



A comprehensive reproductive evaluation is recommended for the mare that has unknown or questionable fertility. Abnormalities can be diagnosed and appropriate therapy instituted to correct any problem before breeding is scheduled. A coordinated plan of management should be developed based on the mare’s history of reproductive performance, previous treatments, examination findings, laboratory test results, and intended use.
Theriogenologists typically examine mares for breeding soundness before purchase or breeding, or when a mare is barren. A complete breeding soundness examination includes:
examination of the external genitalia and mammary gland
palpation and ultrasonography per rectum of the internal genitalia
manual and visual vaginal examination (vaginoscopy)
aerobic culture of an endometrial swab/sample
cytologic evaluation of an endometrial swab/sample
histologic evaluation of an endometrial biopsy sample
In the case of a young, healthy, maiden mare, palpation and ultrasonography per rectum to determine the presence of a uterus of normal size and consistency, normal active ovaries, and functional cervix may suffice. Perineal conformation should be evaluated. A manual vaginal examination should be performed to confirm the hymen is patent. If there is evidence of pneumovagina or vaginitis, commonly present in slim, fit, racing fillies, or if uterine fluid or discharge is seen, an endometrial swab and biopsy are indicated.
In postpartum mares, palpation and ultrasonography per rectum are required to evaluate uterine involution. A manual vaginal examination should be performed to ascertain whether the reproductive tract was traumatized during foaling. Thorough evaluation of the cervix requires direct manual palpation per vagina of the cervix after foal heat ovulation when the mare is in diestrus and under progesterone stimulation. Mares that had foaling problems (eg, dystocia, retained placenta) require a more extensive evaluation. All postpartum mares have a transient endometritis during uterine involution; therefore, uterine swab and biopsy typically provide more useful information if delayed for ≥3 weeks after parturition.
Barren mares require a complete breeding soundness examination. Occasionally, hysteroscopy, endocrine assay, or a karyotype may provide additional information.
Signalment and History in the Breeding Soundness Examination of the Mare

A simple form with spaces to make entries regarding all aspects of the genital tract may help in performing a complete and thorough examination.
Courtesy of Dr. Patricia Sertich.
A standard breeding soundness examination form to record examination findings can be helpful to ensure all parts of the genital tract are examined. The horse should be accurately identified.
Determination of stage of reproductive cycle and estrous cycle is essential for proper evaluation and interpretation of laboratory test results. The history should include previous length and character of estrus, breedings and their results, therapy, and specific reproductive problems. In particular, histologic findings of an endometrial biopsy sample reflect the stage of the mare’s reproductive cycle and any recent intrauterine activities (breeding, treatment, foaling). Regardless of the history, the mare’s nonpregnant status should be confirmed before performing any procedures (eg, endometrial swab, endometrial biopsy, direct manual cervical palpation) that would compromise an existing pregnancy.
Restraint in the Breeding Soundness Examination of the Mare


Sedatives administered to calm a mare will cause considerable relaxation of the perineum, making the anus appear sunken and the vulvar labia poorly apposed and incompetent.
Courtesy of Dr. Patricia Sertich.
Most mares can be restrained in hand, in stocks, or placed against a stall wall with the hindquarters positioned in a doorway. For noncompliant mares, a twitch may provide short-term restraint to allow completion of the examination. For the occasional situation in which the temperament of the mare poses risk of injury to the mare or examiner, chemical restraint may be used. A combination of acepromazine (0.02 mg/kg) and xylazine HCl (0.3–0.5 mg/kg) administered IV works well for short procedures. Intravenous administration of detomidine HCl (0.01 mg/kg) followed by butorphanol tartrate (0.02/kg) may facilitate longer procedures in fractious mares. If possible, the external genitalia should be evaluated before tranquilizers are administered, because the drug's use will alter the tone and competency of the perineum.
Physical Examination in the Breeding Soundness Examination of the Mare

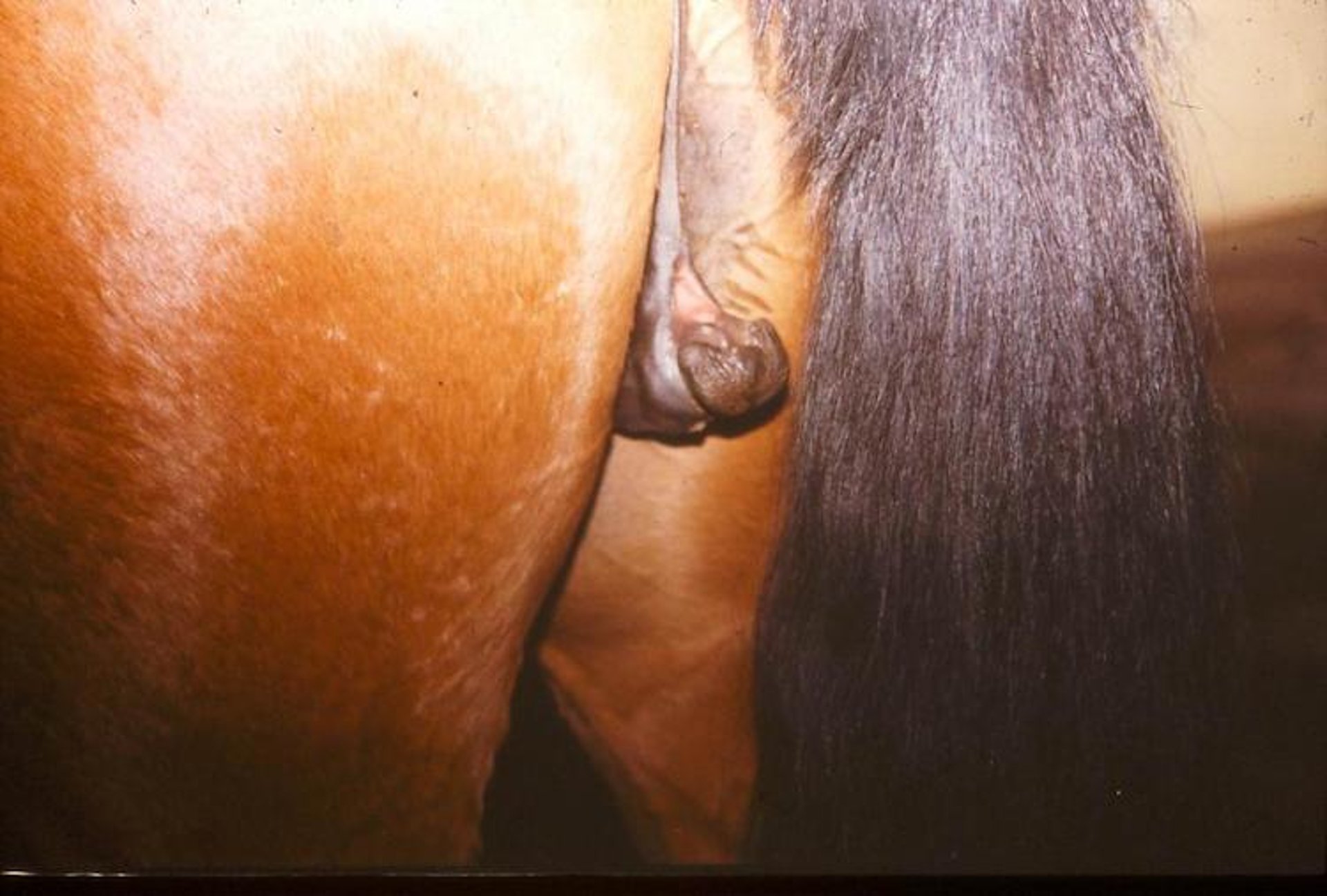
Disorder of sexual development with an enlarged clitoris and internal testicles.
Courtesy of Dr. Patricia Sertich.


Vulvoplasty has been performed to prevent air from being aspirated into the caudal genital tract. Mares with poor perineal conformation may be prone to chronic uterine infections and benefit from a Caslick operation. Owners must be instructed to have an episiotomy performed before parturition in any pregnant mare that has had a Caslick operation.
Courtesy of Dr. Patricia Sertich.
The mare’s tail should be wrapped and tied to one side. The tail and inner thighs should be examined for the presence of dried exudate indicative of genital infection or urine staining that may be associated with urine pooling or incontinence. The size and shape of the clitoris should be assessed. A mare with an excessively large clitoris may have been androgenized either by excessive exogenous hormone administration during pregnancy or by endogenous hormones in an intersex condition (disorder of sexual development). Normal vulvar lips have good tone and apposition and form the first barrier of the uterus against environmental contaminants. The vulvar lips should be parted to determine the competency of the vestibulovaginal fold. If air readily aspirates into the vagina, the mare may be prone to pneumovagina and may require a vulvoplasty (Caslick operation).


Note the presence of perineal exudate on a mare with endometritis.
Courtesy of Dr. Patricia Sertich.


For per rectum procedures, the examiner, wearing a clean examination sleeve with water-soluble lubricant, must first empty the rectum of feces. Palpation and ultrasonography per rectum permit assessment of the internal genital tract. Each part of the genital tract should be systematically palpated. Typically, a real-time 5–10 MHz linear ultrasound probe, which produces a rectangular, cross-sectional image of the structure scanned, is used for ultrasonographic examinations of the reproductive tract. Ovarian size and character as well as the presence of an ovulation fossa should be noted. Anechoic follicles should be measured and counted, and the presence of a hyperechoic corpus luteum recorded. Normal oviducts are not routinely examined because their normal small size prevents palpation and imaging.


Sonogram of endometrial cysts in the base of the right horn of a uterus. The examining veterinarian should always “map” the location of any cysts when breeding a mare. Knowledge of cyst location will prevent mistaking a cyst for an early conceptus when the mare is being examined for pregnancy.
Courtesy of Dr. Patricia Sertich.


Ultrasonography of the uterus will allow characterization of the amount and echogenicity of intraluminal uterine fluid. Note the scalloped edge of the endometrial folds projecting into the lumen.
Courtesy of Dr. Patricia Sertich.
The size, shape, and contents of the uterus should be recorded. The mare’s uterus is T-shaped with the horns perpendicular to the body of the uterus. It is suspended in the pelvic canal by the broad ligament, which is attached dorsally to the sublumbar region. Ultrasonography permits accurate assessment and measurement of the uterine horns. The size and character of any anechoic endometrial cysts should be recorded for reference so their presence will not be confused with a conceptus during subsequent early pregnancy examinations.


Each uterine horn should be carefully palpated and slipped through the examiner's fingers to allow palpation of the endometrial folds. These endometrial folds are palpable in the nonpregnant mare. After a mare is>2–3 weeks pregnant, the character of the uterus changes so the folds are no longer palpable.
Courtesy of Dr. Patricia Sertich.
The uterus has several endometrial folds that increase the surface area of the uterine lumen. The endometrial folds should be carefully assessed during palpation per rectum by "slipping" the folds through the examiner’s fingers along the entire length of each horn. The character of the uterus changes during the estrous cycle. During estrus, the endometrial folds become edematous, causing the uterine horns to have alternating areas of hypo- and hyperechogenicity when a cross-section is viewed ultrasonographically. As estrus progresses, the edema in the endometrial folds wanes so that it is minimal by the time of ovulation. After ovulation and development of the corpus luteum, the uterus is stimulated by progesterone, uterine tone increases, and the endometrial folds are no longer edematous but are still palpable in diestrus. After 14–18 days of gestation, the endometrial folds are not readily palpable because of the gradual but marked increase in uterine wall thickness.


Vaginoscopy may be required to determine the character of the vaginal fluid.
Courtesy of Dr. Patricia Sertich.
The length, width, and tone of the cervix are palpable per rectum; however, complete evaluation of the cervix requires direct palpation per vagina. A cervical evaluation also serves as a bioassay, because the cervix changes in response to the steroid hormone status of the mare. During anestrus, ovarian steroid serum concentrations are low, and the cervix is either short, thin, and open or closed but readily opened. After the first ovulation of the season and during subsequent periods of diestrus, serum progesterone concentrations are increased and the cervix is closed and has tone with a long cylindrical shape. During estrus, serum progesterone concentrations are low, and estrogen concentrations are high; the cervix is relaxed and edematous. Visual (speculum) vaginal examination will allow further assessment of the character of the cervix.

Urine may be present in the vagina transiently during estrus or chronically if conformation is poor.
Courtesy of Dr. Patricia Sertich.

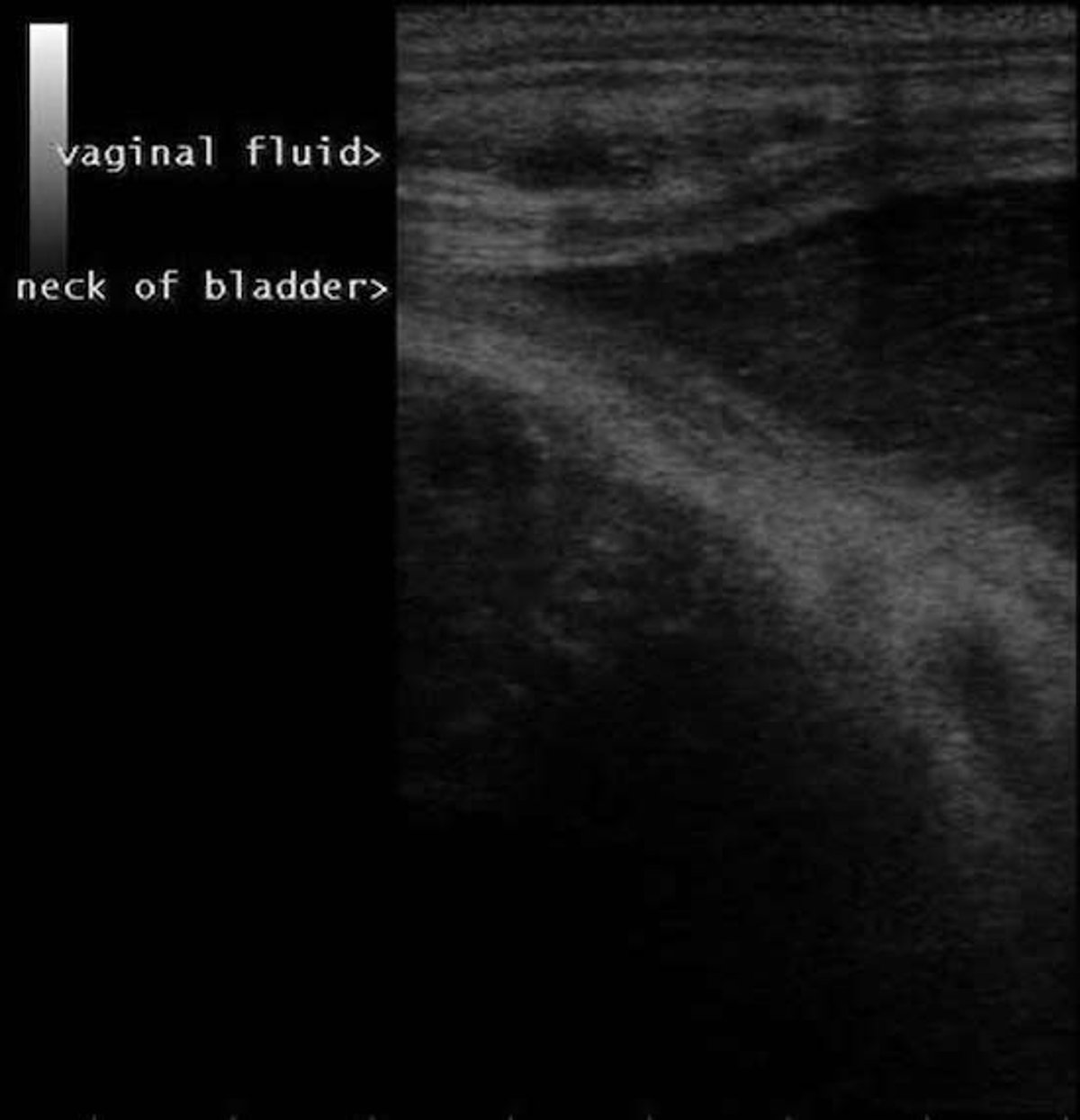
The urethra attaches to the neck of the bladder and opens into the vestibule at the base of the vestibulovaginal fold, which is the caudal border of the vagina. An accumulation of fluid cranial to the vestibulovaginal fold and dorsal to the bladder is abnormal.
Courtesy of Dr. Patricia Sertich.
Urine in the vagina (urovagina) may be seen sporadically or be a chronic problem. Mares with urovagina may have an abnormal voiding pattern, and the endometrium may show histologic evidence of chronic irritation. The neck of the bladder can be used to indicate the caudal boundary of the vagina during ultrasonography. The vagina can be imaged dorsal to the bladder and examined for any accumulation of echogenic fluid caudal to the cervix. A definitive diagnosis of urovagina requires direct observation of urine in the vagina via vaginoscopy.
Endometrial Samples for Aerobic Culture and Cytology in the Breeding Soundness Examination of the Mare
Before an endometrial swab is taken, the nonpregnant status of the mare must be confirmed because the swabbing could lead to termination of a pregnancy. The perineum is cleansed with povidone-iodine scrub, rinsed, and dried. The operator dons a sterile sleeve or clean examination sleeve with the hand encased in a sterile glove. A water-soluble lubricant free of bacteriostatic chemicals is placed on the back of the hand and lower arm. When obtaining an endometrial swab sample, the vestibule, vagina, and cervix must be passed. Care must be taken to avoid contamination of the swab by microorganisms in the structures caudal to the uterus that would hinder accurate interpretation of the culture results.
A double-guarded occluded uterine swab is gently guided through the cranial end of the cervix. Once inside the uterine body, the inner guard is advanced from the outer guard, and the swab is exposed to the uterine lumen for 30–60 seconds. The swab tip is withdrawn into the inner guard, which is then withdrawn into the outer guard before the entire swabbing instrument is removed from the uterine body. The swab tip is carefully placed into a transport system, which is vital to maintain viability of the organisms from the time of sample collection until aerobic culture in the laboratory. Stuart's transport medium may maintain microorganisms for as long as 72 hours if stored at ambient temperature. A second endometrial sample may be taken immediately after the first or simultaneously with a uterine swab or cytology brush. This sample is rolled onto a glass microscope slide, fixed and stained with a Romanowsky-type stain, and viewed microscopically for cytologic evidence of neutrophils, debris, and microorganisms.
A low-volume uterine lavage can be performed in mares with negative culture results despite obvious clinical signs of endometritis. Sterile saline (60–150 mL) is infused into the uterus using a closed system with a small uterine catheter. Oxytocin (20 IU, IV) is administered to enhance uterine evacuation. The effluent is collected by gravity flow and then transferred into a sterile centrifuge tube and centrifuged. The pellet is then swabbed, placed into transport media, and submitted for aerobic culture. A second swab can be made of the pellet for cytologic examination after staining.
Most microbiology laboratories streak the endometrial swabs on 5% sheep blood agar for general growth and on MacConkey’s agar for growth of gram-negative organisms, and agar plate cultures are then aerobically incubated at 37°C (98.6°F).
Organisms commonly isolated that are associated with endometritis include:
beta-hemolytic streptococci (90% Streptococcus zooepidemicus, 10% S equisimilis)
Escherichia coli
Pseudomonas sp (65% P aeruginosa)
Klebsiella pneumoniae
Organisms isolated that are commonly suspected to be contaminants include:
α-hemolytic streptococci
Actinobacillus equuli
Salmonella enteritidis
Pasteurella-like species
Staphylococcus sp
Enterobacter sp
Acinetobacter sp
Proteussp
Citrobactersp
Alcaligenes sp
Aeromonas sp
In most cases, the mixed growth of a few miscellaneous microorganisms is not significant. A heavy growth of any microorganism should be considered significant unless obvious contamination has occurred. Clinical signs must be correlated with culture results to determine clinical significance and to develop a therapeutic plan. Isolation of an organism transmitted venereally, such as Taylorella equigenitalis (requires a special culture system) and certain strains of Pseudomonas and Klebsiella spp, is considered a significant finding. Occasionally, microorganisms causing a pyometra may not be detected on aerobic culture, because products of the inflammatory reaction prohibit their growth.

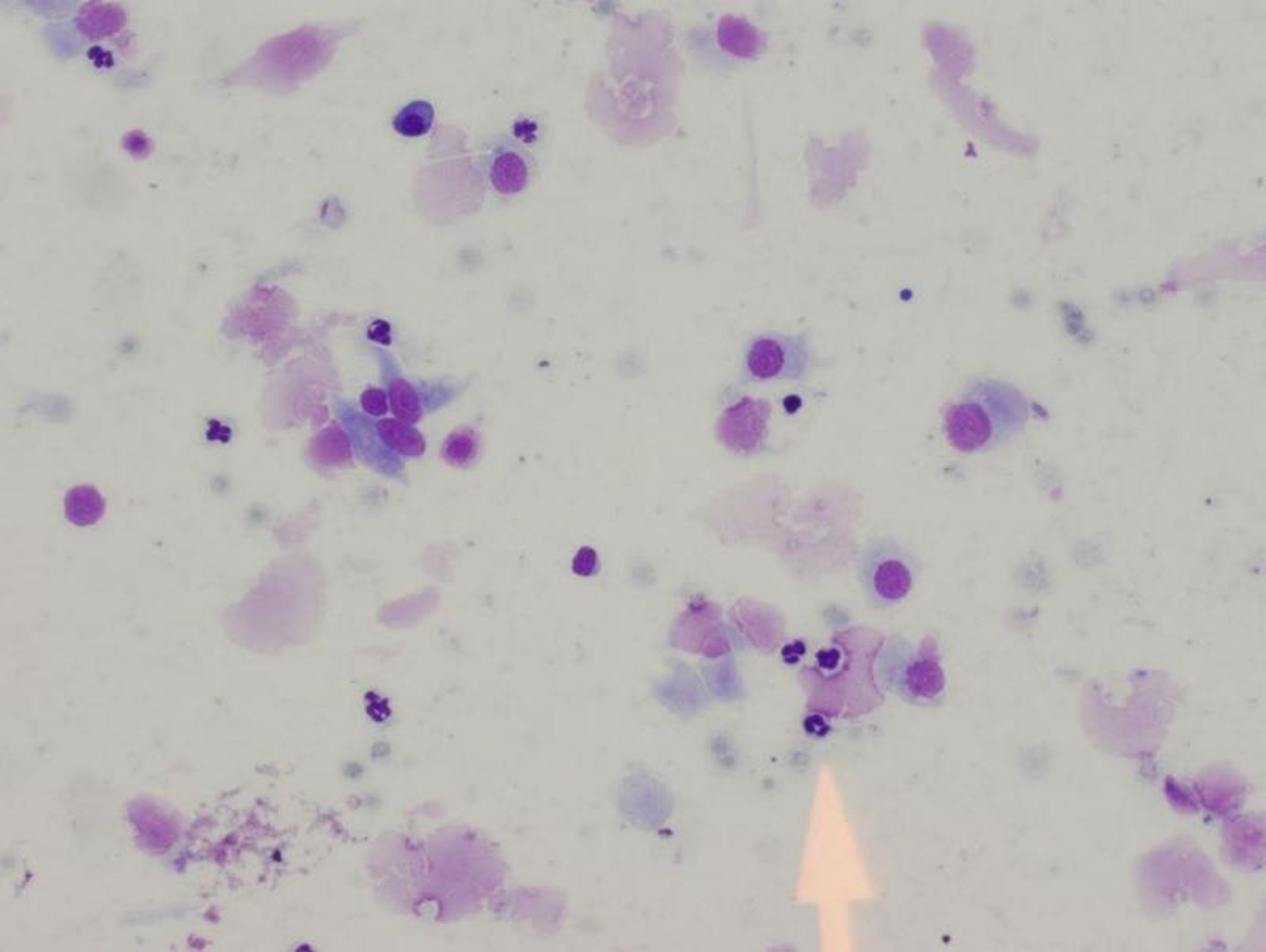
Neutrophils may be harvested from a uterine swab/brush or low volume lavage in a mare with an acute endometritis; arrow points to neutrophil (Romanowsky-type stain).
Courtesy of Dr. Patricia Sertich.
Results of aerobic culture of the endometrial swab should be used as a diagnostic adjunct and not as the sole determinant in diagnosing a uterine infection. A positive culture result must be accompanied by evidence of inflammation for the diagnosis of endometritis to be made. Mares exhibiting clinical signs of infection (uterine fluid as seen on ultrasonographic examination per rectum, tail matting or uterine discharge, and the presence of inflammatory cells seen on a stained smear from a uterine sample) with a positive endometrial swab culture are likely to have endometritis. Inflammation seen on histologic evaluation of the endometrium confirms the diagnosis of endometritis. In these cases, the culture results are useful in determining the sensitivity of the causative microorganism and developing an antimicrobial treatment plan.
The following antibiotics ( see Table: Intrauterine Antibiotics for Use in Mares) have been used for daily (3–7 days) uterine infusion by diluting with sterile saline to an infusion volume of 60–100 mL. Systemic administration of antibiotics may be considered if the microorganism, management situation, and ease of treatment indicate. Two doses of long-acting ceftiofur crystalline free acid (6.6 mg/kg, IM) can be administered 96 hours apart to maintain adequate serum concentration for 10 days, which may be an efficacious treatment for endometritis due to S zooepidemicus.
Intrauterine Antibiotics for Use in Mares
Antibiotic | Intrauterine Dose |
|---|---|
Penicillin (sodium or potassium salt) | 5 million U |
Ampicillin | 1–3 g |
Ticarcillin | 3–6 g |
Ticarcillin with clavulanic acid | 3–6 g |
Carbenicillin | 2–5 g |
Gentamicin sulfate diluted with 20 mL sodium bicarbonate and 20 mL saline | 1 g |
Amikacin sulfate | 1–2 g |
Ceftiofur sodium | 1 g |
Clotrimazole | 400–700 mg |
Endometrial Biopsy in the Breeding and Soundness Examination of the Mare

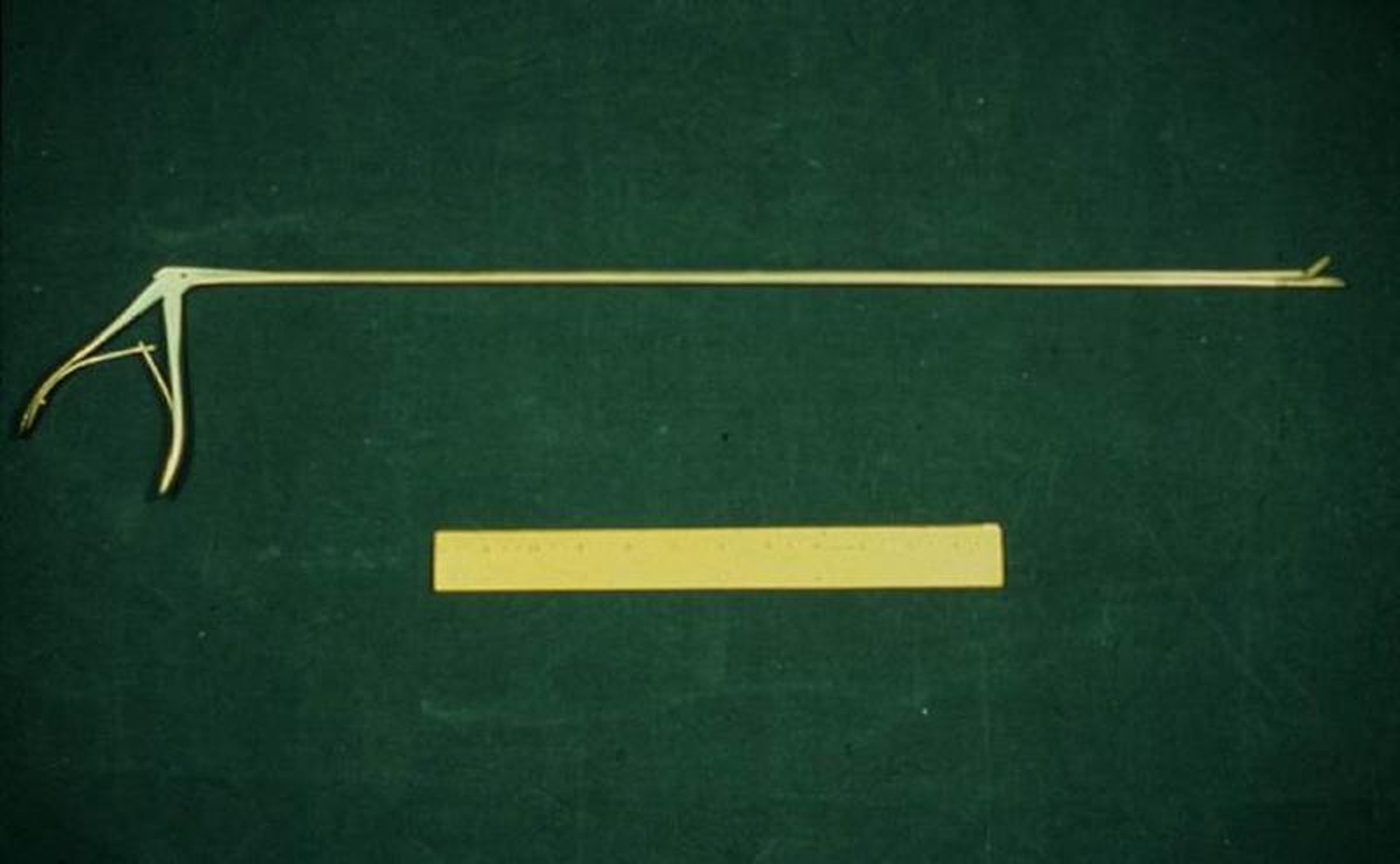
This biopsy instrument has a 65-cm shaft with a 2-cm sample basket.
Courtesy of Dr. Patricia Sertich.
An endometrial biopsy sample is usually obtained immediately after the endometrial culture samples have been procured. It should be kept in mind that manipulation of the endometrium can quickly cause a neutrophilic response in the endometrium. Preparation for biopsy is the same as for taking a swab (see above). The basket of the biopsy instrument should be kept closed during positioning to prevent accidental procurement of vagina, cervix, or examination glove. The instrument is manually guided with the gloved hand through the caudal genital tract into the uterine lumen. While keeping the instrument in place within the uterus with the nongloved (external) hand, the gloved hand is carefully withdrawn from the genital tract and inserted into the rectum to allow positioning of the basket of the biopsy instrument at the ventral luminal surface of the base of a uterine horn. The instrument jaws are then opened, the uterine wall is pressed into the side of the basket, which usually directs an endometrial fold into the basket, and the jaws are closed. The jaws should be kept closed while the instrument is withdrawn from the genital tract. The tissue should be gently teased from the basket and placed into Bouin’s fixative. If the sample will not be processed within a few days, it should be transferred into 70% ethanol or 10% formalin.
It is not unusual for a small amount of uterine bleeding to occur after biopsy. The biopsy procedure is not detrimental to fertility, and a mare can conceive from a breeding that occurred during an estrus when biopsy was performed.
Histologic evaluation of the endometrium provides prognostic information about the mare’s ability to carry a foal to term. The luminal contents may indicate the presence of uterine fluid or exudate. Epithelial cell height is related to hormone status; cells are cuboidal during anestrus and low to tall columnar during the breeding season. Transepithelial cells may indicate active inflammation. The pattern, character, and location of inflammation indicate the chronicity of response—neutrophils indicate an acute reaction, and lymphocytes and plasma cells indicate a chronic reaction. Focal or diffuse cellular distribution pattern, frequency of inflammatory cells, and degree of infiltration (slight to severe) relate to severity of inflammation. Histologic evidence of significant inflammation, combined with a report of growth of microorganisms from aerobic culture of endometrial swab and the presence of clinical signs of infection (uterine fluid, uterine discharge), support the decision that an endometrium would benefit from therapy to decrease inflammation.

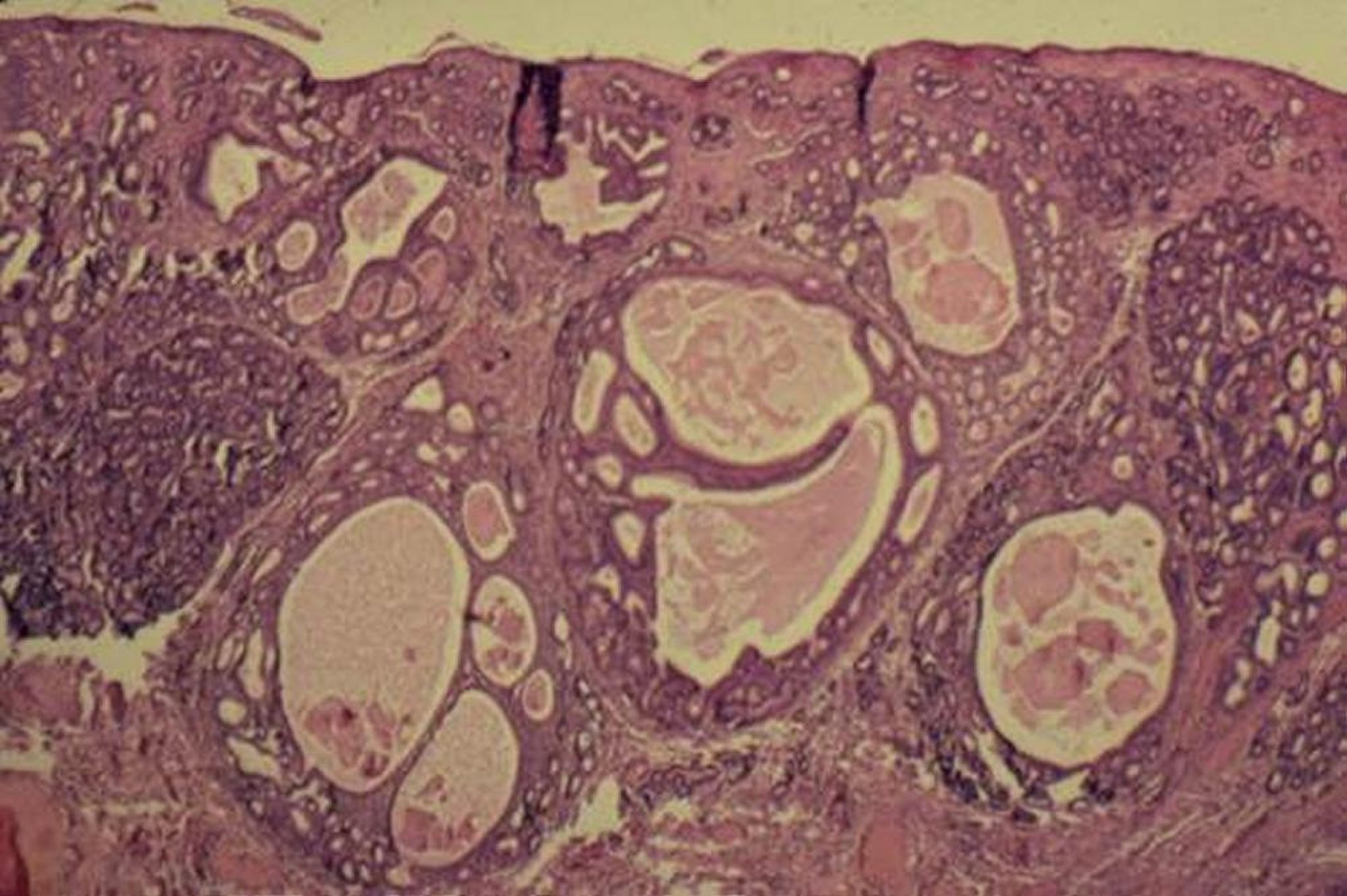
Periglandular fibrosis may contribute to cystic glandular distention, because it prevents the glands from releasing their secretions. There are 7 fibrotic nests in this field. This is a Category III endometrium.
Courtesy of Dr. Patricia Sertich.
Knowledge of the pattern of distribution and severity of periglandular fibrosis is prognostically useful. Fibrosis surrounding groups of glands (“fibrotic nest”) is thought to be more clinically significant than fibrosis of individual glands. Periglandular fibrosis may interfere with endometrial gland function and may be a factor causing early embryonic death. Glandular distention normally develops during pregnancy, but widespread cystic glandular distention in the nonpregnant mare is not normal. Cystic glandular distention is often associated with periglandular fibrosis and may result from an accumulation of gland secretions proximal to the occlusion of the endometrial gland by periglandular fibrosis.
Endometria are classified into 4 categories that attempt to predict its ability to carry a foal to term. Category I indicates no significant changes are present in the endometrium, and no treatment is required. The estimated foaling rate is 80%–90%. An endometrium with any notable periglandular fibrosis cannot be classified as Category I. Category II is a broad category that includes most mares. It has been divided into Category IIA, for mares with less severe changes, and Category IIB, for mares with more severe changes. The estimated foaling rate is 50%–80% in mares with Category IIA endometria and 10%–50% in mares with Category IIB endometria. Often, therapy may improve the state of the endometrium by reducing inflammation, cystic glandular distention, and lymphatic lacunae. Improvement in the endometrium may allow for better classification at a later date. There is no effective treatment to decrease the severity of periglandular fibrosis. Category III is the poorest classification, and these endometria have widespread, severe changes that include periglandular fibrosis or inflammation. The estimated foaling rate is < 10% in mares with Category III endometria. Keep in mind that a widespread pattern of distribution of slight to moderate changes may be more deleterious than more severe changes that are infrequent and only involve individual glands.
During interpretation of the findings on histologic evaluation of an endometrial biopsy sample, the extent of normal, unaffected endometrium is more significant than the presence of any particular lesion. In barren mares with a Category I or IIA endometrium, other reproductive abnormalities or poor breeding management should be investigated as the cause of infertility.
Vaginal Examination in the Breeding and Soundness Examination of the Mare

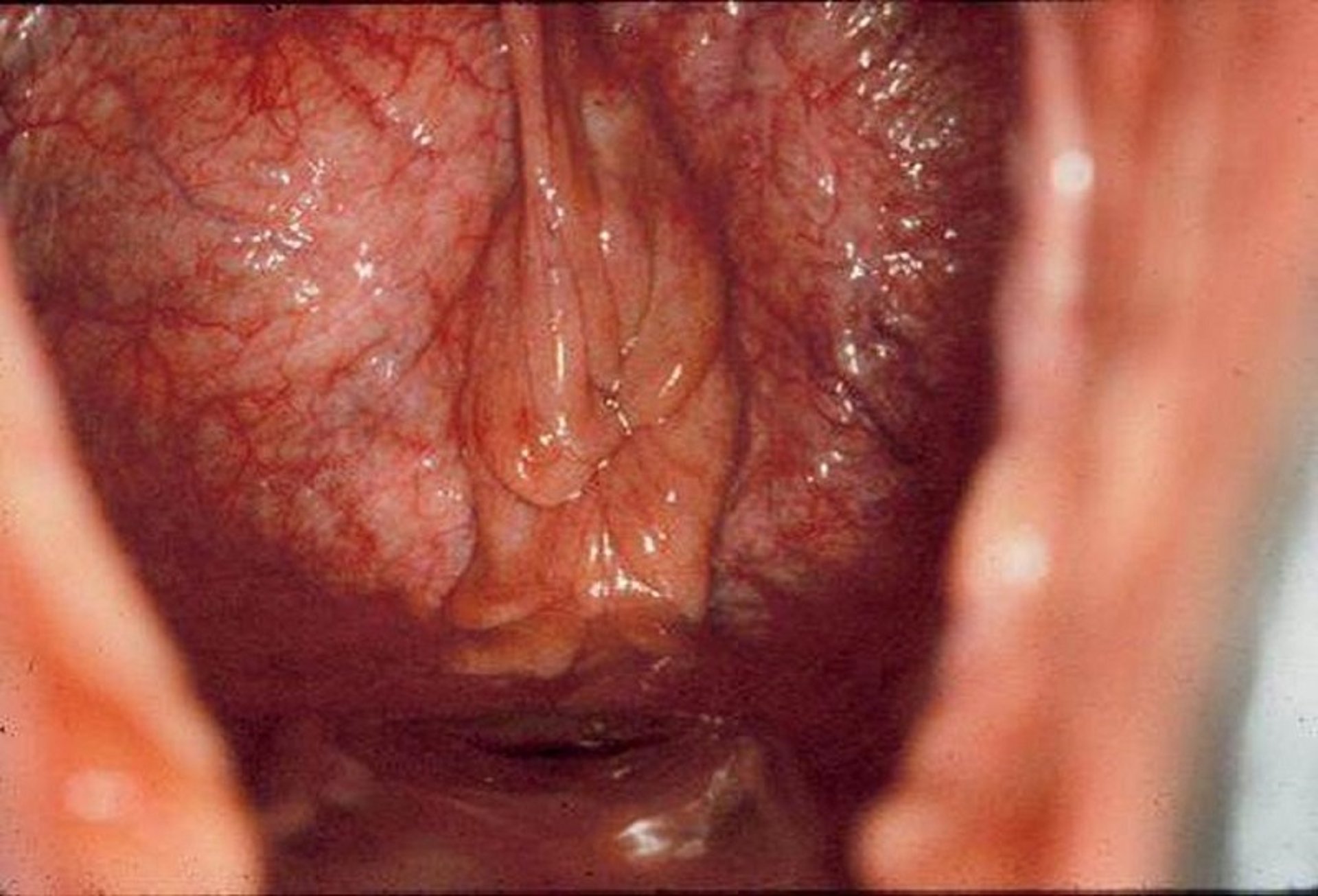
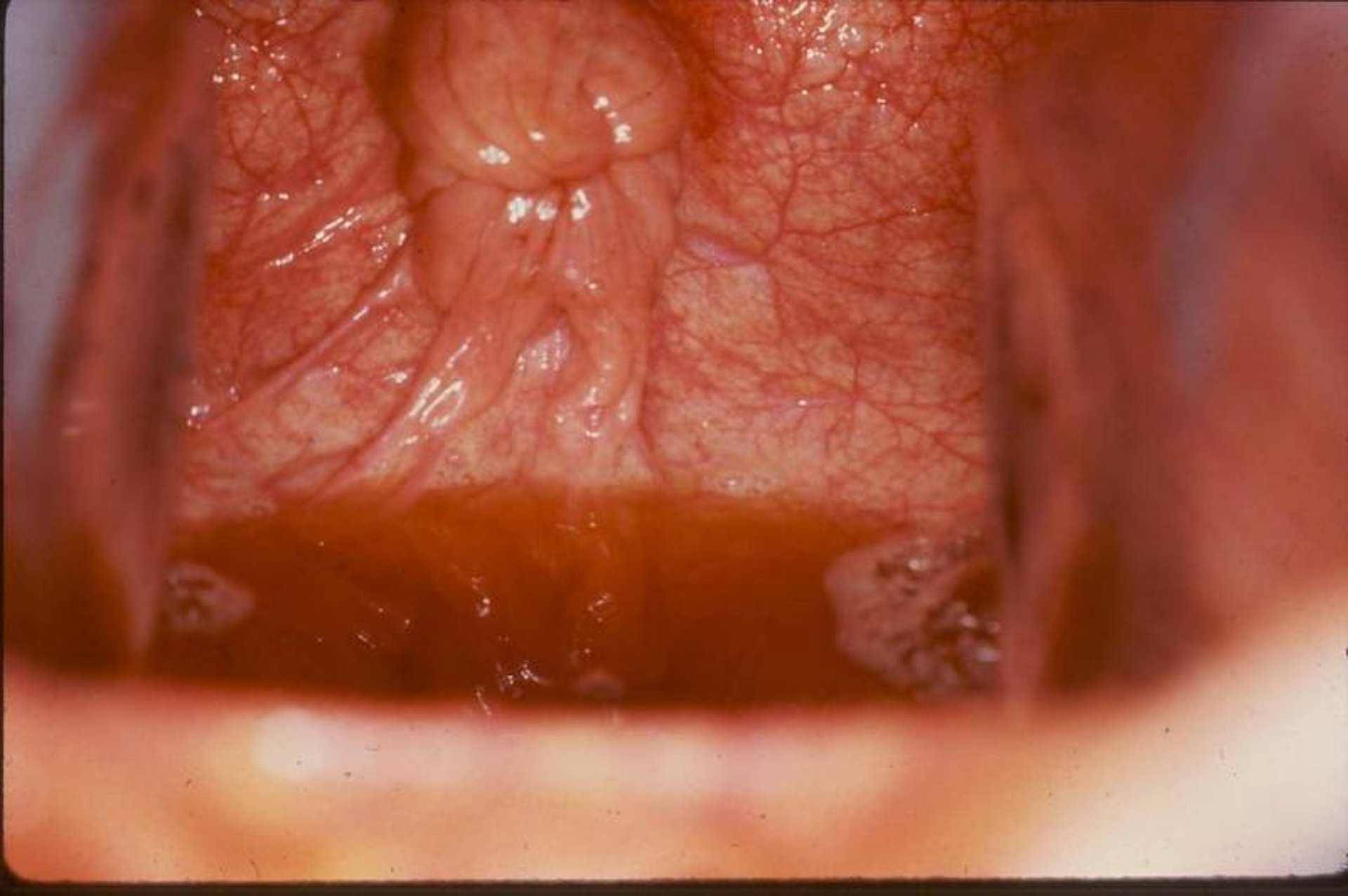
Visual examination of the cervix during estrus reveals it to be moist, hyperemic, and relaxed, which reflects the lack of progesterone and the presence of estrogen.
Courtesy of Dr. Patricia Sertich.
The perineum is cleansed, rinsed, and dried before the visual vaginal examination via speculum. The vulvar lips are separated, and the speculum is advanced cranially at a slight dorsal angle so as to pass over and through the transverse (vestibulovaginal) fold of the vagina. Resistance against the speculum by this fold of tissue indicates good tone and function. A bright light is necessary to adequately view the cervix and vaginal wall. The character of the cervix reflects the hormonal status of the mare. As the speculum is being withdrawn, it should be noted whether the vestibulovaginal fold occludes the vagina. The competency of the vestibulovaginal fold is important, because it forms the second barrier for the uterus against external contaminants.
Thorough evaluation of the completeness and competency of the cervix can be accomplished only by direct digital palpation per vagina while the mare is under endogenous or exogenous progesterone stimulation so that the cervix will be closed. The cervix forms the third barrier for the uterus against external contaminants.
For More Information
Also see pet health content regarding routine health care for horses.





