



Reports of uncomplicated nutrient deficiencies in horses are rare. Caloric intake, protein, and the nutrients calcium, phosphorus, copper, sodium chloride, and selenium, depending on age and type of horse and geographical area, are most likely to be deficient. Clinical signs of deficiency are frequently nonspecific, and diagnosis can be complicated by deficiencies of several nutrients simultaneously. Simple excesses are more common in some regions. Those nutrients most commonly given in excess of needs, leading to toxicity, metabolic disorders, or induced deficits of other nutrients, are phosphorus, iron, copper, selenium, and vitamin A. Overconditioning, as a result of excess dietary energy provision relative to caloric needs, is very common and also contributes to disease.
Energy Deficiency in Horses
Many nonspecific changes found in horses with caloric deficiency can result from inadequate intake, maldigestion, or malabsorption. Weight loss is the cardinal clinical sign of inadequate energy intake. In partial or complete starvation, most internal organs exhibit some atrophy. The brain is least affected, but growth, reproduction, and performance ability are most affected. The immune system is also adversely affected. The young skeleton is extremely sensitive, and growth slows or can completely stop. A decrease in adipose tissue is an early and conspicuous clinical sign and is observed not only in the subcutis but also in the mesentery; around the kidneys, uterus, and testes; and in the retroperitoneum (see ).


Lack of mesenteric fat accumulation in an emaciated horse.
Courtesy of Dr. Sarah Ralston
Low fat content of long-bone marrow is a good indicator of prolonged inanition. A severely restricted diet of less than 1.25% body weight (BW) dry matter (DM) (eg, for an obese horse on a weight loss diet) can result in hyperlipidemia, with ponies, donkeys, and miniature horses at higher risk than light breeds and draft horses (1).
Energy Excess in Horses
Overfeeding high-calorie feeds results in obesity and is a risk factor for insulin dysregulation (ID) in adult equids (see ). Overfeeding may contribute to developmental orthopedic disease in young, rapidly growing animals; however, some horses, especially those that are sedentary, can become obese on good-quality hay or pasture alone. Obesity increases the risk of metabolic disease and consequently the development of laminitis (presumably associated with relative insulin resistance).


Mesenteric fat accumulation in an obese horse.
Courtesy of Dr. Sarah Ralston.
A 2024 study of horses undergoing emergency laparotomy for colic suggested that both high body condition score (BCS) and confirmed metabolic disease carried a higher risk of having a strangulating lipoma (2). This is in line with earlier research, which concluded that horses with higher pituitary scores (≥ 3) and higher BCS had a greater frequency of mesenteric lipomas than horses with lower pituitary scores and BCS, regardless of insulin status (3). See .

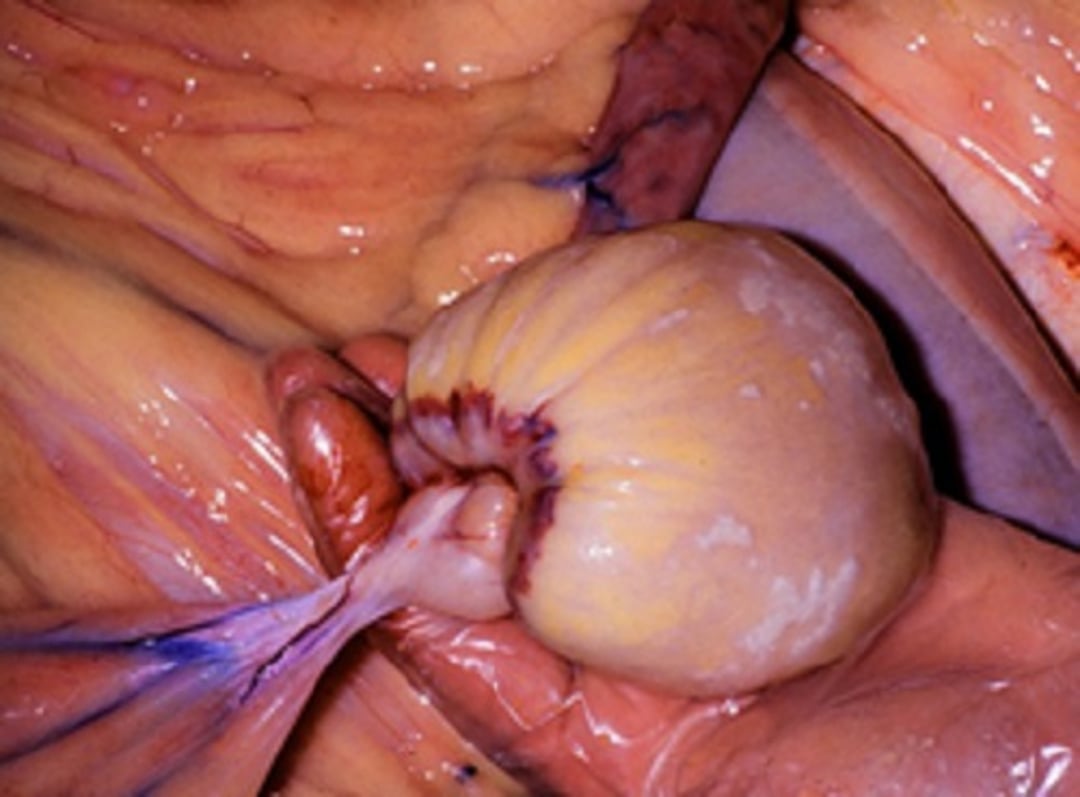
Pedunculated mesenteric lipoma in a horse.
Courtesy of Dr. Sarah Ralston.
Obese horses and ponies have decreased heat and exercise tolerance. Overweight and obese equids should be placed on a controlled calorie diet, which might necessitate the use of slow-feed hay nets, grazing muzzles, and a carefully managed exercise program, if soundness allows. When rations are restricted, it is important to maintain nutrient intake, often easily managed with an appropriate amount of a ration balancer. Starvation diets are not appropriate. Intake below 1.25% BW DM is not recommended.
Protein Deficiency in Horses and Other Equids
A deficiency of dietary protein can be caused by either inadequate intake or lack of a specific essential amino acid. The effects of deficiency are generally nonspecific, and many of the clinical signs do not differ from the effects of partial or total caloric restriction. In general, the horse will have a poor-quality haircoat and hoof growth, weight loss, muscle wasting, and inappetence (see ). Milk production is decreased in lactating mares, and rapidly growing foals will be stunted. Antibody formation is also decreased, which will affect immunity.


Horse suffering from protein/energy deficits. Note the dull haircoat.
Courtesy of Dr. Sarah Ralston.
Refeeding should be done carefully and can necessitate the supervision of a veterinarian depending on the severity. A qualified nutritionist should also be consulted to ensure proper diet balance and refeeding protocol.
Energy Excess in Donkeys
Overweight donkeys are at risk for laminitis and may develop calcified fat pads if obesity has been present over time. In general, obese donkeys still need clean, good quality straw (barley or wheat) as the majority of their diet. Short chopped forage can be fed if dentition is poor. Frequent, small meals are recommended, as is the use of a grazing muzzle to limit pasture intake. A ration balancer may be needed to ensure sufficient nutrient intake, but at a lower rate that what is fed to horses (~75% of horse/pony recommendation).
It is important not to starve or over-restrict the diet as this will put the donkey at risk for hyperlipemia. Concentrates and grain-based feeds along with high-sugar treats should be avoided. Weight loss will occur slowly, ideally around 5 kg per month for the average donkey [[Donkey Sanct overweight 2018]].
Weight tapes and equations suited for estimating weight in horses are not appropriate for estimating weight in donkeys. Equations specifically for use with donkeys have been developed[[Pearson 2000]], and are as follows, where heart girth is measured in cm around the body just behind the front legs, and length is measured from the pin bone (tuber ischii) to the elbow in a straight line in cm:
For an average, healthy weight donkey:
Live weight (kg) = (heart girth [cm]2.12) x (length [cm]0.688)/3801
For overweight donkeys:
Live weight (kg) = (heart girth [cm]2.575) x (height [cm]0.240)/3968
If the donkey is nervous or difficult to handle, one measurement can be used to estimate weight but it is less accurate:
Live weight (kg) = heart girth (cm)2.65/2188
A nomogram has been developed for estimating a donkey's weight as well, which requires the measurement of height and body length in centimeters.
Mineral Deficiencies and Excesses in Horses
Nutritional Secondary Hyperparathyroidism (Big Head, Bran Disease) in Horses
Nutritional secondary hyperparathyroidism (NSH) occurs as a result of sustained release of parathyroid hormone (PTH) in an effort to mobilize calcium from the bones as a result of dietary insufficiency. Bones of the head are most often visibly affected, as osteoid and fibrous tissue replaces mineral content of the facial bones and mandible (osteodystrophia fibrosa), hence the name "big head." Changes are bilateral but not necessarily symmetrical. Difficulty and pain while chewing occur as the disease progresses and can result in decreased food intake and weight loss (4).
Grass hay varieties vary in calcium and phosphorous content, depending on species, and can further vary by soil and other growing conditions. Mature warm-season grasses (eg, Bermuda grass, teff) tend to have lower Ca:P ratios (sometimes below 1:1), hence the recommendation to harvest these grasses before they reach maturity. Cool-season grasses tend to have a Ca:P ratio near 2:1, whereas legumes (eg, alfalfa) may be closer to 4:1 (and sometimes higher) (4). Note that the only way to know the mineral content of a forage is to have it tested by a forage-testing laboratory.
Horses of all ages fed mature grass hay or pasture of any variety and supplemented with large amounts of unfortified, grain-based concentrates (ie, corn, oats, barley) or wheat bran are most likely to develop relative or absolute calcium deficiencies leading to nutritional secondary hyperparathyroidism. Excess phosphorus intake and insufficient calcium intake (Ca:P ratio < 1) cause the same clinical signs. Blood concentrations of calcium do not reflect intake because of homeostatic mechanisms; however, blood inorganic phosphorus may be increased because of mobilization of bone mineral content. Swelling and softening of the facial bones and alternating limb lameness are frequently reported. Serum ALP activity is usually increased, and clotting time may be prolonged slightly. Fractures might occur, and wounds in general heal poorly.
Today, nutritional secondary hyperparathyroidism is not common, but diets with a reversed calcium:phosphorous ratio can cause lesion development. (Also see Osteomalacia in Animals.)
Developmental Orthopedic Disease in Horses
An imbalanced Ca:P ratio is a potential cause of some forms of developmental orthopedic disease (DOD). Copper deficiency may also contribute to osteochondrosis (OC) and/or physitis; however, research has reported mixed data. Per the NRC, appropriate copper supplementation of the pregnant dam, not the foal, may help decrease the incidence of DOD, and copper supplementation of the OC-affected foal may support repair of developing OC lesions. The role of diet in foal growth is complex, and much remains to be understood. In general, diets for growing animals should be formulated within recommended ranges according to the type and class of equid for which they are designed (4).
Excess dietary protein does not cause DOD. Rather, excess energy intake that leads to too-rapid growth has been shown to be a risk for development of DOD.
Phosphorus Deficiency in Horses
Phosphorus deficiency is most likely to occur in horses being fed poor-quality grass hay or pasture without grain, especially equids with higher needs (growing, lactating, performing). Serum inorganic phosphorus concentrations may be decreased, and serum ALP activity increased. Occasionally, serum calcium concentrations may be increased. An insidious shifting lameness may be present. Bone changes resemble those described for calcium deficiency. Affected horses may start to consume large quantities of soil or exhibit other manifestations of pica before other clinical signs are apparent.
Salt Deficiency in Horses
Horses are most likely to develop clinical signs of salt (NaCl) deficiency when worked hard in hot weather or fed salt-deficient rations. Heavily sweating and dehydrated horses given water without supplemental electrolytes can become even more dehydrated because drinking large quantities of plain water will cause a dilution of body fluids and inhibit the thirst mechanism. This situation also signals the kidneys to excrete water in an effort to increase the concentration of sodium. Without electrolytes, particularly NaCl, the body cannot hold on to water (5). Horses deprived of salt and other electrolytes tire easily, stop sweating, and exhibit muscle spasms if exercised strenuously. Anorexia and pica may be evident in chronic deprivation; however, these are not specific clinical signs of salt deficiency. In lactating mares, milk production declines. Polyuria/polydipsia secondary to renal medullary washout may occur in prolonged deficits.
Potassium Deficiency in Horses
Potassium is a major intracellular cation involved in acid-base balance and normal muscle function. Most potassium in the body is found in skeletal muscle. Chronic dietary deficiency of potassium results in a decreased rate of growth as well as anorexia and perhaps hypokalemia. However, most forages contain more than sufficient potassium for the average horse. Acute deficits due to sweat losses are more likely and may cause muscle tremors, cardiac arrhythmias, and weakness. Excess potassium intake has not been well studied in the horse; however, potassium given parenterally would be expected to cause cardiac arrhythmias such as atrial fibrillation and possibly cardiac arrest (4).
Horses with the genetic condition hyperkalemic periodic paralysis (HYPP) can be traced back to a Quarter Horse stallion and are sensitive to dietary potassium. From a nutritional standpoint, dietary potassium is recommended to be limited to 1% or less of the total diet for HYPP horses (4). Forages vary widely in potassium content, and a laboratory analysis is important for an accurate measurement. In general, grass hay contains less potassium than alfalfa and other legumes (4).Soaking hay can decrease potassium content; however, duration and water temperature will affect how much and how fast the decrease occurs. Hay soaked in cool tap water (22°C [72°F]) may take longer to draw out potassium than hay soaked in warm water (39°C [102°F]), and the amount of potassium lost may also depend on forage variety (6).
Magnesium Deficiency in Horses
Foals fed a purified diet containing magnesium at only 7–8 mg/kg (3.2–3.6 mg/pound)/day exhibited hypomagnesemia, nervousness, muscular tremors, and ataxia followed by collapse, with increased respiratory rates, sweating, convulsive paddling, and death after a few weeks. Hypomagnesemia causes mineralization in the aorta, and histological changes can occur within 30 days after starting a low-magnesium diet. However, most commonly used feeds contain magnesium well in excess of the 70–100 mg/kg dry ration currently recommended. Oversupplementation of this mineral is more likely.
Although the effects of excessive magnesium intake in horses have not been determined, according to data from other species, excess magnesium can cause clinical signs of calcium deficiency (4). The use of oral magnesium supplements for their calming effects has not yielded conclusive data in horses and could lead to excess dietary intake. Such supplementation should be done with caution.
Iron Deficiency in Horses
Iron deficiency is generally not of concern to young or mature equids with access to soil (including forages grown on it). Iron deficiency might be secondary to parasitism or chronic blood loss and results in microcytic, hypochromic anemia; however, it is highly unlikely that even anemic horses are iron-deficient. Iron excess interferes with copper metabolism and might contribute to hemochromatosis and hepatopathy (7). Iron in the form of ferrous fumarate is particularly toxic to young foals and can also harm mature animals. Injections of iron are dangerous to all horses and should be avoided (4). Blood transferrin concentrations are the most reliable method to determine the iron status of a horse.Iron supplements have not been shown to improve oxygen-carrying capacity of RBCs or hematopoiesis (4).
Pearls & Pitfalls
|
Zinc Deficiency in Horses
Zinc (Zn) deficiency in foals causes decreased growth rate, anorexia, cutaneous lesions on the lower extremities, alopecia, decreased blood concentration of zinc, and decreased serum ALP activity. Excesses (> 1,000 ppm) were associated with developmental orthopedic disease in young horses (4). Excessive zinc intake can interfere with proper copper (Cu) absorption (and therefore might contribute to DOD in young animals). The effects of excesses or deficits of zinc have not been documented in adult horses. Daily diets are typically formulated with a Zn:Cu ratio of 3:1–4:1 (4).
Copper Deficiency in Horses
Copper deficiency, or hypocupremia, has been associated with osteochondrosis and osteodysgenesis. Low copper intake in young, growing horses could play a role in the development of osteochondritis dissecans lesions, weak cartilage, and poor-quality collagen; however, other factors might also be involved (8). A decline in serum copper concentration may be associated with rupture of the uterine artery in aged parturient mares (4). However, serum copper concentrations might be of limited used in assessing overall copper status. Excessive copper intake may interfere with selenium and/or iron metabolism. Diets are typically formulated with a Zn:Cu ratio of 3:1 to 4:1 (4).
Selenium Deficiency in Horses
Selenium (Se) deficiency causes clinical signs of myopathy including weakness, impaired locomotion, difficulty in suckling and swallowing, respiratory distress, and impaired cardiac function. Serum changes associated with selenium deficiency include increases in CK, AST, potassium, and BUN. White muscle disease could also be a clinical sign of deficiency. Natural toxicosis is rare, and is more likely to occur with oversupplementation. The chemical form of selenium can affect toxicity, with organic selenium compounds found in plants (selenocystine and selenomethionine) the most highly toxic (4).
Horses are more sensitive than cattle to selenium toxicity. Acute toxicity (blind staggers) is characterized by apparent blindness, head pressing, sweating, colic, diarrhea, increased heart and respiration rates, and lethargy.Chronic toxicity is characterized by alopecia of the mane and tail and cracking or sloughing of the hooves, especially around the coronary band (4). Rapid deaths after the injection of toxic concentrations of selenium have occurred (9). For context, the NRC recommends an intake of 1 mg Se per day for an average 500-kg (1,100-pound) horse in light exercise.
Vitamin Deficiencies and Excesses in Horses
A vitamin A deficiency can develop if dried, poor-quality roughage is fed for a prolonged period (more than 6 months). If body stores of vitamin A are high, clinical signs might not appear for several months. Deficiency is characterized by the following clinical signs:
nyctalopia (night blindness)
lacrimation
keratinization of the cornea
susceptibility to pneumonia
abscesses of the sublingual gland
incoordination
impaired reproduction
capricious appetite
progressive weakness in adult horses
Hooves may be deformed, with the horny layer unevenly laid down and unusually brittle.
Vitamin A toxicity is associated with bone fragility, bone exostoses, skin lesions, and birth defects, such as cleft palate and micro-ophthalmia (according to data from both horses and other species). Excess vitamin A fed to pregnant mares is also implicated in birth defects, as well as in DOD in growing horses.
Natural vitamin E(d-alpha-tocopherol) is very labile and quickly lost during storage in both hays and commercial feeds. It is an important antioxidant, and deficiency has been reported to be associated with an increased incidence of muscle myopathies, impaired immune function, reproductive failure, and ocular lesions. Equine motor neuron disease is thought to occur after prolonged periods of vitamin E deficiency. Fresh forages, however, are excellent sources of vitamin E, and horses with free access to good pasture rarely need supplementation. Water-soluble forms of natural vitamin E are the most bioavailable form of supplement, followed by powdered forms, and are often recommended for horses with muscle myopathies or neurological conditions as part of a nutritional management program (10). Vitamin E does not appear to be toxic to horses; however, very high intakes (above 1,000 IU/kg DM) are not recommended and could interfere with absorption of other nutrients.
If sun-cured hay is consumed or the horse is exposed to sunlight, it is doubtful a vitamin D deficiency will develop. Prolonged confinement of young horses offered only limited amounts of sun-cured hay may result in decreased bone calcification, stiff and swollen joints, stiffness of gait, irritability, and decreased serum calcium and phosphorus. Clinical signs are easily reversible with supplementation or exposure to sunlight.
Clinical signs of experimental thiamine deficiency include anorexia, weight loss, incoordination, decreased blood thiamine, and increased blood pyruvate. At necropsy, the heart is dilated. Similar clinical signs have been observed in bracken fern poisoning. Under normal circumstances, the natural diet, plus synthesis by microorganisms in the gut, probably meets the need for thiamine. However, needs can be increased by stress. Thiamine toxicity does not seem likely because it is water-soluble, and toxicity has not been reported.
Key Points
Dietary insufficiency or excess can cause or contribute to health problems in equids.
Mineral balance is important for proper health, as is appropriate intake of vitamins.
Clinical signs of dietary imbalance can be nonspecific but should be considered in the evaluation of health status.
For More Information
Geor R, Harris P, Coenen M, eds. Equine Applied and Clinical Nutrition. Saunders; 2013.
Ellis A, Longland A, Coenen M, Miraglia N, eds. The Impact of Nutrition on the Health and Welfare of Horses. Brill Wageningen Academic; 2010.
References
Hughes K, Hodgson D, Dart A. Equine hyperlipaemia: a review. Aust Vet J. 2008;82(3):136-142. doi:10.1111/j.1751-0813.2004.tb12636.x
Gillen A, Hassel D, Gonzalez S, et al. Risk factors for equine strangulating lipoma: An international, multicentre unmatched case control study. Equine Vet Educ. 2024;36:S13. doi:10.1111/eve.63_14008
Newkirk KM, Chameroy K, Tardos E, Rohrbach B, Frank N. Pituitary lesions, obesity and mesenteric lipomas in insulin-resistant horses. Open J Vet Med. 2014;4(9):190-196. doi:10.4236/ojvm.2014.49022
Committee on Nutrient Requirements of Horses. Nutrient Requirements of Horses, 6th ed. National Research Council. National Academies Press; 2007. https://www.nationalacademies.org/publications/11653
Marlin D, Nankervis KJ. Thermoregulation. Equine Exercise Physiology. Blackwell Science; 2002:133-150.
Martinson KL, Hataway M, Jung H, Sheaffer C. The effect of soaking on protein and mineral loss in orchardgrass and alfalfa hay. J Equine Vet Sci. 2012;32(12):776-782. doi10.1016/j.jevs.2012.03.007
Theelen MJP, Beukers M, Grinwis GCM, Sloet van Oldruitenborgh-Oosterbaan MM.Chronic iron overload causing haemochromatosis and hepatopathy in 21 horses and one donkey. Equine Vet J. 2019;51(3):304-309. doi:10.1111/evj.13029
Hurtig M, Green SL, Dobson H, Mikuni-Takagaki Y, Choi J. Correlative study of defective cartilage and bone growth in foals fed a low-copper diet. Equine Vet J. 1993;25(S16):66-73. doi:10.1111/j.2042-3306.1993.tb04857.x
Desta B, Maldonado G, Reid H, et al. Acute selenium toxicosis in polo ponies. J Vet Diagn Invest. 2011;23(3):623-628. doi:10.1177/1040638711404142
Pagan J, Lennox M, Perry L, et al. Form of alpha-tocopherol affects vitamin E bioavailability in Thoroughbred horses. Proceedings of the First Nordic Feed Science Conference. 2010. https://ker.com/published/form-of-alpha-tocopherol-affects-vitamin-e-bioavailability-in-thoroughbred-horses/





