05%) has sustained residual activity against a broad spectrum of bacteria while causing minimal tissue inflammation. However, gram-negative bacteria may become resistant to chlorhexidine. Stronger solutions of chlorhexidine are toxic to healing tissue.
Povidone-iodine is an effective antiseptic; however, it has minimal residual activity and may be inactivated by purulent debris.
Although an effective antiseptic, hydrogen peroxide is toxic to healthy tissue and should not be used for lavage of wounds.
Surgical Debridement in Small Animals
After wound preparation and hair removal, surgical debridement (removal of nonviable tissue and foreign debris) can be performed. Debridement may involve nonselective removal of large segments of tissue or may be performed more selectively, enabling preservation of specific tissues.
Skin and local tissue viability should be assessed before any attempted debridement. Skin that is blue-black, leathery, thin, or white is usually not viable. This necrotic tissue should be sharply excised. The debridement may be done in layers or as one complete section of tissue (en bloc resection).


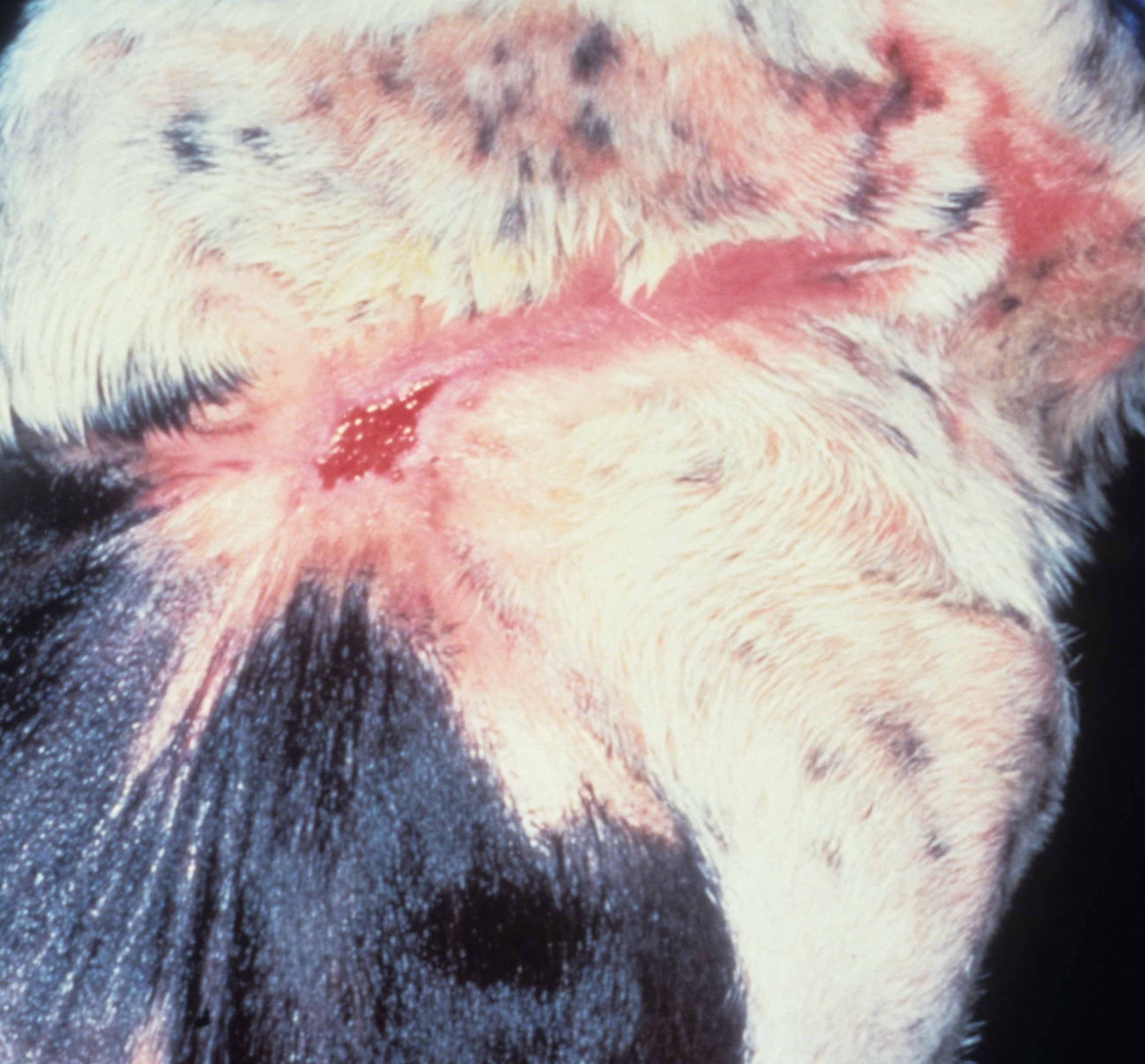
Thermal burn injury in a 2-year-old Chihuahua.
Courtesy of Dr. Kevin Winkler.

Postsurgical debridement of a 2-year-old Chihuahua with a thermal burn injury.
Courtesy of Dr. Kevin Winkler.
Tissues that have questionable viability or are associated with essential structures such as neurovascular bundles should be treated conservatively. Staged debridement is indicated in some situations.
In addition to sharp dissection, debridement may be autolytic, mechanical (eg, bandage debridement), enzymatic, or biological (maggot therapy).
Selective trimming of viable tissue at wound edges (ie, "freshening the edges") is generally not indicated in acute wound management, although it may facilitate wound closure when the shape of the wound makes closure difficult.
Wound Closure in Small Animals
After initial inspection, lavage, and debridement, a veterinarian must decide whether to close the wound or to manage it as an open wound. Considerations include the availability of skin for closure, wound location, and level of contamination or infection.
Although primary closure is the simplest method of wound management, it should be used only in appropriate situations to avoid wound complications. Wounds may be closed with suture, staples, or cyanoacrylate.
Clean wounds that are properly debrided usually heal without complication. With a primary closure, the layers should be individually closed to minimize “dead space” that might contribute to seroma formation. The types of suture and suture patterns used depend on surgeon preference, the size of the wound, the location of the wound, and the size of the animal.
Primary closure may not be appropriate for a grossly contaminated or infected wound. Therefore, if closure is the goal, it may be delayed until the contamination or infection is controlled. The wound can be managed short-term as an open wound until it appears healthy. At that time, the wound can be safely closed with minimal risk of complications.
The time between initial debridement and final closure varies according to the extent of contamination or infection. Minimally contaminated wounds may be closed after 24–72 hours. Longer periods may be required for heavily infected wounds.
Wounds closed > 5 days after the initial wounding are considered to be secondary closure. This implies that granulation tissue has begun to form in the wound before closure.
Open Wound Management in Small Animals
When a wound cannot or should not be closed, open wound management (ie, second-intention healing) is appropriate. Such wounds include those in which there has been a loss of skin that makes closure impossible and those that are too grossly infected to close. Longitudinal degloving injuries of the extremities are especially amenable to open wound management.
If the wound is left open, it should be managed for optimal healing.

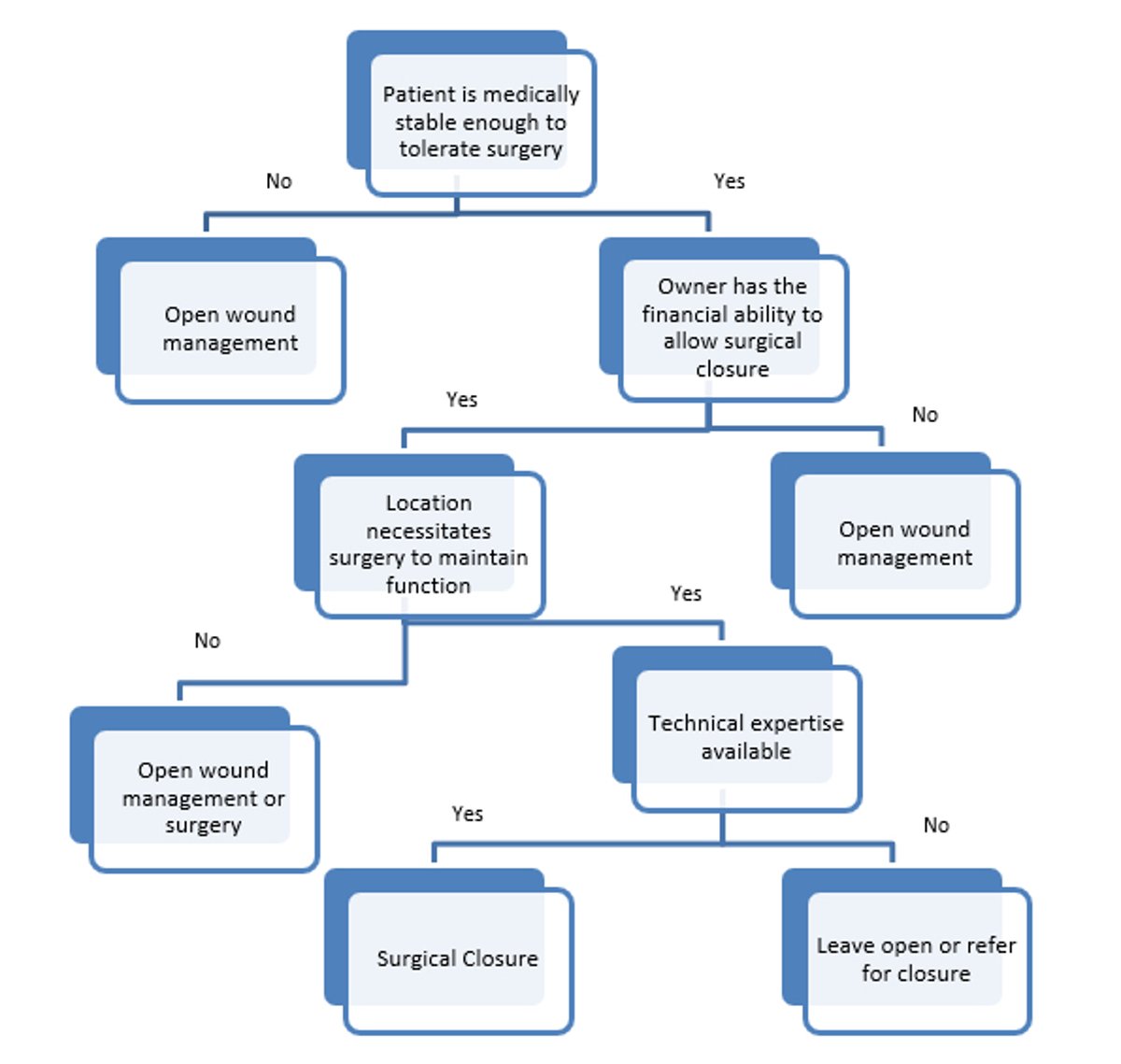
Decision tree diagram used to determine appropriate type of wound management. Options for wound management are closure (ie, primary or secondary wound closure) and open wound management (second-intention healing).
Courtesy of Dr. Kevin Winkler.


Open wound management over the shoulder in an 11-month-old German Shorthaired Pointer.
Courtesy of Dr. Kevin Winkler.

Progressive wound contracture resulting in loss of range of motion in the shoulder.
Courtesy of Dr. Kevin Winkler.
Open wound management enables progressive debridement procedures and does not require specialized equipment (such as may be needed with skin grafting). However, it increases cost, prolongs time for healing, and may create complications from wound contracture.
Open wound management is based on repeated bandaging and debridement as needed until the wound heals. Traditional open wound management calls for wet adherent (wet-to-dry) dressings initially. The initial wide-mesh gauze dressings help with mechanical debridement at every bandage change.
Until a granulation bed forms, the bandage should be changed at least once daily. In the early stages of healing, the bandage may need to be changed as often as twice daily. After granulation tissue develops, the bandage should be changed to a dry, nonadherent dressing so the granulation bed is not disrupted. Both the granulation bed and the early epithelium are easily damaged, and disruption of the granulation bed delays wound healing.
With the concept of moist wound healing, bandaging is combined with autolytic debridement to promote wound healing. The use of moist wound dressings keeps white cells healthier, allowing them to aid in the debridement process. A variety of dressings are available. With these newer dressing options, some consider traditional wet-to-dry dressings to be outdated.
A decision to use open wound management or delayed wound closure is based on several factors:
patient morbidity
cost
wound location
technical expertise required for closure
In certain patients, surgery may not be an option given their health status. For those patients, open wound management is a better choice.
Although the initial cost of surgery is higher than bandage changes, the overall cost may be lower, depending on the nature and length of wound care required without surgical intervention.
Wound location also has a major impact on the decision to surgically intervene. As the open wound heals, contracture of the wound begins to occur. Contracture of a wound on the lateral thorax may not result in any longterm complications. However, a wound spanning or adjacent to a joint may result in loss of longterm joint function or range of motion due to scarring. To avoid this loss of function, the wound should be surgically closed.
Another component of decision-making in these cases relates to the clinician's abilities. If the techniques required for closure exceed the clinician's expertise, referral to another location for closure is advisable to avoid unnecessary complications.
Finally, the owner may have a specific request regarding cosmesis. Closure with open wound management will result in a hairless scar. For various reasons, this may not be acceptable. In those cases, surgical intervention is required.
Key Points
Stabilizing injured patients should take priority over wound management.
Wounds should be irrigated (lavage), with an appropriate solution at appropriate pressure, to remove contamination (bacteria and debris) and improve visibility for wound inspection.
Surgical debridement removes nonviable tissue.
Options for wound management are closure (which may be primary or secondary) and open wound management (second-intention healing).
For More Information
Dycus D, Wardlaw J. Helpful tips for managing wounds in veterinary patients. Today's Vet Pract. Nov/Dec 2013:32-36.
Nagle SM, Stevens KA, Wilbraham SC. Wound Assessment. StatPearls Publishing. 2022. [Updated 2022 Oct 19]. https://www.ncbi.nlm.nih.gov/books/NBK482198/
Also see pet health content regarding initial wound management.





