

Infectious and inflammatory diseases of the spinal column and spinal cord include bacterial, rickettsial, viral, fungal, protozoal, and parasitic infections and idiopathic inflammatory disease. Many of these diseases can also affect the brain ( see Meningitis, Encephalitis, and Encephalomyelitis).
Bacterial Diseases
Diskospondylitis is inflammation of the intervertebral disk and adjacent vertebral bodies. Vertebral osteomyelitis is inflammation of the vertebra without concurrent disk infection. Vertebral physitis is infection centered on the vertebral physis, with no initial involvement of the disk space. These diseases are usually caused by hematogenous transmission of bacterial or, less commonly, fungal infection. Immunosuppression may play a role in some infections. Diskospondylitis is most common in dogs, especially larger breeds. Osteomyelitis of the lumbar vertebrae can develop in dogs secondary to migration of plant awns. Vertebral physitis generally affects the lumbar vertebrae of dogs < 2 years of age. Vertebral infection is rare in cats; it is usually due to direct transmission of infection from an adjacent wound. Diskospondylitis and vertebral osteomyelitis have also been reported in horses, ruminants, and pigs, especially neonates. Infection may occur at any disk space, and multiple lesions may occur.


Gross pathology photograph of a spinal vertebral body abscess in cross section. The pus visible in the affected disk space extends into the epidural space. The adjacent vertebral endplate shows bony lysis.
Courtesy of Dr. Sameeh M. Abutarbush.
In canine diskospondylitis, the most commonly isolated organisms are Staphylococcus spp. Other organisms include Brucella canis, Streptococcus spp, Escherichia coli, Proteus spp, Corynebacterium diphtheroides, Nocardia spp, and Aspergillus spp. Spinal pain is the most consistent clinical finding. Systemic clinical signs, such as fever, depression, and weight loss, are less common. Neurologic deficits may develop because of spinal cord compression caused by proliferative tissue or, rarely, transmission of infection to the spinal cord or pathological fracture.

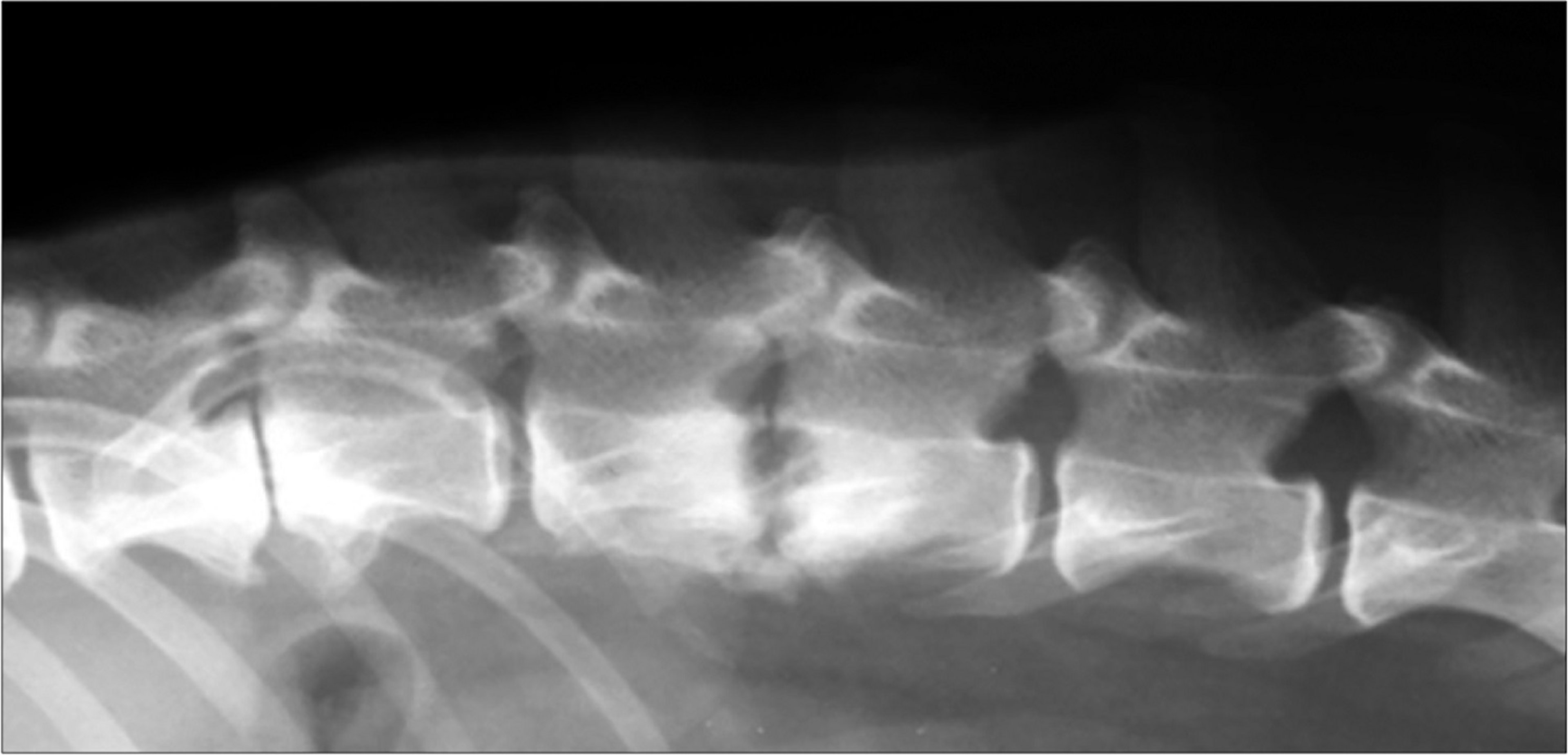
Lateral radiographic view of a dog with lysis of the vertebral endplates at L2 through L3, consistent with diskospondylitis.
Courtesy of Dr. William Thomas.
Early radiographic findings for diskospondylitis consist of destruction of the adjacent vertebral end plates and collapse of the disk space. More advanced lesions also have variable extents of osteophyte formation. Blood and urine cultures often identify the causative organism. Affected dogs should be tested for brucellosis (Brucella canis).
Although clinical signs of diskospondylitis usually resolve within 5 days of treatment with an appropriate antimicrobial, treatment should be continued for at least 12–16 weeks. Administration of amoxicillin potentiated with clavulanic acid for presumed Staphylococcus spp infection is a good choice if cultures yield no growth.
Rickettsial Diseases
Neurologic abnormalities, including clinical signs of spinal cord dysfunction, are sometimes evident in dogs with rickettsial infection. Dogs with Rocky Mountain spotted fever (Rickettsia rickettsii) often have thrombocytopenia, leukocytosis, and a neutrophilic pleocytosis and mildly increased protein on CSF analysis. Diagnosis is based on a 4-fold increase in serum antibody concentration. Dogs with ehrlichiosis (Ehrlichia canis) often have thrombocytopenia, anemia, leukopenia, hyperglobulinemia, and mononuclear pleocytosis and marked increase in protein on CSF analysis. A single serum antibody titer is usually sufficient for diagnosis of E canis. Treatment of rickettsial myelitis consists of administration of doxycycline (5 mg/kg, PO, every 12 hours for 14–21 days) or chloramphenicol (30 mg/kg, PO, every 8 hours for 14–21 days). Prognosis is good with early treatment, although neurologic deficits occasionally progress despite treatment.
Viral Diseases
Canine distemper encephalomyelitis, caused by a paramyxovirus, remains one of the most common CNS disorders in dogs worldwide. Onset of neurologic deficits may be acute or slowly progressive, reflecting the location of the lesions within the CNS. The brainstem and spinal cord are the regions most commonly affected in mature dogs. Clinical neurologic signs are usually not preceded by, nor coincident with, the systemic illness that occurs in young dogs.
Definitive antemortem diagnosis of canine distemper encephalomyelitis is difficult. There may be active or inactive chorioretinitis on fundoscopy. A lymphocytic pleocytosis with increased protein concentration is the most common finding on CSF analysis. Reverse transcriptase-PCR assay on urine or CSF is useful in diagnosis. There is no specific treatment, and the prognosis is poor for severely affected dogs. Vaccination is usually successful in preventing the systemic form of distemper; however, previously vaccinated dogs can be affected by the neurologic form.
Caprine arthritis and encephalomyelitis is caused by a lentivirus that can also cause pneumonitis and arthritis; CNS disease is most common in goats 2–4 months old, although older animals may also be affected. There is an acute onset of slightly asymmetric spastic paraparesis that may progress to tetraplegia with exaggerated reflexes. Mononuclear pleocytosis and increased protein in the CSF are present in ~50% of the cases. Serologic testing can help detect infection; however, false-negative results do occur. Histologically, there is severe nonsuppurative inflammation with demyelination or necrosis, most prominent in the white matter of the spinal cord. There is no treatment, and recovery is unlikely.
A related lentivirus is a rare cause of chronic encephalomyelitis in sheep (maedi). Affected sheep are usually >2 years old and suffer an insidious onset of progressive ataxia, paraparesis, or tetraparesis.
Equine infectious anemia occasionally produces encephalomyelitis in horses. Neurologic deficits are usually referable to spinal cord disease and include ataxia and weakness in the hind limbs. The protein concentration of and the number of lymphocytes in the CSF are often increased. Diagnosis is by positive results of agar gel immunodiffusion testing. There is no treatment, and affected horses are usually euthanized to prevent transmission of the disease.
Equine herpesvirus 1 (EHV-1) encephalomyelopathy is a neurologic disorder that affects horses worldwide. Equine herpesvirus 1 infects vascular endothelial cells, particularly those within the CNS, and causes immune-mediated vasculitis with secondary infarction and hemorrhage throughout the brain and spinal cord. Equine herpesvirus 1 has also been associated with meningoencephalitis in alpacas and llamas. In horses, neurologic signs may be evident as the primary disease or may follow rhinopneumonitis or abortion. Animals of any age may be affected.
Neurologic deficits have an abrupt onset, vary from mild hind limb ataxia to paraplegia, and usually do not progress after 24 hours. Urine dribbling, fecal retention, and sensory deficits in the perineum and tail are common. The CSF is often xanthochromic with increased protein content and normal numbers of cells. Diagnosis is based on clinical findings and an increase in antibody concentration in paired serum samples, isolation of virus from nasal or pharyngeal secretions, or PCR assay.
There is no specific treatment for EHV-1 encephalomyelopathy; however, anti-inflammatory agents such as dimethyl sulfoxide (1 g/kg, IV slowly, every 12 hours for up to 5 days), dexamethasone (2.5–5 mg, IM or IV, every 24 hours until clinical response), and NSAIDs may help. Supportive care is important to prevent complications such as urine retention, cystitis, and decubitus. Mildly affected horses often recover with supportive care. Even recumbent horses can eventually recover with meticulous nursing care. Vaccination does not protect from the neurologic form of this disease.
Feline infectious peritonitis is a disease of domestic cats caused by an immune-mediated response to a virulent biotype of feline coronavirus. Involvement of the CNS is common. There are pyogranulomatous lesions involving the neural parenchyma, choroid plexuses, ependyma, and leptomeninges. Clinical signs of spinal cord involvement include spinal hyperesthesia and paraparesis or tetraparesis. Hyperglobulinemia and involvement of other organs, especially the eyes, are common. Serum antibody tests currently available are insensitive and nonspecific. A mixed (neutrophilic and mononuclear) pleocytosis with increased protein concentration is the most common finding on CSF analysis. There is no effective treatment, and prognosis is poor.
Feline leukemia virus–associated myelopathy occurs in some cats infected with the feline leukemia virus (FeLV) for ≥2 years. Ataxia and weakness of the pelvic limbs progresses to paraplegia within 1 year. Other clinical signs include diffuse spinal pain and abnormal behavior. Diagnosis is based on clinical features, FeLV serology, and exclusion of other causes, such as spinal lymphoma and myelitis due to toxoplasmosis or fungal infection. There is no treatment; affected cats are eventually euthanized because of disability. Pathological findings consist of white matter degeneration, swollen axons, and dilation of myelin sheaths in the spinal cord and brainstem. Feline leukemia virus antigen is present in the nervous system, indicating that the lesions are due to viral infection.
Teschovirus encephalomyelitis, also called Teschen disease, Talfan disease, and porcine polioencephalomyelitis, is caused by a neurotropic teschovirus previously classified as an enterovirus. There is a peracute or subacute onset of hindlimb ataxia and paresis with hyporeflexia, depression, seizures, and death. Older pigs may survive, but mortality is high in young pigs.
Porcine hemagglutinating encephalomyelitis virus is a coronavirus that causes both vomiting and wasting disease and encephalomyelitis. It is most common in piglets < 3 weeks old, and there is some overlap of these syndromes. The CNS disease starts with several days of vomiting, which is followed by hyperesthesia, muscle tremors, ataxia, paresis, opisthotonos, coma, and death. Histopathologically, there is diffuse nonsuppurative encephalomyelitis, primarily involving gray matter. Diagnosis is based on necropsy or an increase in antibody titer in paired sera. There is no treatment.
Rabies is caused by a neurotropic rhabdovirus that reaches the CNS via peripheral nerves. It produces multifocal, nonsuppurative polioencephalomyelitis in all domestic mammals. Clinical signs of spinal cord involvement include ataxia and progressive paralysis, usually with absent reflexes. Affected animals typically, but not invariably, die with progressive neurologic signs within 2–7 days of illness.
Fungal Diseases
Cryptococcus neoformans is the most common fungus to involve the CNS in animals. Infection is most common in dogs and cats and occurs occasionally in horses. Other fungal organisms may invade the CNS, including Blastomyces dermatitidis, Histoplasma capsulatum, Coccidioides immitis, Aspergillus spp, and phaeohyphomycoses. Affected animals often have involvement of other organs, such as the lungs, eyes, skin, or bones. Clinical signs of spinal cord involvement include paresis or paralysis and spinal hyperesthesia. Diagnosis is based on serology, culture, or identifying the organism in CSF or extraneural tissue. Fluconazole is often effective for cryptococcosis and coccidioidomycosis. Itraconazole or amphotericin B is recommended for histoplasmosis and blastomycosis; however, the prognosis is guarded to poor. (Also see Fungal Infections.)
Protozoal Diseases
Equine protozoal myeloencephalitis is a common disease of horses that produces nonsuppurative, often necrotizing, meningoencephalomyelitis. Horses are likely an aberrant host for the causative organism, usually Sarcocystis neurona; less commonly, however, other protozoa cause the disease. Neurologic signs are extremely variable and often asymmetric, reflecting involvement anywhere in the CNS. Ataxia and paresis are common. Other potential clinical signs include obscure lameness, focal muscle atrophy, and cranial nerve dysfunction. Approximately 75% of affected horses improve with treatment; however, permanent neurologic deficits are possible and relapse is not rare.
Neosporosis is caused by Neospora caninum, a protozoan that can cause a nonsuppurative encephalomyelitis, most commonly in dogs. Infection in young puppies typically causes ascending paralysis with rigid contraction of the muscles of one or both pelvic limbs. Other organs, including muscle, liver, and lungs, can be affected. Diagnosis is based on detection of antibodies to the organism by immunohistochemical analysis or PCR assay. Early treatment with clindamycin or sulfadiazine and pyrimethamine may be effective; however, the prognosis is poor.
Toxoplasmosis is caused by Toxoplasma gondii and can occasionally cause nonsuppurative encephalomyelitis in puppies, kittens, and piglets. Diagnosis is based on identifying the organism in tissue or a 4-fold increase in IgG antibody in paired sera. In cats, a high concentration of IgM antibody in serum or CSF supports the diagnosis. Administration of clindamycin or sulfadiazine and pyrimethamine are recommended for treatment.
Parasitic Diseases
Verminous myelitis is inflammation of the spinal cord caused by parasite migration. Organisms include Parelaphostrongylus tenuis in sheep, goats, and llamas; Hypoderma bovis in cattle; Strongylus vulgaris, Halicephalobus deletrix, and Setaria spp in horses; Stephanurus dentatus in pigs; Cuterebra spp in cats; and Baylisascaris procyonis in dogs. Clinical signs of spinal cord involvement are usually acute, often asymmetric, and may be progressive. Antemortem diagnosis is difficult. Increased numbers of eosinophils in the CSF are suggestive, but CSF findings are variable. Treatment with fenbendazole, thiabendazole, or ivermectin is recommended; however, the prognosis is guarded. (Also see Central Nervous System Diseases Caused by Helminths and Arthropods.)
Idiopathic Inflammatory Diseases
Feline nonsuppurative meningoencephalomyelitis (feline polioencephalomyelitis, staggering disease) is a slowly progressive, inflammatory disease of the CNS in domestic cats. It has been reported in North America, Europe, and Australia. The cause is unknown; however, an infectious agent, probably a virus, is strongly suspected. The disease causes neuronal degeneration, axonal loss, and demyelination with mononuclear inflammation, most severe in the thoracic segments of the spinal cord. The clinical course is marked by progressive paraparesis of 1–2 months duration, often with focal hyperesthesia, head tremor, and behavioral changes. Antemortem diagnosis is difficult. There is no treatment, and prognosis is poor.
Granulomatous meningoencephalomyelitis (GME) is an inflammatory disease of the CNS in dogs worldwide. The cause is unknown, although an infectious agent, most likely a virus, is suspected. In the disseminated form, previously called inflammatory reticulosis, there are perivascular accumulations of mononuclear cells and neutrophils. In the focal form, previously called neoplastic reticulosis, there are granulomatous lesions containing primarily reticulohistiocytic cells. Adult dogs of any breed can be affected; however, female, small-breed dogs, especially Poodles, may be predisposed.
Clinical signs of GME are variable and may indicate focal or multifocal brain or spinal cord dysfunction. Cervical pain and tetraparesis are the most common clinical signs of spinal cord involvement. Clinical signs are often acute; however, the focal form of GME can cause neurologic deficits that slowly progress over several months. The CSF usually has increased protein and pleocytosis, with either mononuclear cells or neutrophils predominating. Advanced imaging (ie, MRI or CT) often shows single or multiple enhancing masses. Tentative diagnosis is based on clinical findings, imaging, CSF analysis, and exclusion of other possible diseases. Dogs often improve with administration of immunosuppressive doses of corticosteroids and other immunomodulating drugs such as cytarabine, cyclosporine, and procarbazine; however, relapse is possible, and many dogs eventually become refractory to treatment.





