


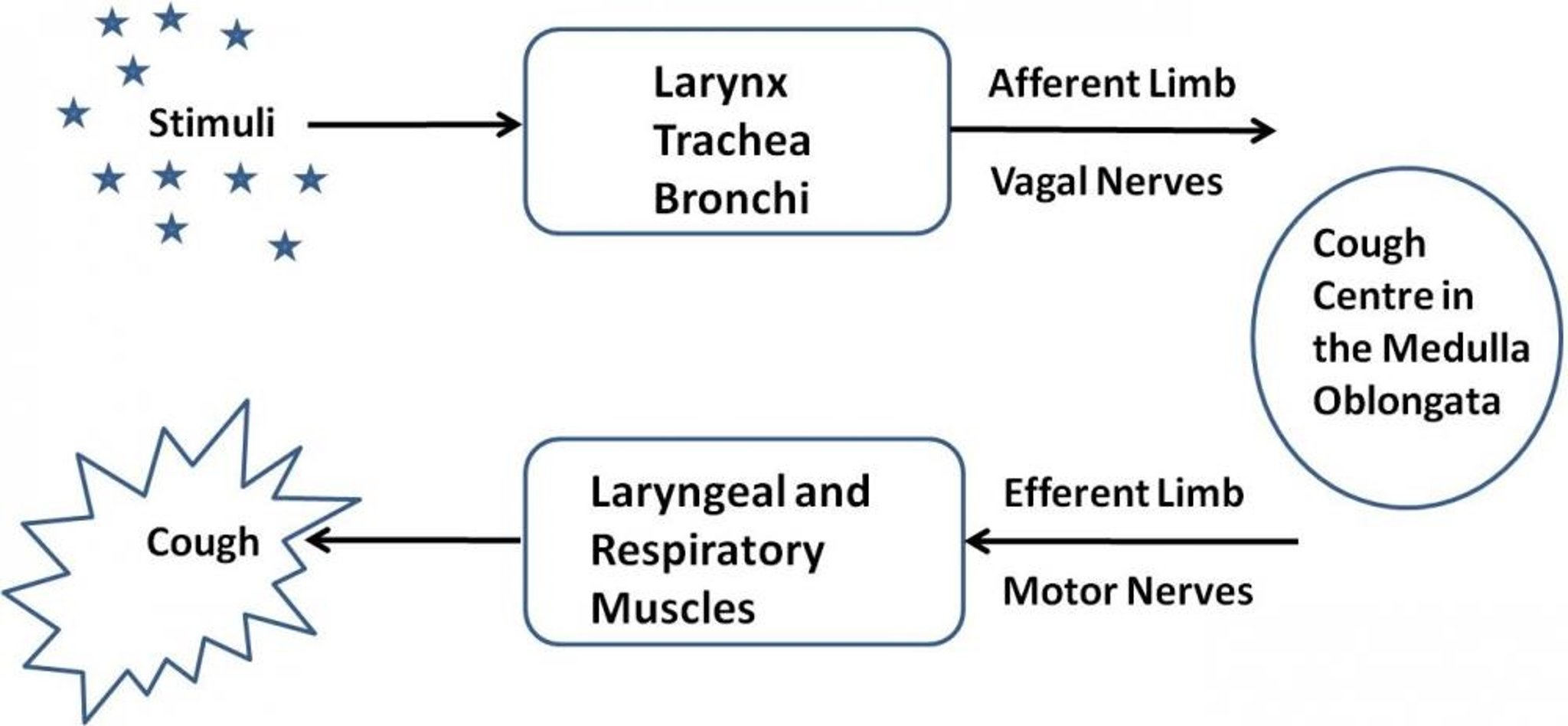
The sensory and motor pathways of the cough reflex.
Courtesy of Dr. Patricia Dowling.
A cough is a sudden, explosive exhalation of air that functions to clear material from the airways. Coughing is one way in which the lungs and airways are protected from inhaled particles. Coughing sometimes produces sputum (also called phlegm), a mixture of mucus, debris, and cells expelled from the lungs. The cough reflex has both sensory (afferent) and motor (efferent) pathways. The internal laryngeal nerve carries the sensory information away from the area above the glottis in the trachea to the cough center located in the medulla oblongata via the vagus nerve. Stimulation of this area by dust or foreign particles produces a cough to remove the foreign material from the respiratory tract before it reaches the lungs. Mucus production in the bronchi is an airway defense mechanism, and increases with inflammation and infection.
In dogs, cats, and horses, coughing occurs because of a primary disease process, such as Bordetella bronchiseptica infection ("kennel cough") or chronic bronchitis in dogs, feline asthma or heartworm-associated respiratory disease in cats, and equine asthma. In most cases, addressing the primary disease will resolve the cough. Antitussive treatment is supportive and is primarily for the comfort of the animal and the owner. Most antitussive drugs are opiates or opioids that directly suppress the cough center in the medulla oblongata ( see Table: Antitussive Drugs). The antitussive effect does not appear to be related to the binding of traditional opiate receptors (mu and kappa). For example, dextromethorphan is an opioid derivative with good antitussive activity in some species; however, it does not have activity at opiate receptors and is not analgesic or addictive.
Antitussive Drugs
Drug | Dosage |
|---|---|
Codeine | Dogs: 1–2 mg/kg, PO, q 6–12 h |
Hydrocodone | Dogs: 0.25 mg/kg, PO, q 6–12 h |
Butorphanol | Dogs: 0.055–0.11 mg/kg, SC, q 6–12 h, or 0.55–1.1 mg/kg, PO, q 6–12 h Cats: 0.1–0.4 mg/kg, SC, q 6–12 h |
Maropitant | Dogs: 2 mg/kg, PO, q 48 h |
Morphine is an effective antitussive at doses lower than those that produce analgesia and sedation. It is not commonly used for antitussive activity because of adverse effects and the potential for abuse and addiction. Morphine has poor oral bioavailability because of a significant first-pass effect by the liver.
Codeine is methylmorphine; methylation of morphine significantly improves the oral bioavailability by reducing the first-pass effect. Codeine phosphate and codeine sulfate are found in many antitussive preparations, including tablets, liquids, and syrups. Codeine has analgesic effects that are about one-tenth that of morphine; however, its antitussive potency is approximately equal to that of morphine. The adverse effects of codeine are considerably less than those that occur with morphine at antitussive doses. Adverse reactions (especially in cats) are exhibited as excitement, muscular spasms, convulsions, respiratory depression, sedation, and constipation. Codeine should not be used after GI tract surgery because of its effects on intestinal motility.
Hydrocodone is chemically and pharmacologically similar to codeine but more potent. It is combined with an anticholinergic drug (homatropine) to discourage abuse by humans. It is prescribed for dogs with chronic cough due to canine bronchitis; however, information on its use is mainly anecdotal.
Dextromethorphan is technically not considered an opiate, because it does not bind to traditional opiate receptors and is not addictive or analgesic. It is the d-isomer of levorphanol. The l-isomer of levorphanol has addictive and analgesic properties. Although it is recommended anecdotally to treat cough, a pharmacokinetic study in dogs demonstrated a short elimination half-life, rapid clearance, and poor oral bioavailability, making its use as an orally administered cough suppressant in dogs questionable.
Butorphanol, an opioid agonist-antagonist, is used as an analgesic and antitussive in dogs. As an antitussive in dogs, butorphanol is 4 times more potent than morphine and 100 times more potent than codeine. At antitussive dosages, it may produce considerable sedation in dogs. Because butorphanol has poor bioavailability, the oral dose in dogs is 10 times the subcutaneous dose. In cats, butorphanol is primarily used as an injectable analgesic. In some cats, it may cause pain on injection, as well as mydriasis, disorientation, swallowing/licking, and sedation.
Maropitant has potential for use as a cough suppressant. NK1 antagonism has been shown to have antitussive effects in canine and feline models. In a study of dogs with chronic bronchitis, maropitant given at 2 mg/kg, PO, every 48 hours for 14 days reduced frequency of coughing.
For More Information
Also see pet health content regarding drugs used to treat lung and airway disorders.





