

Pericardial disease most commonly causes an accumulation of fluid within the pericardial sac (ie, pericardial effusion). This accumulation can be acute or chronic, but chronic is much more common in veterinary medicine. When the fluid accumulation is severe enough to markedly increase the intrapericardial pressure, cardiac tamponade occurs. Acute cardiac tamponade primarily results in decreased cardiac filling and an abrupt decrease in cardiac output. Chronic cardiac tamponade primarily increases the diastolic intraventricular pressures, causing clinical signs of heart failure. Right-side diastolic pressure—and thus systemic venous pressure and capillary pressure—has to increase only from a normal of 5 mm Hg to 10–15 mm Hg to produce clinical signs of right heart failure, whereas left-side pressures must increase from a normal of < 10 mm Hg to > 20 mm Hg to produce left heart failure. Thus, clinical signs of right heart failure predominate.
Pericardial effusion is a relatively common form of acquired cardiovascular disease in dogs, is uncommon in cattle, and is rare in cats. In dogs, cases most commonly involve middle-aged, predominantly male, large breeds. Idiopathic pericarditis and cardiac neoplasia are the most common causes of pericardial effusion in dogs. Hemangiosarcoma and heart base tumors (chemodectoma, ectopic thyroid carcinoma) are the most common cardiac neoplasms. Heart base tumors usually are identified between the aorta and main pulmonary artery.
In cats, the most common cardiac neoplasia is lymphoma, but the most common cause of mild pericardial effusion is heart failure. Most cases of pericardial effusion in cats are not severe enough to cause cardiac tamponade. Less common causes of pericardial effusion in dogs are infections (eg, coccidioidomycosis), trauma, left atrial rupture, and CHF. Cattle most often develop pericardial effusion secondary to traumatic reticulopericarditis or cardiac neoplasia (lymphoma). Lymphoma in cattle can also result in valvular insufficiencies.
The severity of clinical signs with pericardial disease depends on the rate of pericardial fluid accumulation. In dogs, ascites is by far the most common clinical sign. Collapse, cough, and vomiting may occur. The femoral pulse may be weak or decrease on inspiration and increase on expiration (pulsus paradoxus). With slow development of pericardial fluid, the pericardial sac is able to stretch or enlarge, and clinical signs of right heart failure may not develop until severe pericardial effusion is present.
CBC, serum chemistry profile, and urinalysis results are usually normal in cases of pericardial effusion. In dogs, a tumor (most commonly a hemangiosarcoma) will occasionally bleed, producing an effusion with a PCV similar to that of blood.


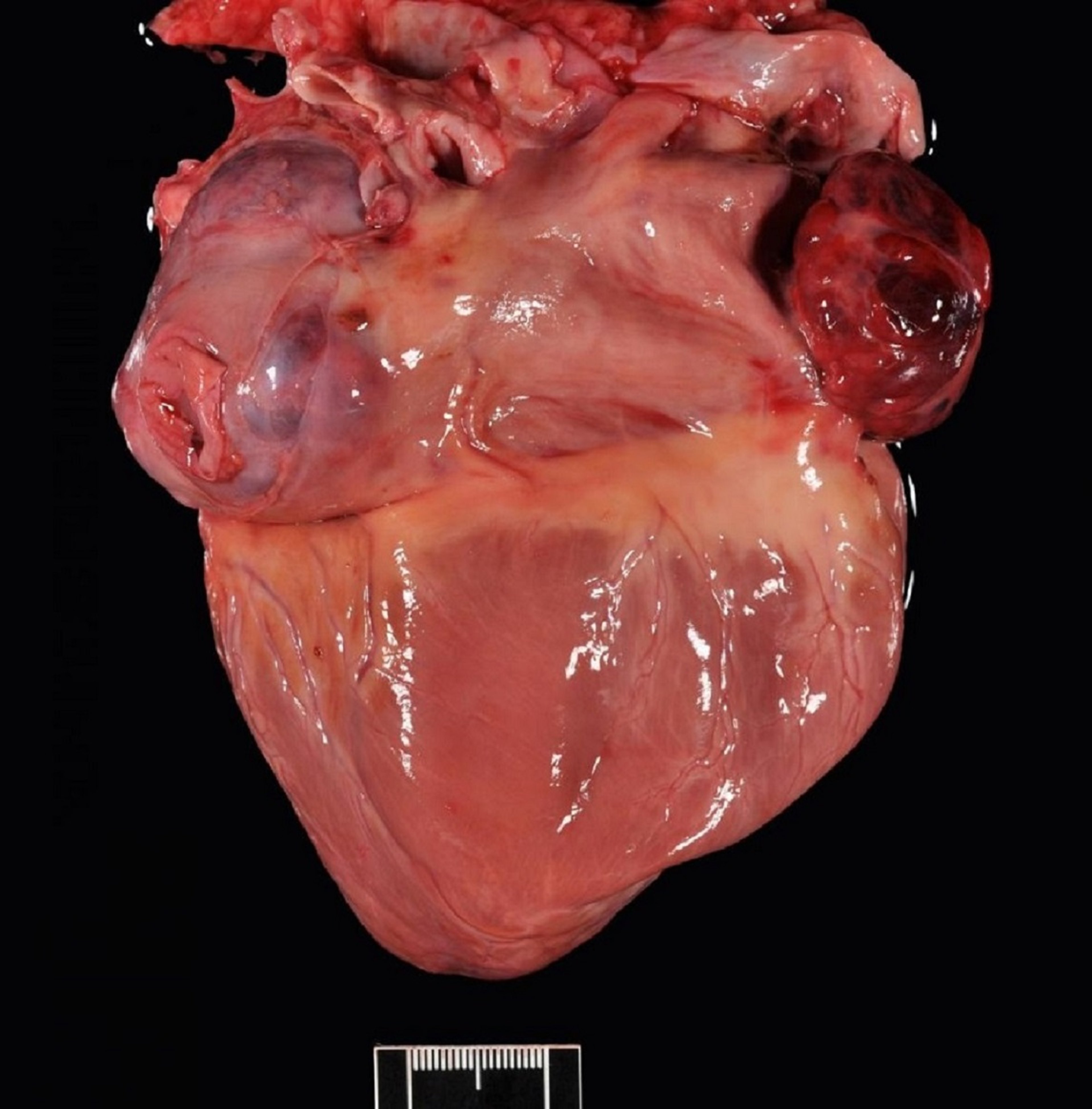
Courtesy of Dr. Mark D. Kittleson.

Courtesy of Dr. Mark D. Kittleson.
In dogs with pericardial effusion, radiographs often show an increase in the size of the cardiac silhouette, which commonly takes on a rounded (globoid) appearance. However, this classic appearance is not always present. If the cause is a cardiac tumor, especially a heart base tumor, the cardiac silhouette may have a bulge at the top of the heart cranial to the carina or at the region of the cranial waist if no effusion or only slight effusion is present. The caudal vena cava may be dilated if cardiac tamponade is present. Pleural effusion may also be present, more commonly if mesothelioma is the cause of the pericardial effusion.
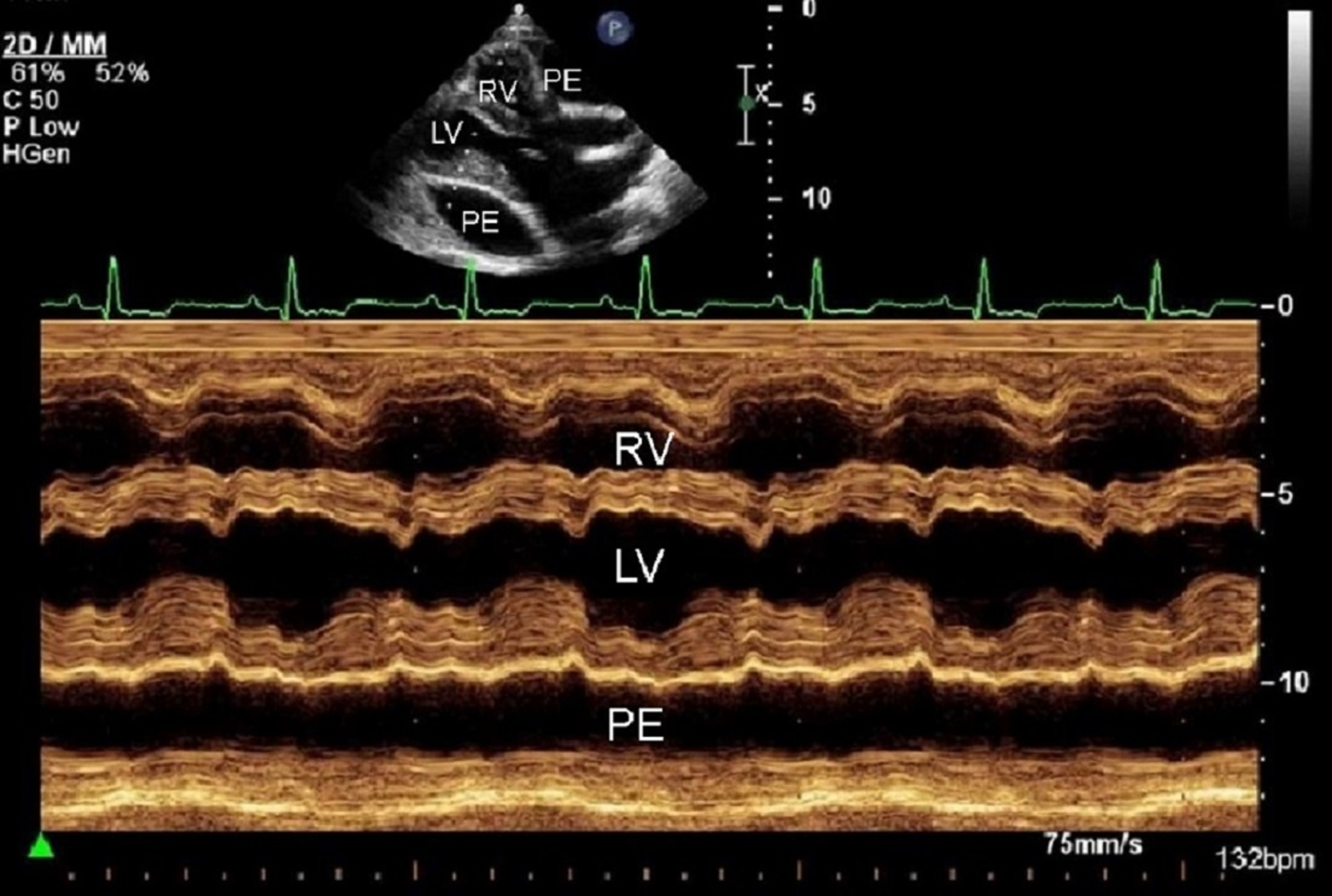
The ECG in most cases shows normal sinus rhythm to sinus tachycardia. Occasional atrial premature and ventricular complexes may occur. The height of the R wave is often decreased (< 1 mV in dogs), and there may be a pattern of alternating variation in R wave amplitude, referred to as electrical alternans, when a large amount of effusion is present. Electrical alternans results from the swinging motion of the heart within the fluid-filled pericardial sac. Echocardiography is the most sensitive and specific test for detection of pericardial effusion. A tumor can be visualized in most cases of neoplastic effusion. When cardiac tamponade is present, the walls of the right atrium and right ventricle may collapse in systole or diastole.
Animals with cardiac tamponade require mechanical drainage of the pericardial space (pericardiocentesis) using a catheter. Medical treatment is typically ineffective at decreasing pericardial effusion. Diuretics are contraindicated in acute cardiac tamponade because they decrease blood volume and cause a further decrease in cardiac output. Pericardiocentesis in dogs and cats is done by placement of a catheter through the chest wall on the right side, just above the costochondral junction at the fourth to fifth intercostal space. Echocardiography can be used to guide catheter placement at the point where the pericardial sac is closest to the thoracic wall and most distended with fluid, but it is not necessary. Fenestrating the catheter helps prevent blockage. A syringe or extension set with stopcock and syringe (preferred) is attached to the catheter. The system must be closed to air at all times after the chest wall has been penetrated, to avoid creating a pneumothorax.
The catheter is passed directly toward the heart while gently aspirating. When the pericardial sac is entered, fluid (usually quite bloody) flows freely into the syringe. The catheter should be carefully advanced over the needle into the pericardial sac. The fluid should be placed either in a glass tube or in a tube containing thrombin to cause clotting. If the blood clots, the catheter is in a cardiac chamber and should be removed from that chamber. As much fluid as possible should be removed from the pericardial sac, and a sample should be submitted for analysis. Pericardiocentesis is relatively easy to perform in dogs, and serious complications are rare. However, confirming the presence of pericardial effusion by echocardiography is advisable before performing pericardiocentesis.

Courtesy of Dr. Mark D. Kittleson.
Parenteral fluids may be given immediately before and after pericardiocentesis. Treatment with corticosteroids has not been shown to be beneficial in idiopathic pericarditis (benign pericardial effusion) in dogs. Most tumors that cause neoplastic effusion do not respond well to chemotherapy. Radiation treatment might be beneficial. Rarely, a hemangiosarcoma can be surgically removed if it is confined to the right auricle and no metastatic disease is present. Chemotherapy (eg, doxorubicin hydrochloride) might be beneficial in some dogs with hemangiosarcoma.
When idiopathic pericarditis is suspected (ie, no mass is visible on echocardiography), the owner should be instructed to carefully monitor the animal for any clinical signs of recurrence after pericardiocentesis. If such signs arise, a repeat pericardiocentesis is indicated. A subtotal pericardiectomy is generally recommended after the third pericardiocentesis. Heart base tumors only rarely metastasize in dogs; however, they can grow to be quite large and may compromise the function of surrounding structures. If recurrent pericardial effusion secondary to a heart base tumor is diagnosed, subtotal pericardiectomy should be considered. A dog can survive up to 2 years after successful subtotal pericardiectomy. The prognosis for right atrial hemangiosarcoma is poor to grave. Many dogs have metastasis or micrometastasis (most commonly to the lungs and not visible on radiographs) at the time of diagnosis.
Constrictive pericarditis and constrictive/effusive pericarditis are rare and occur primarily in dogs. They are thought to be an end result of chronic idiopathic pericarditis. A dog with constrictive pericarditis usually presents with ascites, no murmur, normal heart sounds, normal cardiac silhouette on thoracic radiographs, a positive hepatojugular reflux test (see Ascites), and distended hepatic veins on ultrasonography. Diagnosis can be difficult and may require cardiac catheterization. Treatment is surgical. With constrictive/effusive pericarditis, there is still a fluid layer between the pericardial sac and the surface of the heart, so surgical removal of the pericardium is relatively easy. With constrictive pericarditis, the pericardium and epicardium are fused into one fibrous layer that must be painstakingly removed surgically.





