



The most common uroliths in dogs are struvite, calcium oxalate, and urate (see ). Less common uroliths include cystine, silica, calcium phosphate, and xanthine.

Struvite Stones in Dogs
Calcium oxalate and struvite are the most common stone types in dogs (see and images). The mineral composition of struvite stones is mostly magnesium ammonium phosphate hexahydrate (MgNH4PO4 • 6H2O); however, small amounts of other minerals are often present.


Gross pathology of a struvite stone from a dog. Note the smooth, round appearance of the stone.
Courtesy of Ontario Veterinary College.


Gross pathology of struvite calculi removed from the urinary bladder. Note the smooth, round, or faceted appearance of the stones.
Courtesy of Ontario Veterinary College.
In most cases, struvite uroliths form in association with urinary tract infections caused by urease-producing Staphylococcus or Proteus bacteria. Struvite stones can also form in the absence of infection.
Although they are common in cats, sterile struvite uroliths rarely form in dogs. They have been detected in a family of English Cocker Spaniels (1), suggesting a genetic predisposition, as well as in male Pugs. Sterile struvite uroliths can also form because of urine composition altered by renal tubular acidosis.
Struvite uroliths in dogs are amenable to medical dissolution, which involves feeding a prescription struvite dissolution diet. These diets have lower amounts of protein, magnesium, and phosphorus to decrease urinary excretion of ammonium, magnesium, and phosphorus. They also promote urinary acidification and have added sodium to increase water consumption. Supplementing water and/or feeding a diet high in moisture content also decreases the concentration of struvite components in the urine.
In some cases (eg, owner noncompliance or dog intolerance of diet), medical dissolution of struvite uroliths is not possible. Contraindications to medical dissolution include urethral obstruction and disease processes such as hyperlipidemia or pancreatitis, for which prescription dissolution diets are not appropriate. In these cases, other methods of stone removal, such as surgery or lithotripsy, can be performed.
Before beginning medical stone dissolution, physical examination, CBC, serum chemical profile, urinalysis, urine culture and susceptibility, and abdominal radiography to document stone size should be performed.
Dissolution Protocol for Struvite Stones
Dissolution of infection-induced struvite stones in dogs involves concurrent treatment with an antimicrobial and administration of a struvite dissolution diet. No other food, including treats, should be fed, and adequate fresh water should always be available.
The choice of antimicrobial should be based on susceptibility testing when possible. Concurrent treatment with a urease inhibitor such as acetohydroxamic acid has been described in dogs (2); however, it is not typically necessary and not recommended as part of first-line therapy.
After approximately 4 weeks of treatment, physical examination, serum chemical profile, urinalysis, and abdominal radiography or ultrasonography should be repeated. The stone dissolution protocol should be discontinued if severe adverse effects develop.
With good compliance, the following results can be anticipated: urine pH < 6.5, urine specific gravity < 1.025, serum urea < 10 mg/dL.
The stone size on radiographs should be compared with the size on previous radiographs. Stones that fail to decrease in size after 1–2 months of treatment are probably not composed of struvite and should be treated another way.
Complete dissolution of struvite cystoliths in dogs takes 1–2 months, on average, but can take longer. Traditionally, continuing the dissolution diet and antimicrobial therapy for 2–4 weeks past radiographic resolution of the stones has been recommended; however, little evidence supports this approach, and a shorter duration of antimicrobial therapy might be effective.
Renal stones tend to dissolve more slowly than bladder stones; however, successful dissolution of infection-induced nephroliths and uroliths has been described.
Sterile struvite uroliths are dissolved in the same way as infection-induced struvite stones, except that antimicrobial therapy is not necessary and dissolution can occur faster.
Prevention Protocol for Struvite Stones
Struvite urolithiasis in dogs can recur in both infection-induced and sterile cases. With infection-induced cases, recurrence typically results from incomplete dissolution or removal of stones and/or recurrent urinary tract infection with urease-producing bacteria. Addressing the underlying cause(s) of urinary tract infection and carefully monitoring for recurrence are indicated. Long-term dietary management after the infection has resolved is not indicated.
Sterile struvite uroliths in dogs are more likely to recur than infection-induced stones, because the underlying cause is not completely understood and persists after successful dissolution or removal of stones. Some prescription diets are formulated for long-term feeding to discourage recurrence of struvite stones; however, data on their efficacy are lacking.
Dogs predisposed to struvite stones should ideally have a urine pH of 6–6.5 and a urine specific gravity of < 1.020 to discourage precipitation of struvite.
Calcium Oxalate Stones in Dogs
Along with struvite, calcium oxalate is the most common stone type in dogs.
Although calcium oxalate stones can be found in any dog breed, numerous small breeds (Miniature Schnauzer, Chihuahua, Bichon Frise, Yorkshire Terrier, Shih Tzu, Lhasa Apso, and others) are more commonly affected.
Calcium oxalate stones tend to form in middle-aged to older dogs, but juvenile dogs can also be affected.
The etiology of calcium oxalate urolith formation remains unclear; however, disorders that cause increased urinary calcium excretion, genetic factors, and dietary factors all might play a role.
Workup of dogs with confirmed (or suspected) calcium oxalate stones should include evaluation for correctable underlying metabolic disorders that might increase urinary calcium excretion, such as hypercalcemia, hyperadrenocorticism, and primary hyperparathyroidism. In addition, these dogs should be evaluated for common comorbid conditions, such as chronic kidney disease and heart disease, that can affect treatment and prevention strategies.
Calcium oxalate uroliths in dogs are not amenable to medical dissolution and must be mechanically removed.
Prevention Protocol for Calcium Oxalate Stones
Recurrence is a major problem with calcium oxalate uroliths in dogs. It is difficult to prevent their formation because the etiology is incompletely understood. Although preventive measures should be implemented in dogs that form calcium oxalate stones, recurrence should be expected, because preventive strategies are intended to slow the rate of recurrence, slow further development of existing calcium oxalate uroliths, and potentially facilitate early detection of recurrence for easier noninvasive removal.
When possible, reversible predisposing factors like hypercalcemia should be addressed. Additional modifications aimed at making the urine composition inhospitable for precipitation of calcium oxalate components can be attempted. Numerous prescription diets are available for prevention of calcium oxalate stones in dogs; dietary factors that discourage calcium oxalate stone formation include decreased dietary protein, decreased calcium, and decreased sodium.
In straightforward cases of calcium oxalate uroliths, feeding a canned urinary prescription diet is recommended; however, the nutritional requirements of any comorbid conditions must be considered as well. As with all dogs that form stones, consumption of a high-moisture diet is recommended to decrease urine concentration.
For prevention of calcium oxalate uroliths in dogs, urine should ideally be maintained at pH 6.5–7.5 and specific gravity < 1.020.
Potassium citrate (75 mg/kg, PO, every 12 hours, increased incrementally as needed to reach target urine pH) can be added to help alkalinize the urine; furthermore, citrate is a chelator of calcium.
Hydrochlorothiazide (2 mg/kg, PO, every 12 hours) can also be added for recurrent calcium oxalate stone formation when dietary therapy is ineffective, because it decreases the excretion of calcium in the urine.
Dogs that have a high risk of calcium oxalate stones or a history of frequent recurrence should be monitored with radiography every 3–6 months to check for recurrence and potentially identify stones when they are small enough to be removed via voiding urohydropropulsion, thereby avoiding future surgeries and the associated risk of stone recurrence triggered by intraluminal suture.
Pearls & Pitfalls
|
It has also been suggested that dogs with recurrent uroliths that are not showing clinical signs should be monitored for future problems (obstruction, lower urinary tract signs, urinary tract infection). If they do not develop clinical signs, the uroliths should be left in place to avoid frequent, expensive removal procedures.
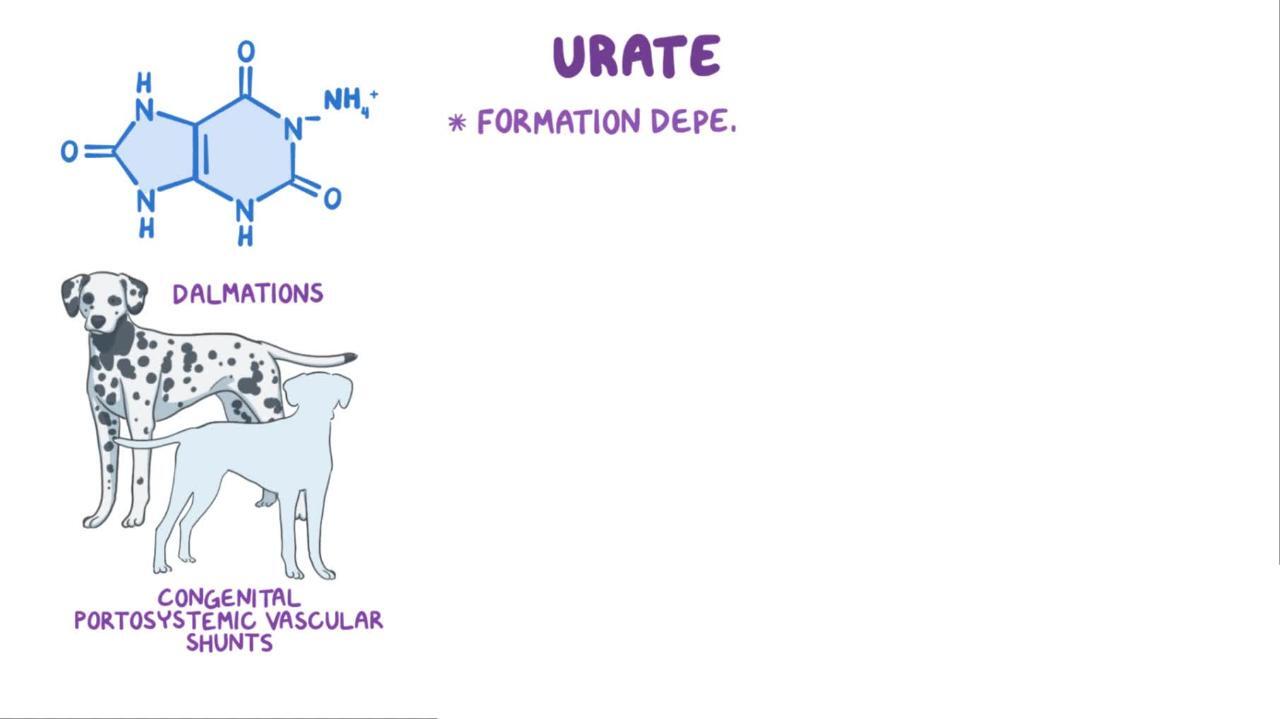
Urate Stones in Dogs
Urate stones (most commonly ammonium urate) are the third-most-common stone type found in dogs (see image).


Gross pathology of a urate bladder stone from a 5-year-old Dalmatian. Note the smooth, oval appearance of the stone.
Courtesy of Ontario Veterinary College.
There are two major etiologies to consider in dogs with urate stones: a congenital error of metabolism resulting in excessive excretion of uric acid in the urine (hyperuricosuria) and congenital portovascular anomalies.
In most dogs, uric acid, a product of purine metabolism, is converted to allantoin in the liver; allantoin is soluble and excreted in the urine. This conversion is decreased in Dalmatians, and they excrete most nucleic acid metabolites as relatively insoluble urate (see ).


Intraoperative photograph of a 5-year-old Dalmatian undergoing urethrostomy because of urethral calculi.
Courtesy of Ontario Veterinary College.
A mutation of a gene that encodes for a uric acid transporter (SLC2A9) has been found in Dalmatians with hyperuricosuria, as well as in some English Bulldogs and Black Russian Terriers (3).
In dogs with a portovascular anomaly, increased urinary ammonium output can be due in part to the increased filtered load of ammonia in these animals. When urate uroliths are identified in any breed not known to be predisposed to hyperuricosuria, investigation for portosystemic shunt, including serum bile acids, should be performed.
Pearls & Pitfalls
|
Dissolution Protocol for Urate Stones
Dissolution of urate uroliths that are not a result of liver disease can be attempted in dogs. Key components of a successful dissolution protocol include increasing urate solubility by raising urine pH to > 7, increasing dietary water content, and feeding a low-purine diet.
The xanthine oxidase inhibitor allopurinol (15 mg/kg, PO, every 12 hours for 4 weeks) can be added; however, strict adherence to a low-purine diet must be maintained to prevent the formation of xanthine uroliths.
Complete dissolution of urate uroliths has been reported to be successful approximately half the time in Dalmatians, occurring in approximately 1 month (4).
Prevention Protocol for Urate Stones
Urate stones are highly recurrent in dogs with hyperuricosuria, and prevention strategies should be implemented to minimize the recurrence rate.
Feeding a low-purine diet with or without supplemental potassium citrate to alkalinize the urine discourages the formation of new stones.
When dietary management alone is inadequate for preventing the formation of urate stones in dogs, a low dose of allopurinol can be administered (5–7 mg/kg, PO, every 12–24 hours long-term as needed); however, xanthine stone formation is still a risk.
As with calcium oxalate stone formers, dogs that form urate stones and have a history of frequent recurrence can be monitored periodically with abdominal imaging to allow the opportunity for voiding urohydropropulsion before the stones grow too large.
Cystine Stones in Dogs
Stones composed almost entirely of cystine form in dogs that have a renal tubular amino acid reabsorption defect known as cystinuria. Healthy dogs demonstrate 97% fractional reabsorption of cystine; affected dogs excrete a much greater proportion of the filtered cystine load and might even exhibit net cystine secretion.
Cystine is a relatively insoluble amino acid; therefore, in high concentrations it can precipitate and form stones. Identification of cystine crystals by urinalysis in a dog indicates a risk of forming cystine uroliths.
Cystine stones are uncommon in dogs, but they occur in breeds affected by cystinuria, including English Bulldogs, Mastiffs, French Bulldogs, Newfoundlands, and others. The vast majority of cystine stones are recovered from younger, intact male dogs.
Dissolution and Prevention Protocols for Cystine Stones
Cystine uroliths in dogs can be medically dissolved. A decreased-protein, canned, alkalinizing prescription diet is ideal, along with administration of 2-mercaptopropionylgylcine (2-MPG), or tiopronin (15–20 mg/kg, PO, every 12 hours until dissolution of the stones [1–3 months]).
To prevent cystine stone formation in dogs, the urine should be alkalinized to pH > 7.5, so additional alkalinization with potassium citrate can be included, if necessary. Because some cases of cystinuria are androgen dependent, neutering is recommended to prevent recurrence when cystine stones are identified in male dogs. In other cases, cystinuria is a lifelong defect of tubular reabsorption and cannot be cured.
Pearls & Pitfalls
|
Cystine stones in dogs tend to recur within 1 year if not managed to prevent recurrence, and they often recur despite attempts at prevention.
Silica Stones in Dogs
Early reports indicated a predominance of silica stones in German Shepherd Dogs, but many breeds have now been implicated. In males, urethral obstruction is the most common presenting problem; however, clinical signs similar to those associated with other types of uroliths also might be noted.
The mean age at occurrence of silica stones in dogs is approximately 6 years.
Silica stones in dogs are usually multiple and develop in the bladder and urethra. Silica uroliths are radiopaque. Frequently they have a characteristic “jackstone” appearance (characterized by a central dense core with a spiculated contour, resembling a toy jack). Identification requires spectrographic analysis and cannot be made with kits for qualitative stone analysis.
The role of diet in spontaneously occurring silica urolithiasis in dogs has not been determined; however, plants are often an abundant source of silica. If the diet of an affected dog is known to be high in silica, or if silica urolithiasis has been recurrent, a dietary change should be recommended.
Only general management principles can be suggested for preventing silicate urolithiasis in dogs. Additional salt and/or water should be included in the diet to induce diuresis and to lower the urine solute concentration. When present, urinary tract infections should be eliminated. Diets high in plant proteins should be avoided.
Key Points
Calcium oxalate and struvite are the most common urolith types found in dogs.
Struvite uroliths in dogs are most often the result of infection with a urease-producing bacterial organism.
Struvite stones can be dissolved medically by treatment of the urinary tract infection, combined with feeding a struvite dissolution diet.
Calcium oxalate stones cannot be removed via medical dissolution and are highly recurrent.
Prevention of calcium oxalate stone formation involves treating causes of hypercalciuria, when possible, along with dietary and medical management.
Urate stones in dogs are caused by either a congenital error of metabolism or a portovascular anomaly.
For More Information
Lulich JP, Berent AC, Adams LG, Westropp JL, Bartges JW, Osborne CA. ACVIM Small Animal Consensus Recommendations on the Treatment and Prevention of Uroliths in Dogs and Cats. J Vet Intern Med. 2016;30(5):1564-1574.
Bartges JW, Callens AJ. Urolithiasis. Vet Clin North Am Small Anim Pract. 2015;45(4):747-768.
Queau Y. Nutritional management of urolithiasis. Vet Clin North Am Small Anim Pract. 2019;49(2):175-186.
Allen HS, Swecker WS, Becvarova I, Weeth LP, Werre SR. Associations of diet and breed with recurrence of calcium oxalate cystic calculi in dogs. J Am Vet Med Assoc. 2015;246(10):1098-1103.
Wingert AM, Murray OA, Lulich JP, Hoelmer AM, Merkel LK, Furrow E. Efficacy of medical dissolution for suspected struvite cystoliths in dogs. J Vet Intern Med. 2021;35(5):2287-2295. doi:10.1111/jvim.16252
Also see pet owner content regarding urinary stones in dogs.
References
Bartges JW, Osborne CA, Polzin DJ. Recurrent sterile struvite urocystolithiasis in three related English cocker spaniels. J Am Anim Hosp Assoc. 1992;28(5):459–469.
Krawiec DR, Osborne CA, Leininger JR, Griffith DP. Effect of acetohydroxamic acid on dissolution of canine struvite uroliths. Am J Vet Res. 1984;45(7):1266-1275. doi:10.2460/ajvr.1984.45.07.1266
Bannasch D, Safra N, Young A, Karmi N, Schaible RS, Ling GV. Mutations in the SLC2A9 gene cause hyperuricosuria and hyperuricemia in the dog. PLoS Genet. 2008;4(11):e1000246. doi:10.1371/journal.pgen.1000246
Bartges JW, Osborne CA, Lulich JP, et al. Canine urate urolithiasis: etiopathogenesis, diagnosis, and management. Vet Clin North Am Small Anim Pract. 1999;29(1):161-191. doi:10.1016/s0195-5616(99)50010-7





