

Blastomycosis is a multifocal fungal infection due to the dimorphic fungi Blastomyces spp. The fungi are often found in soil or decomposing organic matter, such as leaves. Infection is characterized by pyogranulomatous lesions in various tissues, most frequently the lungs or skin.
Species causing infection include Blastomyces dermatitidis, B gilchristii, and B helices. Blastomycosis affects some species but not others:
Most commonly affected: dogs, humans
Less commonly diagnosed: cats, horses, ferrets, deer, many wildlife species
Not reported to be susceptible: cattle, sheep, pigs
Blastomycosis, sometimes called "blasto," is most often diagnosed in North America but has been reported from most continents. While humans can get blastomycosis, they do not acquire infection from animals. Instead, both animals and humans acquire infection from the environment.
Most cases have occurred in:
River basins: Mississippi, Missouri, Tennessee, and Ohio rivers
Great Lakes
St. Lawrence Seaway
Pacific Northwest
Even within these regions, the organism is found in geographically restricted areas. Beaver dams and other habitats where soil is moist, acidic, and rich in decaying vegetation may serve as the ecologic niche for the organism; however, it is often difficult to find in the environment. Most dogs with blastomycosis live within 400 m of a waterway. In the environment, the fungus grows in saprophytic mycelial form and produces conidia.
Rain, dew, or fog may play a critical role in liberating the infective conidia, which are then aerosolized and inhaled. When respiratory defenses are overwhelmed or immunosuppressed, disseminated disease occurs via hematogenous spread from the lungs.
Cutaneous lesions may result from a primary entry via the skin or, more commonly, by dissemination from a pulmonary focus. Needle-stick injuries to veterinary personnel after aspiration of cutaneous lesions from infected patients have resulted in primary cutaneous infection.
Clinical Signs of Blastomycosis in Animals

Courtesy of Ontario Veterinary College.
The clinical signs of blastomycosis vary with organ involvement and are not specific:
weight loss
cough
anorexia
lymphadenopathy
dyspnea
ocular disease
lameness
skin lesions
fever
Young adult large-breed dogs are predisposed; extensive outdoor use (eg, hunting) is another predisposing factor. Inhaled conidia transform into yeasts that resist neutrophil inactivation and create pyogranulomas in the lung. Yeasts may disseminate via blood or lymphatics.

Courtesy of Dr. Dae Young Kim.
Dry, harsh lung sounds from lung lesions are common in dogs with blastomycosis. Clinical signs of pulmonary involvement occur in as many as 85% of affected dogs. Severe pulmonary involvement results in hypoxemia, which indicates a poor prognosis.
Lymph node involvement is evident in approximately half of affected dogs, which is about the same proportion of dogs that have cutaneous involvement. Lung lesions may resolve by the time disseminated or cutaneous involvement is noted.
Skin lesions may include proliferative granulomas and subcutaneous abscesses that ulcerate and drain a serosanguineous discharge. The skin lesions are often very small and multifocal in dogs. The planum nasale, face, and nail beds are most often involved.
Clinical signs of ocular blastomycosis are present in 30%–50% of affected dogs and include blindness, uveitis, glaucoma, and retinal detachment. Lameness associated with fungal osteomyelitis or severe paronychia occurs in approximately one-quarter of affected dogs. CNS signs are uncommon, occurring in < 5% of dogs, but they may be more common in cats. Hematuria and dysuria may be present with urogenital blastomycosis.
The pattern of systemic involvement is similar in cats, but cats are affected far less commonly than dogs. Large cutaneous abscesses may occur in cats.
Lesions
Gross lesions consist of few to numerous, variable-sized, irregular, firm, gray to yellow areas of pulmonary consolidation and nodules in the lungs and thoracic lymph nodes. Dissemination may result in nodular lesions in various organs but especially the skin, eyes, and bone. Cutaneous lesions are single or multiple papules, or chronic, draining, nodular pyogranulomas.
Diagnosis of Blastomycosis in Dogs and Cats
Identification of yeasts in tissue impressions, fine needle aspirates, fluids, or biopsies
Antigen testing of urine is sensitive; may cross-react with Histoplasma
Blastomycosis should be considered in dogs with draining cutaneous nodules and clinical signs of respiratory disease. In cats, respiratory tract involvement occurs most frequently, followed by involvement of the CNS, regional lymph nodes, skin, eyes, and GI and urinary tracts.
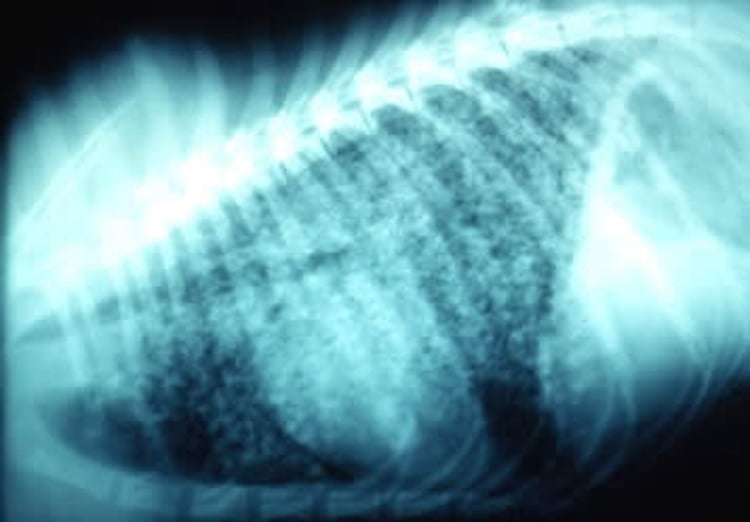
Radiographic findings in the lungs include noncalcified nodules or consolidation, with enlargement of the bronchial and mediastinal lymph nodes. The predominant patterns on thoracic radiographs are those of diffuse nodular interstitial and peribronchial densities. Commonly, the bronchial lymph nodes are greatly enlarged and appear in radiographs as dense masses.
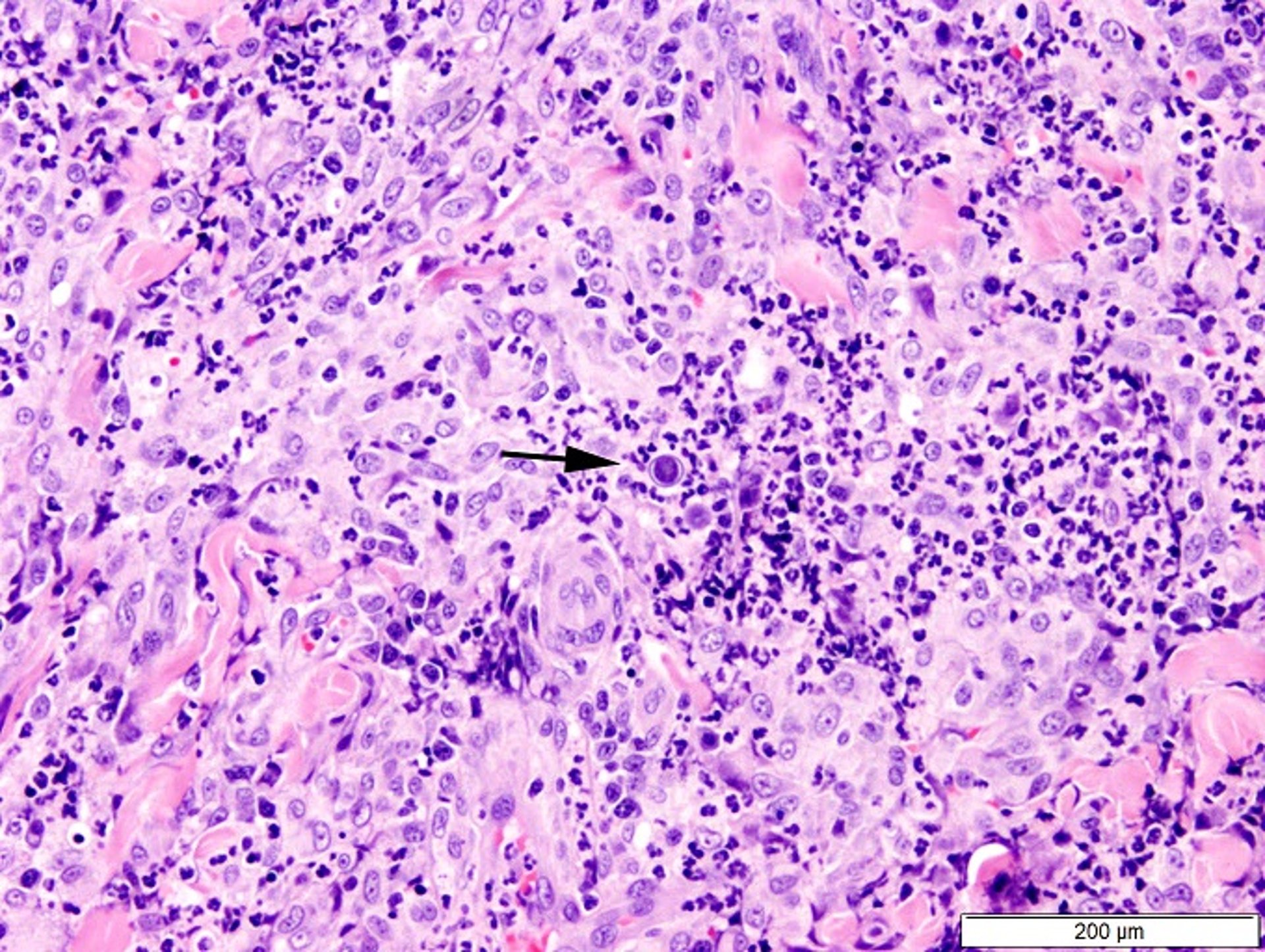
Diagnosis can be made from biopsy of tissue or aspirated specimens taken from cutaneous lesions or other involved organs by the presence of thick-walled yeasts that often have daughter cells budding from a broad base. These round to ovoid, pale pink (H&E) blastospores measure 8–25 mcm and have a refractile, double-contoured wall. They may be empty or contain basophilic nuclear material and have single, broad-based buds. An antibody response, detected by agar gel immunodiffusion, usually occurs; however, this response is neither sensitive nor specific when attempting to make a definitive diagnosis.
An enzyme immunoassay for antibodies against recombinant Blastomyces adhesin-1 repeat antigen(rBAD-1) has shown improved sensitivity; however, the most sensitive assay is antigen immunoassay of urine, which detects cell wall galactomannan. This test is highly sensitive for fungal infection but can cross-react with Histoplasma antigens.
Treatment of Blastomycosis in Dogs and Cats
Itraconazole (5 mg/kg, PO, once daily, long-term treatment)
Recurrence of disease in approximately 1 in 5 dogs
Itraconazole (5 mg/kg every 24 hours) is the treatment of choice for dogs and cats with blastomycosis. A minimum of 3 months of treatment is necessary, and the drug should be continued until active disease is not apparent. Clinical cure can be expected in ~70% of dogs, with recurrence months or years after treatment noted in ~20% of treated dogs.
Most dogs will respond to retreatment with itraconazole. Other azoles such as fluconazole and ketoconazole are not as effective as itraconazole; however, a study evaluating cost-effectiveness of fluconazole showed it to be a less expensive alternative, despite longer treatment times.
In fulminating cases of blastomycosis, especially those with evidence of hypoxemia, combination treatment with amphotericin B and itraconazole is recommended. Fifty percent of severely affected dogs may die during the first week of treatment. Short courses of anti-inflammatory dosages of glucocorticoids have been advocated during the first few days of treatment for dogs that develop more severe respiratory signs after starting treatment.
The prognosis is best for dogs with only mild lung disease, more guarded for dogs with moderate to severe lung disease, and poorest for dogs with CNS involvement. Treatment progress may be evaluated via serial urine antigen titers. Treatment is recommended to continue until two negative antigen test results are achieved 3–4 weeks apart. Radiographic changes may take months to years to resolve.
Key Points
Blastomycosis occurs after inhalation of conidia from the environment; pulmonary disease can progress to disseminated disease.
Observation of yeasts in tissue impressions, fluids, aspirates, or biopsies confirms the diagnosis; fungal antigen assays may also be of use.
Treatment is itraconazole and/or amphotericin B and must be continued for months; recurrence is common.





