

Prostatic diseases in small animals include benign prostatic hyperplasia, bacterial prostatitis (acute and chronic), prostatic cysts and abscesses, and prostatic metaplasia and neoplasia. Disease of the prostate can be inapparent or cause urinary, GI, and musculoskeletal signs. Evaluation of prostatic fluid, as well as ultrasonographic size and echotexture of the prostate, will yield a definitive diagnosis in most cases. Many prostatic diseases are androgen-dependent, so eliminating (eg, by castration or finasteride) the source of androgens is indicated in most cases.
Disease of the prostate gland is common in sexually intact male dogs but rare in cats and other domestic animal species.
Benign prostatic hyperplasia (BPH) is by far the most common disease of the prostate in sexually intact male dogs and has not been reported in cats. Bacterial prostatitis (acute or chronic), intraprostatic and paraprostatic cysts, prostatic abscesses, prostatic squamous metaplasia, and prostatic adenocarcinoma are observed much less frequently and can occur in castrated male dogs.
When prostatic calculi occur in dogs (rarely), there is usually some other prostatic disease as well. Radiopaque prostatic calculi are rare incidental findings on abdominal radiographs.
Although both acute and chronic bacterial prostatitis have been reported in cats, prostate tumors are exceedingly rare, and there have only been singular case reports of prostatic squamous metaplasia and paraprostatic cysts.
Depending on the prostatic disorder, clinical signs may include the following:
intermittent hematuria
recurrent urinary tract infections
caudal abdominal discomfort
tenesmus
However, many sexually intact male dogs with BPH (with or without chronic prostatitis) are clinically normal or develop clinical signs of hemospermia and/or infertility only.
For acute bacterial prostatitis, prostatic abscesses, or prostatic neoplasia, nonspecific clinical signs (eg, fever, malaise, anorexia, severe stiffness, and caudal abdominal pain) can occur. Prostatic adenocarcinoma with bony involvement of the pelvis and lumbar vertebrae may cause hindlimb gait abnormalities. Less commonly, prostatic diseases may cause urinary incontinence. Prostatic adenocarcinoma may cause complete urethral obstruction.
In cases of suspected prostatic disease, physical examination should include abdominal and rectal palpation. An enlarged prostate typically is located farther cranial than usual and can be found in the caudal abdomen rather than within the pelvic canal. Simultaneous abdominal and rectal palpation allow not only for the cranial aspects of the prostate to be palpated but also for better palpation per rectum, because the prostate can be pushed into or near the pelvic canal, which is especially important in large-breed dogs and in males with very enlarged prostates.
Size, shape, symmetry, consistency, mobility, and presence or absence of pain can be assessed by palpation of the prostate gland. The normal dorsal sulcus (depression) aids in assessment of shape and symmetry.
More than 90% of protein secreted in prostatic fluid is canine prostatic-specific esterase, an arginine esterase found mainly on the apical regional of prostatic secretory epithelial cells. Canine prostatic-specific esterase has increased serum concentrations with all forms of prostate disease but is not notably different across BPH, prostatitis, and neoplasia.
Abdominal radiographs may help define the size, shape, and position of the prostate gland (see ). The sublumbar lymph nodes, lumbar vertebrae, and bony pelvis should be evaluated radiographically for evidence of periosteal new bone and bony metastases, which can be seen with neoplasia of the prostate.


Lateral radiographic view in a dog with prostatomegaly. In the caudal ventral abdomen, the enlarged prostate appears caudal to the bladder and is approximately half the size of the bladder with a similar radiographic density and shape (giving the illusion of a double bladder).
Courtesy of Dr. Ronald Green.
A positive-contrast retrograde urethrogram can be performed when an abnormal prostate or paraprostatic cyst is difficult to differentiate from the bladder.
Transabdominal ultrasonography is the best imaging modality for evaluating the prostate, because it allows the prostatic parenchyma and adjacent soft tissue structures to be visualized (see ).

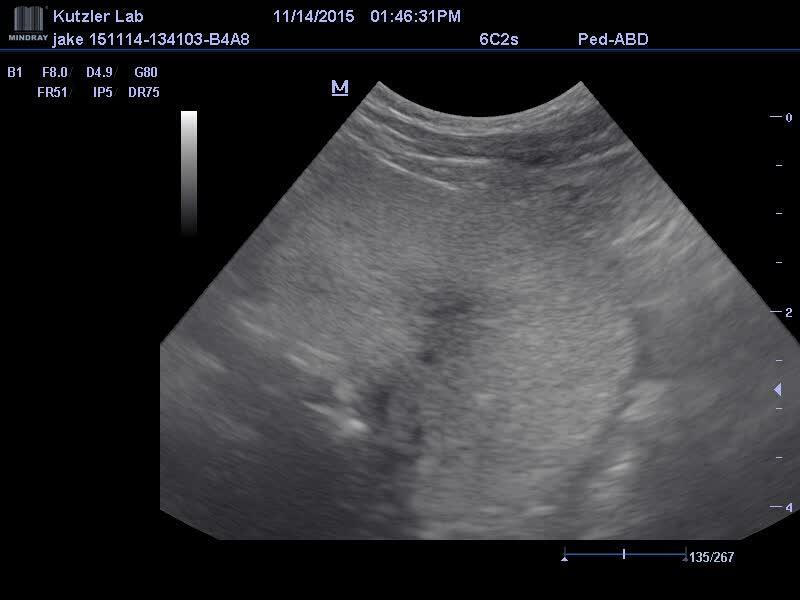
Intraprostatic cysts appear as anechoic areas within the prostatic parenchyma. Increased echogenicity (see ) is associated with BPH, chronic bacterial prostatitis, and prostatic neoplasia, whereas areas of mineralization may be secondary to chronic bacterial prostatitis or prostatic neoplasia. Mass lesions within the prostatic urethra and discontinuity of the prostatic urethral wall are both highly suggestive of prostatic neoplasia.

Ultrasonographic views of the parenchyma of the right (A) and left (B) prostatic lobes of a dog with prostatitis. Note the focal to multifocal areas of increased echogenicity (yellow arrows) indicative of prostatic inflammation, which can be associated with benign prostatic hyperplasia, chronic bacterial prostatitis, and prostatic neoplasia.
Courtesy of Dr. Michelle Kutzler.
The best way to obtain a representative sample of prostatic fluid for cytological evaluation and culture is by manual ejaculation of the dog (see ) and separate collection of the third (prostatic) fraction of the ejaculate into a sterile container.

If the dog will not ejaculate, material for cytological and microbiological examination can be obtained by prostatic massage and wash:
Using aseptic technique, catheterize the bladder and remove all urine.
Flush the bladder with saline solution (0.9% NaCl) and save the sample (prewash specimen).
Withdraw the catheter so that the end is caudal to the prostate.
Massage the prostate per rectum for about 1 minute to release prostatic fluid into the urethra, where the catheter can collect it.
While occluding the urethral opening, slowly inject saline solution.
Advance the catheter into the bladder as aspiration is performed, and collect another sample (prostatic wash specimen).
Results of cytological and microbiological examination from both the prewash and prostatic wash specimens should be compared.
Prostatic massage is contraindicated in dogs with acute bacterial prostatitis or a prostatic abscess because postprocedural septicemia has been reported. In addition, a limitation of prostatic wash is that neoplastic cells are often not recovered in these specimens.
Fine-needle aspiration of the prostate gland can be performed transrectally or percutaneously, with or without ultrasonographic guidance. Although generally safe and simple, this procedure carries some risk of penetration of surrounding structures and iatrogenic peritonitis.
Prostatic biopsy is the most definitive, but also the most invasive, diagnostic procedure to differentiate prostatic diseases. To obtain diagnostic samples, a prostatic biopsy should be performed via celiotomy or by a skilled ultrasonographer.
Alternatively, if a prostatic urethral transitional cell carcinoma is suspected, a catheter biopsy of the prostate can be performed with minimal chemical restraint:
Select the largest-bore catheter (with side holes) that can be advanced into the urethra.
Catheterize the bladder and empty it of urine.
Attach the catheter to a 12-mL syringe filled with 3–10 mL of saline solution (0.9% NaCl) and guide it to the level of the lesion as indicated by radiographs or ultrasonographic evaluation, or by a finger inserted in the rectum.
With a finger in the rectum, push the lesion ventrally against the urinary catheter.
Apply negative pressure by retracting the syringe plunger, and rapidly move the catheter back and forth over a short distance to secure a piece of tissue.
Gradually release the negative pressure and withdraw the catheter.
If the lesion involves the prostate gland, it should be massaged rectally before and during the aspiration phase. Tissue pieces are fixed in 10% neutral-buffered formalin and evaluated histologically. Slides are made of the remaining liquid portion of the sample and examined cytologically.
Key Points
Diseases of the prostate gland are relatively common in intact dogs but rare in cats and neutered dogs.
Prostate diseases include benign prostatitic hyperplasia, bacterial prostatitis (acute and chronic), and prostatic cysts and abscesses, as well as prostatic metaplasia and neoplasia.
Prostatic diseases can be inapparent or cause urinary, GI, and musculoskeletal signs.
Evaluation of prostatic fluid, as well as ultrasonographic size and echotexture of the prostate, yields a diagnosis in most cases of prostatic disease.
Many prostatic diseases are androgen-dependent, so eliminating (eg, via castration or finasteride) the source of androgens is indicated in most cases.
For More Information
Palmieri C, Fonseca-Alves CE, Laufer-Amorim R. A review on canine and feline prostate pathology. Front Vet Sci. 2022;9:881232.
Freitag T, Jerram RM, Walker AM, Warman CG. Surgical management of common canine prostatic conditions. Compend Contin Educ Vet. 2007;29(11):656-673.
Also see pet owner content regarding prostatic diseases in dogs and prostatic diseases in cats.





