

Arthritis is a nonspecific term denoting inflammation of a joint. All joint diseases of large animals have an inflammatory component to varying degrees. Arthritides of importance include traumatic arthritis, osteochondritis dissecans, subchondral bone cysts, cystic lesions, septic (or infective) arthritis, and osteoarthritis (also called degenerative joint disease).
Traumatic Arthritis
Traumatic arthritis includes traumatic synovitis and capsulitis, major intra-articular fractures, small osteochondral (chip) fractures, cartilage trauma, ligamentous tears (sprains) involving periarticular and intra-articular ligaments, and meniscal tears. Traumatic arthritis occurs primarily in athletic horses, but it can occur in all breeds of horses and all species of large animals. Unresolved traumatic arthritis often results in the development of osteoarthritis.
Clinical Findings and Diagnosis of Traumatic Arthritis in Large Animals


Courtesy of Dr. Stephen Adams.
Clinical signs such as lameness, joint pain, and joint effusion
Radiographic and ultrasonographic evaluation
Traumatic synovitis and capsulitis is inflammation of the synovial membrane and fibrous joint capsule associated with trauma. Typical cases in equine athletes are associated with synovial effusion in the acute stage and with general thickening and fibrosis in the more chronic stage. Lameness varies from a mild gait change to severe lameness. Traumatic synovitis and capsulitis is differentiated from other traumatic entities by use of radiography to exclude fractures and ultrasonography to exclude ligament disease. Tearing of some ligaments or menisci (in femorotibial joints) can often be determined only by arthroscopy. Major fractures and osteochondral fractures are diagnosed by radiographic evaluation.
Clinical signs of osteochondral fractures are similar to those of synovitis and capsulitis as well as those of osteoarthritis; diagnosis is based on radiography, ultrasonography, and, in some cases, arthroscopy.
Treatment of Traumatic Arthritis in Large Animals
Rest, systemic and intra-articular anti-inflammatory drugs, and physical rehabilitation
Repair of major articular fractures; removal of smaller osteochondral fractures
Medical treatment. Treatment of acute traumatic synovitis and capsulitis includes rest and physical rehabilitation regimens such as cold water treatment, application of ice, passive flexion, and swimming. Orally or IV administered NSAIDs (eg, phenylbutazone) are used routinely and may reduce synovial inflammation. The US FDA prohibits all uses of phenylbutazone in female dairy cattle >20 months of age; the Food Animal Residue and Avoidance Databank (FARAD) has recommended a 55–60 day withdrawal interval following chronic oral administration (>10 days), and a minimum withdrawal interval of 55 days following IM administration in beef cattle.
Various drugs have been used for intra-articular administration. Corticosteroids are the most potent anti-inflammatory agents and are effective in acute traumatic arthritis. In horses, betamethasone and triamcinolone acetonide are effective and are not known to be associated with any detrimental effects, while methylprednisolone acetate is more potent and longer acting but may cause degenerative changes in the articular cartilage. Hyaluronate sodium has been used effectively for mild to moderate synovitis in horses and has a chondroprotective effect, but it is less effective in severe synovitis or when intra-articular fractures are present.
An IV formulation of hyaluronic acid appears to be effective in clinical cases as well as in a controlled model of arthritis in horses. Polysulfated glycosaminoglycans (PSGAGs) are also used frequently for traumatic arthritis in horses; PSGAGs are effective for synovitis and can help prevent ongoing degeneration of articular cartilage. Although the effectiveness of PSGAGs when administered intra-articularly (250 mg/joint, intra-articularly, every 7 days for 5 week) has been established, their effectiveness when administered IM (500 mg/horse, IM, every 4 days for 28 days) is less certain. Pentosan polysulfate (3 mg/kg, IM, every 7 days for 4 consecutive treatments) has been shown to be effective as a disease-modifying osteoarthritis drug (DMOAD) in experimental models of equine osteoarthritis and has been extensively used in clinical cases outside the US.
Biologic treatments such as autologous conditioned serum, platelet-rich plasma, and autologous protein solutions are also more commonly being used to control inflammation and aid healing.
Surgical treatment. Major intra-articular fractures (eg, third carpal bone slab fractures, proximal phalanx sagittal articular fractures, and distal metacarpal and metatarsal condylar fractures) that disrupt joint congruity should be repaired to avoid development of osteoarthritis. Horses with osteochondral chip fragmentation (occurring most commonly in the carpus and metacarpophalangeal [fetlock] joints) are treated with arthroscopic surgery to remove the fragments and minimize development of osteoarthritis. Fragments are removed and defective bone and cartilage debrided. Rest periods of 2–4 months follow, and physical rehabilitation regimens are instituted in the convalescent period. The success rate in returning horses to previous performance level is high when secondary osteoarthritic changes are minimal at the time of surgery. Osteochondral chip fragments that are amenable to arthroscopic surgery include those associated with the distal radius, carpal bones, dorsoproximal first phalanx, or proximal palmar or plantar first phalanx; apical, abaxial, and basilar fragments of the proximal sesamoid bones; fragmentation of the distal patella in the femoropatellar joint; chip fragments of the tibiotarsal joint; and fragments of the extensor process of the distal phalanx (coffin joint).
Osteochondrosis
Osteochondrosis (dyschondroplasia) is a focal defect in endochondral ossification. The disease may manifest as osteochondritis dissecans—which results in the formation of flaps of cartilage or cartilage and bone in the joint—or as subchondral bone cysts. Osteochondrosis has been described in pigs, horses, and cattle, among other species. For a discussion of equine osteochondrosis, see Osteochondrosis in Horses.
Osteochondritis Dissecans
Etiology
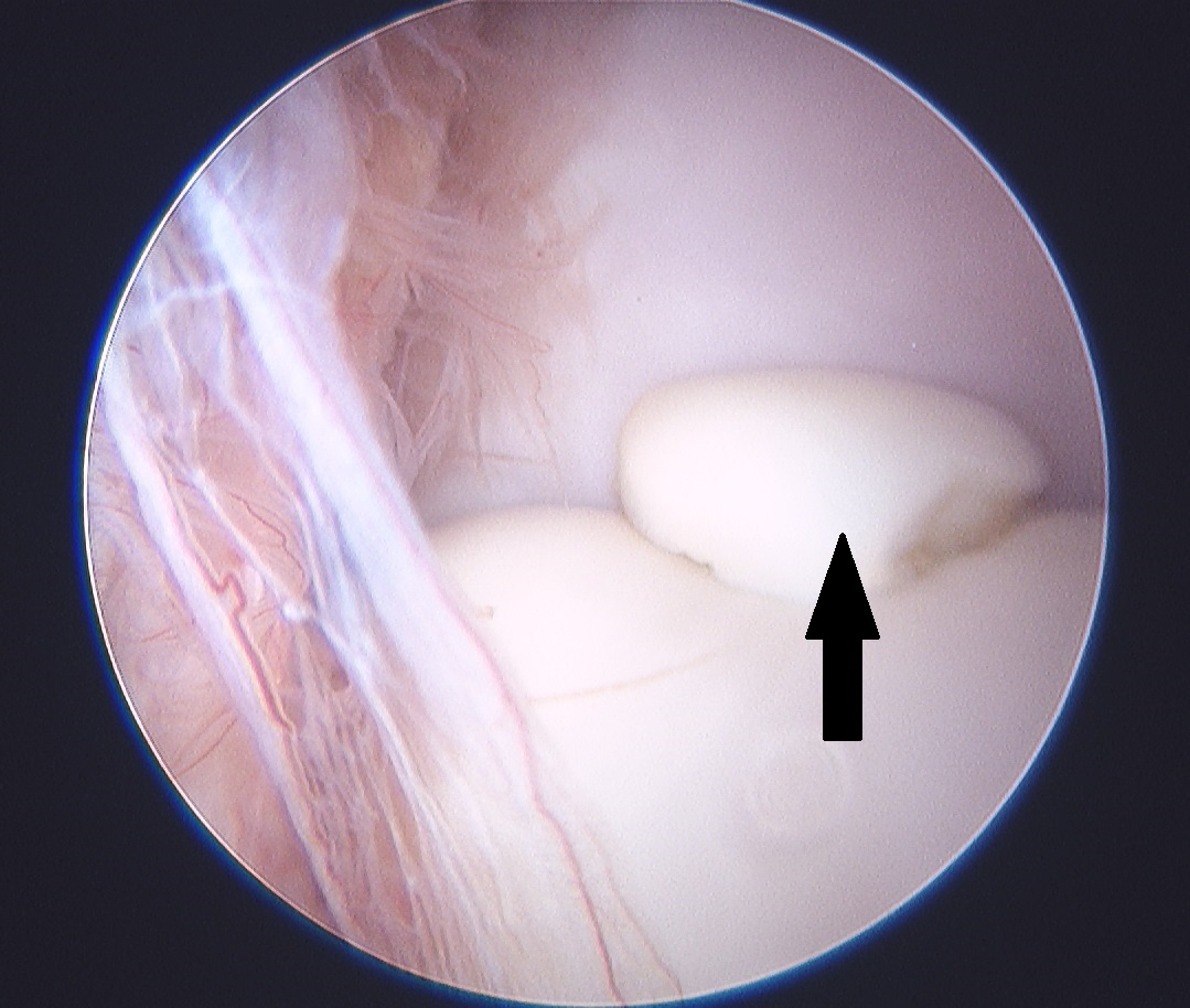
In osteochondritis dissecans (OCD), a focal area of the immature articular cartilage is retained, and the matrix in the basal area of this region becomes chondromalacic and acellular. The immature articular cartilage separates from the underlying trabecular bone. The chondral fracture extends horizontally and vertically until a flap is formed. Synovial fluid gains entrance to the underlying medullary space, and subchondral cysts may form (usually only in larger animals). The flap of immature articular cartilage may remain separated and loose, break away completely (the free-floating cartilage fragments are known as joint mice), or reattach by endochondral ossification to the underlying bone, especially in pigs, and result in a wrinkled articular surface. The latter occurs only if the joint is rested or protected, permitting reestablishment of the circulation necessary for endochondral ossification. If the flap is torn free by joint motion, it may be ground into smaller pieces during locomotion and disappear, whereas the larger plaques may become attached to the synovial membrane, become vascularized, and ossify. The resultant articular defect, in time, fills with fibrocartilage.
The exact cause of OCD is unknown but is assumed to be multifactorial. Risk factors include genetic predisposition, fast growth, high caloric intake, low copper and high zinc concentrations, endocrine factors, and trauma to the joint.
Clinical Findings
The most common sites of OCD, which usually occurs in young animals (< 1 year old), are the femoropatellar joint, tibiotarsal (tarsocrural) joint, fetlock (metacarpophalangeal and metatarsophalangeal) joints, and the shoulder.
Animals with OCD of the shoulder usually develop severe forelimb lameness and possibly some muscular atrophy. Animals with OCD in the other joints usually develop synovial effusion and varying amounts of lameness.
Diagnosis


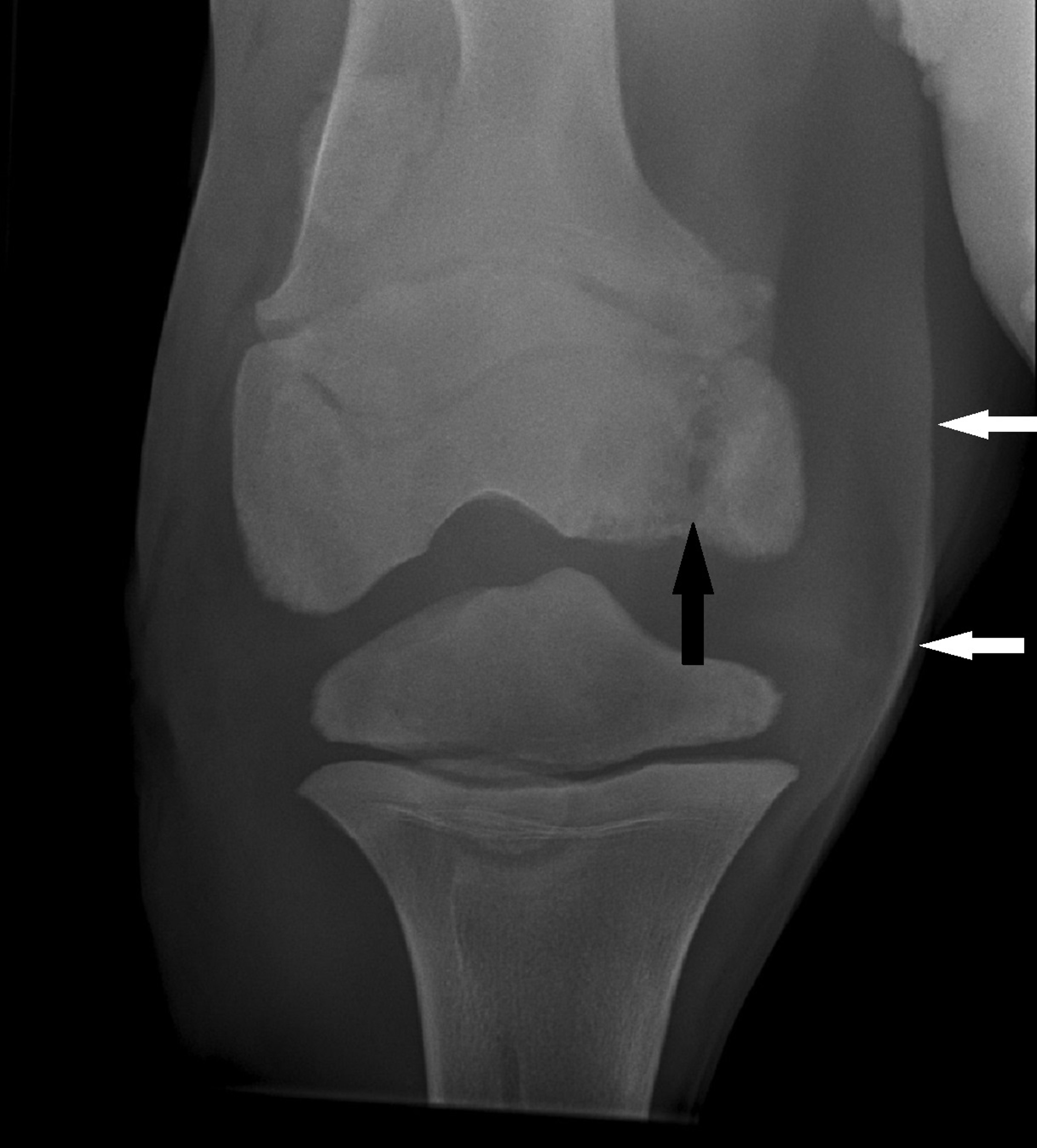
Courtesy of Dr. Stephen Adams.


Courtesy of Dr. Stephen Adams.
Diagnosis is confirmed by radiographic evaluation. The animal's history, age, breed, sex, and clinical signs provide useful information; however, radiographs are required to substantiate a diagnosis of OCD.
Treatment

Stephen Adams
Arthroscopic surgery to remove fragments of bone and cartilage
Treatment of OCD depends on the location and extent of involvement. Femoropatellar joint lesions are associated with the lateral trochlear ridge of the femur, medial trochlear ridge of the femur, or distal patella. They are amenable to arthroscopic surgery, which is recommended in all cases except early lesions characterized by flattening (without fragmentation) < 2 cm long on the lateral trochlear ridge. In the tarsocrural joint, OCD lesions occur in decreasing frequency on the intermediate (sagittal) ridge of the tibia, lateral trochlear ridge of the talus, medial malleolus of the tibia, and medial trochlear ridge of the talus. All lesions are amenable to arthroscopic surgery, and the prognosis is usually good. Surgery is recommended when synovial effusion is present. Lesions without fragmentation in the metacarpophalangeal or metatarsophalangeal joints can be treated conservatively, and most affected animals recover well. If a fragment is present, arthroscopic surgery is recommended. In the shoulder, surgery is usually recommended, although milder cases have been managed conservatively with success. The prognosis with arthroscopic surgery is generally less favorable in the shoulder than in other joints.
Subchondral Bone Cysts


Courtesy of Dr. Stephen Adams.
Most subchondral bone cysts are a manifestation of osteochondrosis; however, the cysts can be secondary to intra-articular trauma to cartilage or subchondral bone or secondary to osteoarthritis. Subchondral bone cysts in growing horses that are due to osteochondrosis occur most commonly in the medial femoral condyle in the femorotibial joint; however, they may also occur in the fetlock (metacarpophalangeal and metatarsophalangeal), pastern, elbow, shoulder, and proximal and distal interphalangeal joints in horses. Diagnosis is usually based on localization of lameness after a lameness examination, intra-articular analgesia, and confirmation by radiographic evaluation. Synovial effusion may or may not be present in the affected joint.
Treatment
In young horses, subchondral bone cysts secondary to osteochondrosis can be managed with pasture rest, intralesional corticosteroid injections guided by ultrasonography or done arthroscopically, or placement of a screw across the cyst. Some cysts will resolve with rest, and lameness can resolve in some horses in which the cyst remains. For cysts of the medial femoral condyle, arthroscopically guided intralesional injection of corticosteroids is often the choice for initial treatment. Athletic soundness is achieved in 65%–70% of these horses with medial femoral condyle cysts. However transcondylar screw placement has shown success and is now the treatment of choice of some surgeons. Smaller, dome-shaped or flattened lesions are usually treated conservatively in the initial period. When cystic lesions are found during arthroscopic surgery to have collapsed edges, or when cysts are unresponsive to other therapy, arthroscopic debridement augmented by fibrin, growth factors, and mesenchymal stem cells has been used. Surgery is usually recommended for subchondral cystic lesions of the distal metacarpus in the fetlock joint; however, exposure of the cyst can be difficult, and surgery is not done as consistently as in the femorotibial joint. Single lesions associated with the pastern and elbow joint may be treated conservatively, with intralesional corticosteroids or with screws across the cyst, and have a fair prognosis. If possible, surgery is recommended for cystic lesions of the distal phalanx (results with conservative treatment are very poor). Cysts in the distal aspect of the proximal phalanx in the rear limbs of horses often result in osteoarthritis of the pastern joint, and treatment by surgical arthrodesis of the joint can result in soundness.
Septic Arthritis
(Infective Arthritis, Suppurative Arthritis)
Etiology of Septic Arthritis in Large Animals
Septic arthritis (infective arthritis) results from sequestration of bacterial infection in a joint. Infection of a joint develops in three main ways: hematogenous infection, which is common in foals, calves, and lambs (commonly referred to as navel ill); traumatic injury with local introduction of infection; or iatrogenic infection associated with joint injection or surgery (usually in horses). Navel ill is only one example of a hematogenous route of infection, which can also be gained from GI or pulmonary sources.
Mycoplasma arthritis is common in growing calves 3–6 months of age. The tarsi and carpi are the most commonly affected joints. Mycoplasma arthritis is less common in dairy cattle than in beef cattle, although cases of Mycoplasma bovis polytendonitis or polyarthritis affecting a single limb in weaning calves to aged cattle have been recognized in dairy cattle. Mycoplasma arthritis has been found in many herds with Mycoplasma mastitis cases or in which Mycoplasma spp. are ubiquitous in the respiratory tract; affected calves frequently have concurrent pneumonia.
In young lambs, Actinobacillus seminis causes polyarthritis, as do Chlamydophila (Chlamydia) psittaci and Erysipelothrix rhusiopathiae (insidiosa). Erysipelas arthritis can follow docking, castration, or navel infection. Viruses and mycoplasma may also be etiologic agents in food-producing animals.
In mature goats, caprine arthritis and encephalitis virus is an important cause of septic arthritis. In young goats, Chlamydophila (Chlamydia) pecorum (reclassified from Chlamydophila [Chlamydia] psittaci) and Mycoplasma mycoides are frequent causes.
Bacterial (including Mycoplasma) arthritides occur in young pigs. In newborn pigs, septic arthritis usually is due to intrauterine or navel infection with Escherichia coli, Corynebacterium spp, Streptococcus spp, or Staphylococcus spp. Control is best directed toward decreasing the possibility of infection from the environment. Older pigs sometimes develop arthritis as a sequela of infection with Haemophilus spp, Erysipelothrix spp, or Mycoplasma spp. Although diagnosis in the early stages is not difficult, the more chronic stages can be confused with articular lesions produced by dietary hypervitaminosis A.
Traumatic injury to joints with bacterial contamination and progression to infection is common in horses, and various species of bacteria are involved. Infection associated with intra-articular injection or surgery occurs in horses and is usually associated with Staphylococcus aureus or S epidermidis.
Clinical Findings and Diagnosis of Septic Arthritis in Large Animals


Courtesy of Dr. Sameeh M. Abutarbush.

Courtesy of Dr. Stephen Adams.
Analysis of synovial fluid
Radiographic and ultrasonographic evaluation to determine the extent of damage to septic joints
Septic arthritis is usually characterized by severe lameness and distention of affected joints. Synovial fluid is usually cloudy and turbid and contains >30,000 WBCs/mL and a total protein concentration >4 g/dL. In addition, on cytologic evaluation, ≥80% of the nucleated cells are neutrophils. Degenerative neutrophils are apparent in most bacterial arthritis cases, but the neutrophils may be relatively well preserved in acute Mycoplasma infections. In young foals, calves, and other neonates with no history of trauma or joint injections, cell counts >10,000 WBCs/mL and total protein concentration >2.5 g/dL are strongly suggestive of sepsis. Failure to grow organisms on culture of synovial fluid does not rule out joint sepsis. Failure to isolate organisms is common in adult horses that have been treated with antimicrobial drugs before collection of synovial fluid for culture. Determining serum amyloid A (SAA) concentrations in synovial fluid may be helpful in differentiating nonseptic joint inflammation from joint sepsis. Concentrations of SAA are elevated in septic joints.
Radiographs of septic joints reveal soft tissue swelling and effusion in the early stages of disease. As sepsis progresses or goes untreated, subchondral bone lysis, collapse of the joint space, and periarticular new bone formation may occur. Ultrasonographic evaluation of affected joints can help determine the extent of capsular swelling, the presence of fibrin and debris within the joint, and subchondral irregularity. Computed tomography can be helpful in evaluating septic joints that may have subchondral changes not revealed by standard radiography.
In foals, in addition to infection of a puncture wound and contiguous soft tissue, hematogenous osteomyelitis often accompanies septic arthritis. Septic arthritis in foals has been classified into several types: septic synovitis of any joint with no bone involvement (S-type), osteomyelitis of the adjacent growth plate (P-type), osteomyelitis of the epiphyseal and subchondral bone (E-type), and osteomyelitis of the cuboidal bones of the carpus or tarsus (T-type). Various organisms may be involved.
Treatment of Septic Arthritis in Large Animals
Administration of systemic and local antimicrobials
Flushing of septic joints to remove bacteria, fibrin, and inflammatory mediators


Courtesy of Dr. Stephen Adams.
Septic arthritis requires prompt treatment to avoid irreparable damage to cartilage and subchondral bone. All affected horses should receive systemic broad-spectrum antimicrobial therapy. The initial choice is based on the most likely pathogen; however, it is subject to change depending on results of bacteriologic culture and antimicrobial susceptibility testing. Many horses are given a combination of penicillins (eg, ticarcillin or ampicillin) and aminoglycosides (eg, amikacin in foals or gentamicin in adults) initially; ceftiofur is used in calves. Systemic antimicrobial therapy should be combined with a method of local antimicrobial delivery, such as direct intra-articular injection, IV regional limb perfusion (IVRLP) in joints from the tarsus and carpus distally, and continuous delivery into affected joints using a pump. All local antimicrobial delivery methods achieve higher concentrations of antimicrobials in the joint and surrounding tissues than does systemic administration of antimicrobials alone. Flushing debris and bacteria out of the joint with through-and-through needle lavage or more aggressive arthroscopic lavage is indicated for all septic joints. Adjunctive treatment with NSAIDs (eg, phenylbutazone in horses or flunixin meglumine in cattle) to control pain and inflammation is also recommended. The effectiveness of treatment is monitored carefully through assessment of clinical signs and repeated analyses of synovial fluid.
Osteoarthritis
(Degenerative Joint Disease)
Etiology of Osteoarthritis in Large Animals
Osteoarthritis is characterized by a progressive degradation of articular cartilage with associated soft tissue inflammation and subchondral bone changes. Osteoarthritis can result from natural wear and tear on joints or from lack of treatment or unsuccessful treatment of joints with sepsis, osteochondrosis, or traumatic arthritis. For this reason, prompt diagnosis and correct management of traumatic synovitis and capsulitis, intra-articular fractures or traumatic cartilage damage, osteochondritis dissecans, subchondral cystic lesions, and septic arthritis is necessary to prevent osteoarthritis. Osteoarthritis cannot be cured but often can be successfully managed.
Clinical Findings and Diagnosis of Osteoarthritis in Large Animals


Courtesy of Dr. Stephen Adams.
Animals with clinically pronounced osteoarthritis are lame. Lameness can be localized to a joint by use of intra-articular analgesia delivered to the affected joint. There are varying extents of synovial effusion, joint capsule fibrosis, and decreased range of motion (decreased flexion). Radiographic signs of osteoarthritis include decreased joint space, uneven joint space, osteophyte formation, enthesitis, subchondral sclerosis, subchondral lysis, and soft tissue swelling. Advanced imaging such as MRI can be useful for evaluating joint disease in horses and determining the condition of bone, subchondral bone, and soft tissues. In less severe cases, articular degradation, particularly when the main component is cartilage loss and deterioration, may best be evaluated with arthroscopy.
Treatment of Osteoarthritis in Large Animals
Treatment of osteoarthritis is most commonly palliative and includes the use of NSAIDs; IM or intra-articularly administered polysulfated glycosaminoglycans; intra-articularly administered corticosteroids; IV or intra-articularly administered hyaluronic acid; biologic treatments such as autologous conditioned serum, platelet-rich plasma, and autologous protein solutions; and polyacrylamide hydrogel. Corrective shoeing may help some horses, particularly if osteoarthritis affects the distal limb joints. Orally administered joint supplements are commonly used for mild cases of osteoarthritis and may help some horses. Physical rehabilitation regimens may also prove useful. In advanced cases of osteoarthritis, surgical fusion (arthrodesis) may be performed on selected joints. Surgical fusion of the proximal interphalangeal joint (pastern) or distal tarsal joints can result in athletic soundness. Fetlock (metacarpophalangeal or metatarsophalangeal) joint arthrodesis and, less commonly, pan-carpal arthrodesis are also done in valuable animals and can make them comfortable and capable of breeding. Treatment is usually unsuccessful in chronic cases in bulls and cows; however, restricted exercise, along with careful feeding and nursing, prolong life and can be worthwhile for valuable breeding animals. In performance horses, arthroscopy may be performed to diagnose the extent of articular cartilage loss as well as to treat primary conditions such as articular cartilage separation, meniscal tears, and ligamentous injury.





