




Dystocia (Egg Retention) in Reptiles


Courtesy of Dr. Stephen Divers.

Courtesy of Dr. Stephen Divers.
Routine sterilization of young reptiles is still uncommon but is certainly practical in many lizards and chelonians. Currently, therefore, reproductive disease remains a common presentation in practice. In oviparous reptiles, eggs (demonstrating various degrees of shell mineralization) may be retained, whereas in (ovo)viviparous species unfertilized ova or fetuses may be seen. In some cases, abnormal and persistent preovulatory follicles may also be diagnosed as spherical masses that fail to ovulate or resorb (preovulatory follicular stasis). Dystocia is generally not an acute presentation as in mammals or birds, and reptiles may retain eggs/fetuses for weeks or even months after the normal timing of laying/birth. Coupled with imprecise details of copulation, this can often make the distinction between normal gravidity and dystocia difficult in otherwise clinically healthy reptiles. Certainly, severe metabolic disturbance and infection can exacerbate the issue. In general, a presumptive diagnosis can be achieved through palpation and diagnostic imaging, especially radiography and ultrasonography. Hematology and plasma biochemistry may also help identify inflammatory/infectious changes and metabolic disturbances, especially hypercalcemia.
Unless there is evidence of obstructive disease, medical management may be tried, although it frequently fails. Improvements in husbandry (especially provision of solitude and a suitable substrate), corrections of any metabolic disturbances, subcutaneous dilute oxytocin/vasotocin, and potentially prostaglandin (PGF2a and PGE) may be helpful. In most cases, surgical ovariosalpingectomy is required (unless a valuable breeding animal) after medical stabilization.
After a diagnosis of reproductive disease or complication, surgical investigation (including biopsy) or reproductive sterilization may be indicated. Ovariectomy (oophorectomy), ovariosalpingectomy, salpingotomy, orchiectomy and phallectomy are commonly performed surgical procedures in reptiles. Surgery is often indicated with reproductive disease such as oophoritis, orchitis, salpingitis, paraphimosis, and neoplasia. For breeding reptiles, sample collection, including surgical biopsies, may be performed intraoperatively. Complications from reproductive activity in females (with or without the presence of a mate), including preovulatory follicular stasis, dystocia (postovulatory egg stasis), ectopic eggs, or egg yolk coelomitis, are common indications for surgery.
Preventive health measures and behavior management of pet or display reptiles may include elective gonadectomy to eliminate high-risk complications of reproduction in females or to reduce aggression in males. When preserving future reproductive capabilities is important, salpingotomy and unilateral ovariosalpingectomy may be indicated.


Courtesy of Dr. Stephen Divers.
In chelonians, ovariectomy, orchiectomy, and phallectomies have been used to manage population issues in conservation projects. Vasectomy, although an option for male sterilization, is not commonly performed. Prolapses involving reproductive organs are common in reptiles and are a frequent indication for surgery. Many reproductive surgical procedures discussed here can be performed using minimally invasive endoscopic approaches.
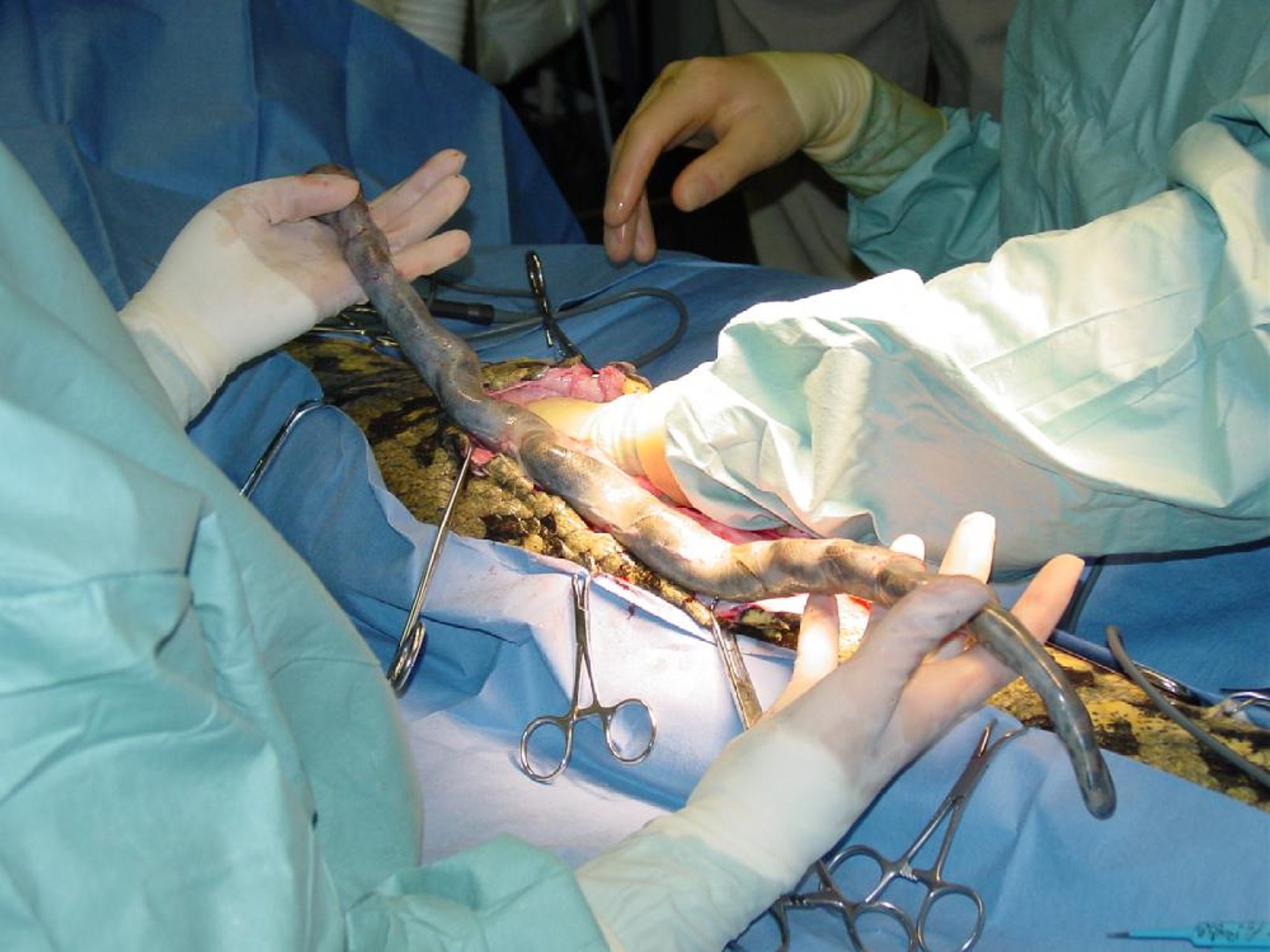
In most female lizards, the reproductive tract is accessed surgically from a ventral coeliotomy (midline or paramedian) approach, whereas in chameleons a lateral approach is often preferred. Once the coelom is entered, the enlarged reproductive structures (ie, enlarged ovaries in pre-ovulatory follicular stasis or egg-filled oviducts in cases of dystocia) are obvious; however, the paired coelomic fat pads, bladder (if present), and portions of the gastrointestinal tract may need to be retracted or exteriorized. In cases of dystocia, the oviducts are filled with eggs or fetuses and need to be exteriorized and removed first to allow exposure of the ovaries, which may be small. In cases of follicular stasis, the ovaries are typically very large and the oviducts small. In most cases involving pet reptiles, ovariosalpingectomy is performed; however, where breeding potential must be retained, salpingotomy and egg removal or hemiovariosalpingectomy may be indicated. Vascular clips are often used to expedite surgery.

Indications for ovariectomy and ovariosalpingectomy are less common in snakes but are often related to damage to the salpinx via prolapse or an obstructive dystocia. In these cases, if the oviduct cannot be repaired the ipsilateral ovary must be removed along with the diseased or damaged oviduct.
In chelonians, a prefemoral, soft-tissue approach to the coelom is preferred to avoid going through the plastron. Such an approach facilitates unilateral access to the ipsilateral ovary and oviduct to remove single eggs or to perform an ovariosalpingectomy. Such an approach also provides access to the bladder to remove egg(s). In many species, bilateral ovariectomy can be performed from a unilateral approach. If extensive pathology is present or when access is required, a ventral plastronectomy may be necessary.
Vent Prolapse in Reptiles

Courtesy of Dr. Stephen Divers.

Courtesy of Dr. Stephen Divers.
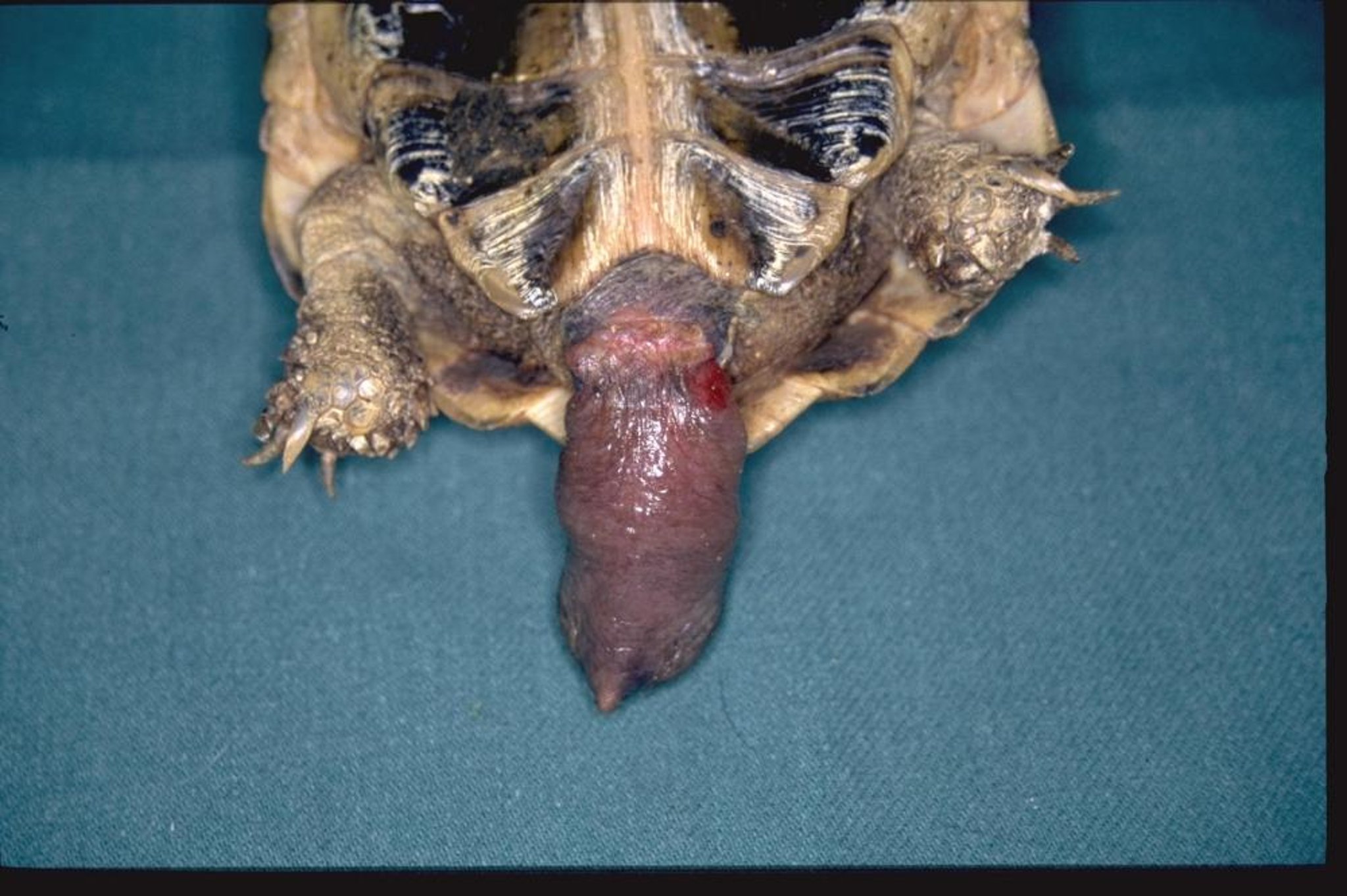
A variety of prolapses may be seen emanating from the vent of reptiles, including cloaca, colon, oviduct, hemipenes/phallus, and (if present) bladder. Common causes include dystocia, copulation trauma, cloacitis, bacterial/fungal/parasitic infection, metabolic disease (especially secondary hyperparathyroidism), cystic calculi, renal disease, neoplasia, or any space-occupying lesion within the coelom causing tenesmus. It is important to identify the prolapsed organ, because some (eg, phallus/hemipenes) can be amputated, whereas others (eg, cloaca, colon) cannot. The prolapse should be gently cleaned, and the application of hyperosmotics may help reduce swelling and facilitate replacement. However, it is also important to determine the cause to prevent recurrence.

Courtesy of Dr. Stephen Divers.
Prolapses of the hemipenes and phallus can be amputated after induction of general anesthesia or intrathecal (caudal spinal) block; this will render the animal infertile. If the prolapsed tissue is viable and can be replaced, purse-string sutures of the vent should be avoided, because they tend to deform the vent and may interfere with the urogenital openings. In such cases, it is preferable to use a transcutaneous cloacopexy technique. If the tissue is not viable, then careful and detailed surgery is required when attempting debridement and resection-anastomosis of the cloaca, colon, or bladder and often necessitates both cloacal and coeliotomy approaches.
For More Information
Divers SJ and Stahl SJ (2019), Reptile and Amphibian Medicine and Surgery, Elsevier Publishing.







